Article Text

Statistics from Altmetric.com
Case presentation
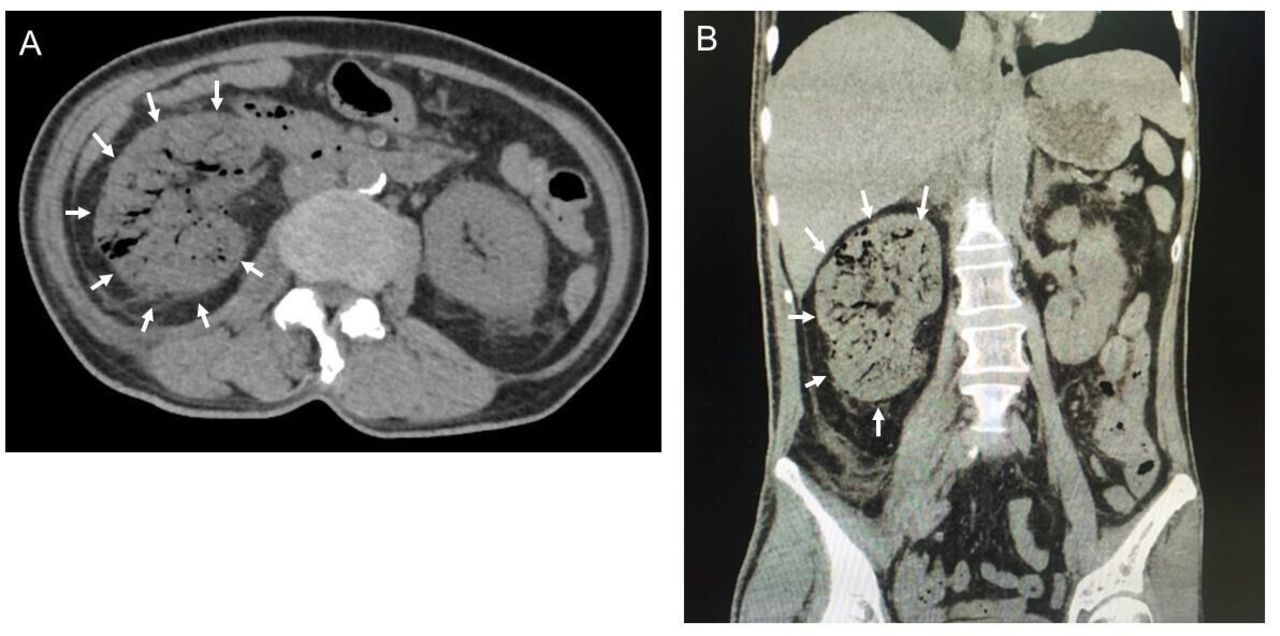
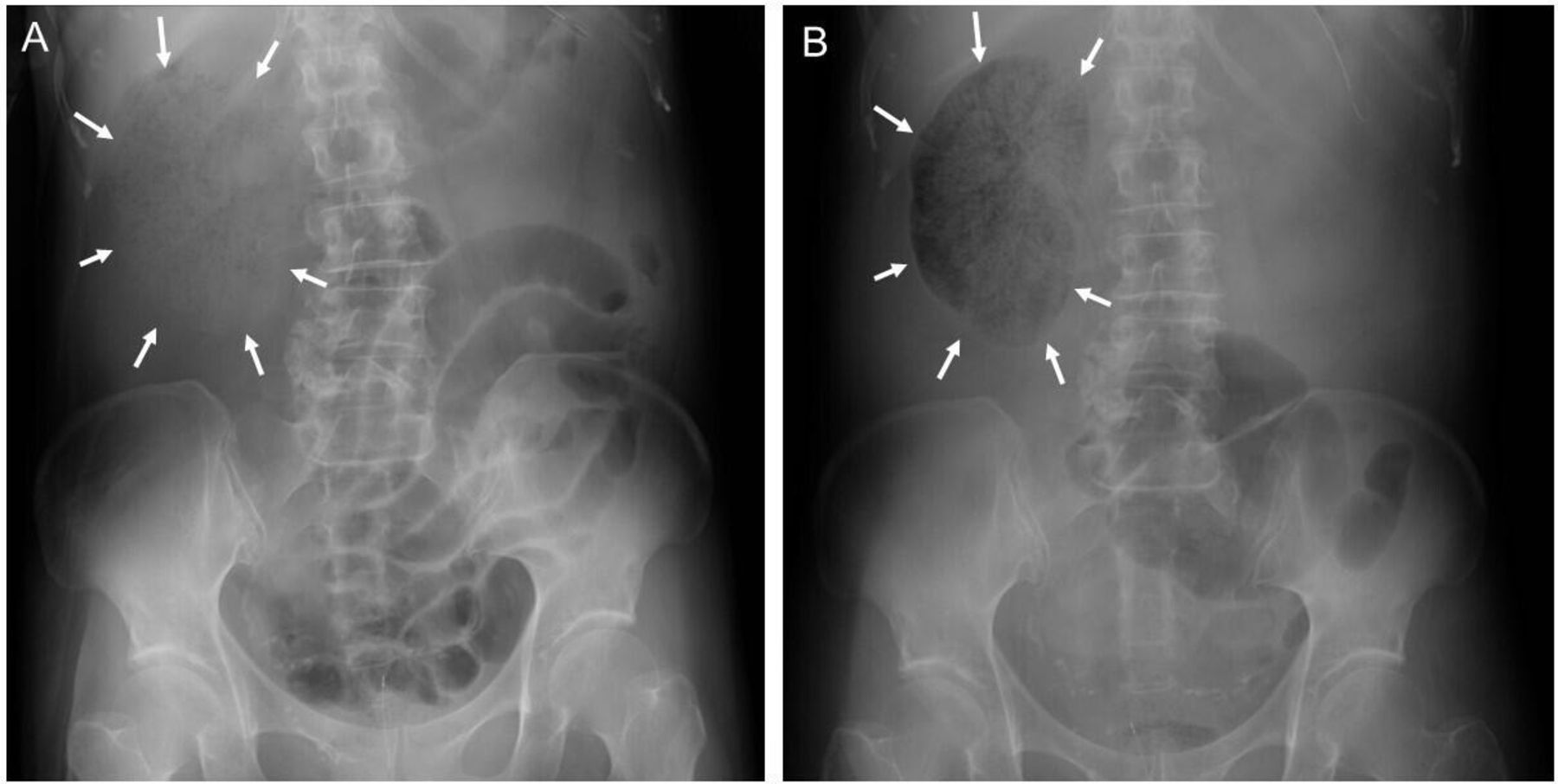
A 65-year-old woman presented with a 1-week history of right flank pain and fatigue. On the day of admission, she was found immobile at home and was transported by ambulance. Her medical history included diabetes mellitus and breast cancer 10 years ago. At admission, vital signs included: Glasgow Coma Scale: E4V5M6, blood pressure 77/55 mm Hg, heart rate 120 beats/min, temperature 36.2°C, and respiratory rate 42/min. Physical examination revealed a mildly distended abdomen with right flank and costovertebral angle tenderness. Blood tests showed white bleed cell count 18.5x109/L, hemoglobin 11.7 × 10-1 g/L, platelet 7.8×10-5/L, blood urea nitrogen 67.9 mg/dL, creatinine 3.53 mg/dL, sodium 124 mEq/L, potassium 3.7 mEq/L, chloride 84 mEq/L, prothrombin time-international normalized ratio 1.29, blood glucose 543 mg/dL and glycosylated hemoglobin A1c 12.1%. Blood gas analysis was significant for metabolic acidosis with pH 7.41, arterial oxygen pressure 101.6 mm Hg, PaCO2 16.1 mm Hg, bicarbonate 10.0 mEq/L, base excess 12.1 mEq/L, and lactic acid 3.43 mmol/dL. Urinalysis showed white blood cell 3+ and occult blood 3+. CT scan of the abdomen revealed emphysematous changes in the right kidney (figure 1), and the diagnosis of right emphysematous pyelonephritis (EPN) class 3B was made. She was admitted to the intensive care unit (ICU). After obtaining blood and urine cultures, meropenem and vancomycin were administered intravenously. Resuscitation continued with intravenous fluids, vasopressors, and steroids according to surviving sepsis guidelines, but her condition deteriorated. Six hours after admission, she was intubated and required mechanical ventilation. A portable abdominal X-ray showed progression of emphysematous changes in the right kidney (figure 2).

Non-contrast CT scan of the abdomen revealed a significantly enlarged and emphysematous right kidney (arrows) on the axial view (A) and on the coronal view (B).

A plain abdominal X-ray at admission showed a sparse bubbly shadow in the area of the right kidney (A). Six hours later, repeat X-ray showed that the right kidney shadow had been replaced by air (B).
What would you do?
Administer antifungal agents
Treat disseminated intravascular coagulation with recombinant human soluble thrombomodulin
Percutaneous drainage of the right perinephric abscess
Right nephrectomy
What we did and why
The patient was brought to the operating room by the acute care surgery team for exploratory laparotomy. As the ascending colon was mobilized, swelling in Gerota’s fascia was evident. Opening Gerota’s fascia resulted in the release of foul-smelling gas. The renal parenchyma was spongy and drained purulent material (figure 3) and a right nephrectomy was performed. After copious irrigation, the abdomen was closed. She was returned to the ICU postoperatively. Subsequent cultures of blood, urine and the purulent material in the right renal parenchyma revealed Escherichia coli. Antibiotics were continued for 14 days until leukocytosis and fever subsided. Postoperatively, she developed acute renal failure requiring hemodialysis. She underwent tracheostomy due to the need for prolonged mechanical ventilation. Eventually, she was weaned from hemodialysis and mechanical ventilation. She was transferred to a rehabilitation hospital 21 days after surgery.

{kind=link}
{kind=link}
{kind=link}
The right nephrectomy specimen had spongy changes throughout the parenchyma.
Discussion
EPN is a necrotizing infection of the renal parenchyma and surrounding tissues that often occurs in patients with urinary tract stones and diabetes and can be fatal in severe cases with a mortality reported as high as 11%–42%. Host factors contribute to the development of EPN, such as diabetes, malignant tumors, and urinary tract obstruction. Tseng reported in a multivariate analysis that patients with diabetes and urinary tract obstruction are more prone to develop EPN than those with routine urinary tract infections, especially patients with poorly controlled diabetes (glycosylated hemoglobin A1c >11.0%). Huang et al classified EPN based on CT scan findings: class 1: gas in the collecting system only, class 2: gas in the renal parenchyma without extension to the extrarenal space, class 3A: extension of gas or abscess to the perinephric space, class 3B: extension of gas or abscess to the pararenal space, and class 4: bilateral EPN or a solitary kidney with EPN. They specified four risk factors associated with poor outcomes including: thrombocytopenia, acute kidney injury, altered mental status, and shock. The treatment strategy for patients with EPN depends on Huang’s classification and the presence of risk factors. Class 1 and 2 patients are usually treated non-operatively. Class 3A and 3B patients with zero or one risk factor can be initially managed non-operatively, followed by surgical treatment in case of treatment failure. Of note, surgical treatment is the first choice for class 3A or B patients with two or more risk factors. For class 4 patients, bilateral percutaneous drainage is attempted, and surgical treatment is performed for treatment failure. Since the present patient had class 3B disease with four risk factors, surgical treatment was indicated according to the treatment algorithm based on Huang’s classification and risk factors.
In summary, the present patient with severe EPN class 3B and four risk factors was successfully treated by emergency nephrectomy. If the patient is in septic shock due to severe EPN, it is important to proceed with surgical source control as soon as possible.
Level of evidence
V.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by TUIC-COI 19-264. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors sincerely thank Professor Alan Kawarai Lefor for his guidance and English editing.
Footnotes
Contributors Conception and design—KI. Acquisition of data—KK. Drafting of the article—KK. Critical revision of the article—TN, TK, AT and KI. Supervision—KI.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.