Article Text

Abstract
Background Although hemorrhage remains the leading cause of survivable death in casualties, modern conflicts are becoming more austere limiting available resources to include resuscitation products. With limited resources also comes prolonged evacuation time, leaving suboptimal prehospital field care conditions. When blood products are limited or unavailable, crystalloid becomes the resuscitation fluid of choice. However, there is concern of continuous crystalloid infusion during a prolonged period to achieve hemodynamic stability for a patient. This study evaluates the effect of hemodilution from a 6-hour prehospital hypotensive phase on coagulation in a porcine model of severe hemorrhagic shock.
Methods Adult male swine (n=5/group) were randomized into three experimental groups. Non-shock (NS)/normotensive did not undergo injury and were controls. NS/permissive hypotensive (PH) was bled to the PH target of systolic blood pressure (SBP) 85±5 mm Hg for 6 hours of prolonged field care (PFC) with SBP maintained via crystalloid, then recovered. Experimental group underwent controlled hemorrhage to mean arterial pressure 30 mm Hg until decompensation (Decomp/PH), followed by PH resuscitation with crystalloid for 6 hours. Hemorrhaged animals were then resuscitated with whole blood and recovered. Blood samples were collected at certain time points for analysis of complete blood counts, coagulation function, and inflammation.
Results Throughout the 6-hour PFC, hematocrit, hemoglobin, and platelets showed significant decreases over time in the Decomp/PH group, indicating hemodilution, compared with the other groups. However, this was corrected with whole blood resuscitation. Despite the appearance of hemodilution, coagulation and perfusion parameters were not severely compromised.
Conclusions Although significant hemodilution occurred, there was minimal impact on coagulation and endothelial function. This suggests that it is possible to maintain the SBP target to preserve perfusion of vital organs at a hemodilution threshold in resource-constrained environments. Future studies should address therapeutics that can mitigate potential hemodilutional effects such as lack of fibrinogen or platelets.
Level of evidence Not applicable—Basic Animal Research.
- Blood coagulation
- resuscitation
- Shock, Hemorrhagic
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Whole blood is the gold standard for damage control resuscitation; however, it does not take into account prolonged field care and resource-constrained environments where crystalloid is the only option.
WHAT THIS STUDY ADDS
During resuscitation with crystalloid during a 6-hour prolonged prehospital time in a swine model of controlled hemorrhage, hypotensive resuscitation targets were able to be maintained without increased mortality. However, this resulted in a dilutional coagulopathy that was reversed with subsequent whole blood resuscitation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Findings from this study warrant further investigation in uncontrolled hemorrhage and polytrauma animal models to better understand how hemodilution and coagulopathy affect survival. This can be used in future clinical practice guidelines to direct resuscitation in austere prolonged field care scenarios where crystalloid may be the only resuscitation available.
Introduction
Despite advances in treatment, the leading cause of potentially preventable death in both military and civilian trauma continues to be hemorrhagic shock. Resuscitation and restoration of blood volume follow stabilization of the patient, which is referred to as a ‘damage control resuscitation’ strategy, the principles of which allow for permissive hypotension. Following the current Joint Trauma System (JTS) Clinical Practice Guidelines (CPGs), resuscitative fluids of choice are whole blood (WB) or blood products, with hydroxyethyl starch no longer recommended, and crystalloid used only in prolonged field care (PFC) scenarios, continuing until definitive surgical care is reached. However in the PFC scenario, prior to Role 2 surgical care, resuscitation with intravenous crystalloid administration is still common, given logistical and cost benefits as compared with blood products. Casualties in shock and absence of traumatic brain injuries are resuscitated to a ‘permissive’ hypotensive systolic blood pressure (SBP) generally recommended as 100±10 mm Hg.1 2 In the combat setting, this must be structured around robust evacuation capabilities with expeditious delivery of the casualty to definitive surgical control, with timelines based on the ‘golden hour’ concept. However, modern conflicts are becoming increasingly more austere and resource denied, and prehospital field care is expected to extend out to 72 hours or more.
The ideal ‘fluid’ for combat trauma and resuscitation is inarguably WB, with historical and current combat data supporting its continued use.3–5 In the austere and denied environment, however, there are logistical challenges for safe product delivery to the front lines. Warm, fresh WB continues to be available in the form of a walking blood bank (WBB), but in resource-denied environments, small teams, and care under fire scenarios, it can be difficult to manage a WBB without compromising overall manpower, resources, and mission goals.6–8 These realities unfortunately leave limited blood and component therapy available, with the more readily available crystalloid solutions as resuscitative fluids. In scenarios where crystalloids are the only available option, JTS CPGs allow for an even lower SBP target of 85±5 mm Hg when not able to use blood products.2 This is in part due to the anticipated volumes of fluids required to keep casualties stable and prevent worsening shock through increased prehospital timelines. The resulting fluids are likely to exceed that which would be necessary in an environment conducive to the ‘golden hour’, and hemodilution is more likely to occur, causing further disturbance of hemostasis and potentially contributing downstream to endotheliopathy.9 10
With the reality of modern conflicts moving towards becoming more austere, such as cold weather or maritime environments, questions regarding the safety and efficacy of prolonged hypotension in PFC settings remain. Although it has recently been demonstrated that 6 hours of hypotensive PFC can provide 100% survival with acceptable neurological outcomes, it is currently unknown how the increased resuscitative fluids needed to maintain acceptable targets will affect hemostasis. Therefore, the goal of this study was to determine the effects of maintaining permissive hypotension on hemostasis after hemorrhagic shock during 6 hours of PFC. We hypothesized that prolonged hypotensive resuscitation maintained via crystalloid will result in dilutional coagulopathy and endotheliopathy compared with normotensive and hypotensive controls.
Materials and methods
All procedures were performed in facilities accredited by the Association for Assessment and Accreditation of Laboratory Animal Care International. Animals were acquired from an approved vendor and free of select pathogens. Upon arrival, animals were group housed and allowed to acclimate for at least 3 days prior to procedures.
Preoperative preparation
Fifteen naïve male swine (Sus scrofa domesticus) weighing 70 kg to 90 kg were randomized via a random order generator into three experimental groups: (1) anesthesia sham (non-shock/normotensive: NS/NT, n=5); (2) hypotensive sham (NS/permissive hypotensive: NS/PH, n=5); or (3) decompensated hemorrhage+hypotension (Decomp/PH, n=5). Male swine were used in this protocol due to males constituting the majority of battlefield injuries,11 in addition to exhibiting more deleterious responses to traumatic hemorrhage than females across many species.12 Anesthesia sham controls were used to delineate any potential effects to coagulation seen from prolonged anesthesia, and hypotensive sham controls were included to establish any effects of prolonged hypotension in the absence of hemorrhagic shock and subsequent resuscitation. Although hypotensive controls were critical in the evaluation of neurological outcomes in the corresponding published article,13 it is important to include these findings in the context of dilutional coagulopathy because although hypotension can produce ischemic injury, the subsequent resuscitation from hemorrhagic shock is capable of producing a reperfusion injury. Experimental timeline is depicted in figure 1.

Experimental timeline. Schematic depicting experimental timeline, with time points running from instrumentation, through hemorrhage, prolonged field care (PFC), hospital care, postoperative recovery and observation, and euthanasia. Blood draws were obtained at each indicated time point for labs (complete blood counts, ROTEM, STAGO, and ELISAs) at baseline (BSLN), end of shock (EOS), PFC1, PFC2, PFC4, END PFC, end hospital care (EHC) and euthanasia (FINAL). ELISAs, enzyme-linked immunosorbent assay; MAP, mean arterial pressure; SBP, systolic blood pressure.
Animals were anesthetized and instrumented as previously described.13 Briefly, animals were sedated, intubated, and anesthesia was maintained on 1% to 3% isoflurane. The femoral artery and vein were catheterized for blood withdrawal, blood sampling, blood pressure monitoring, and resuscitation. Core body temperature was monitored via a rectal temperature probe and maintained between 36.0°C and 38.0°C. End-tidal carbon dioxide was monitored continuously on the Dräger Apollo Anesthesia Workstation.
Hemorrhagic shock
After baseline (BSLN) blood samples were drawn, hemorrhage was initiated by free flow of arterial blood until the mean arterial pressure (MAP) reached 30 mm Hg. Additional blood was withdrawn as needed to maintain a MAP of 30 mm Hg to 35 mm Hg. End of shock (EOS) was defined as physiological decompensation, where the animal was unable to maintain a MAP >30 mm Hg for 10 min. Hemorrhaged blood was collected in a blood donor bag containing anticoagulant citrate phosphate dextrose adenine solution at a 1:10 ratio for subsequent use in resuscitation.
To establish BSLN data and isolate any additional effects of anesthesia, animals in NS/NT group were maintained at normotensive levels (MAP ≥70 mm Hg) by administering supplemental fluid (lactated Ringer’s solution) during shock without a period of hemorrhage.
Simulated PFC
At the beginning of the 6-hour simulated PFC phase of resuscitation, isoflurane was gradually reduced to 0.4% to 0.5%, and an intravenous combination of propofol (3–10 mg/kg/hr) and buprenorphine (2–8 µg/kg/hr) started. Resuscitation via lactated Ringer’s solution commenced for Decomp/PH, targeting an SBP of 85±5 mm Hg, according to current JTS CPGs.2 Animals in the NS/PH group were brought down to and maintained at the target SBP by discontinuing fluid administration and removing blood until they reached 85±5 mm Hg. For both PH groups, the target SBP range was maintained by either infusing lactated Ringer’s solution to increase SBP or removing additional blood to decrease SBP.
Hospital care, recovery, and euthanasia
At the end of PFC (END PFC), animals entered a 2-hour simulated hospital phase. Anesthesia was returned to 1% to 3% isoflurane, with cessation of propofol and buprenorphine. Animals received a WB transfusion of 100% shed blood volume (SBV) preceded by calcium gluconate (23% solution; Vedco, Saint Joseph, MO) to counteract the anticoagulant. Additional resuscitation maintenance fluids (lactated Ringer’s solution) were infused during the final 90 min of hospital care to maintain MAP >70 mm Hg. At end of hospital care (EHC), all instrumentation was removed prior to recovering animals. Animals were transferred to a recovery pen where they were monitored for general condition and pain management. After the 24-hour recovery period, animals were sedated as described above, and final blood draws taken prior to the animals being humanely killed.
Blood draws and laboratory analysis
WB was collected as BSLN, EOS, PFC (hour) 1, 2, and 4, END PFC, EHC, and Final. Arterial blood gas parameters were assessed using a GEM Premier 4000 (Instrumentation Laboratory, Bedford, MA). Complete blood counts were evaluated by the ProCyte Dx Hematology (IDEXX Laboratories, Inc., Westbrook, ME). WB viscoelastic clotting properties were evaluated by rotational thromboelastometry (ROTEM Delta System, TEM Systems Inc., Durham, NC). ROTEM analyses included evaluation of extrinsic coagulation pathway function (ExTEM) and fibrin activity (FibTEM) to measure clotting time (CT), clot formation time (CFT), alpha-angle (α), amplitude 10 min after CT, (A10), and maximum clot firmness (MCF).
Concentrations of coagulation factors were evaluated using STAGO STA Compact (Diagnostica Stago Inc., Parsippany, NJ). STAGO analysis included prothrombin time (PT), partial thromboplastin time (PTT), antithrombin (ATIII), von Willebrand factor (vWF), fibrinogen (FIB), and D-dimer, in addition to a panel that included factors from both intrinsic and extrinsic pathways.
Biomarker analyses
Systemic inflammatory cytokines and chemokines in plasma to include interferon (IFN)-α, IFN-γ, interleukin (IL)-1β, IL-4, IL-6, IL-8, IL-10, IL-12p40, and tumor necrosis factor (TNF)-α were quantified using the Procartaplex Porcine Cytokine and Chemokine Panel (Invitrogen, Carlsbad, CA) performed on a Luminex IS100 (Luminex Corporation, Austin, TX). An enzyme-linked immunosorbent assay was used to quantify syndecan-1 in serum samples as a marker of endotheliopathy.
Data and statistical analysis
Statistical analyses were performed using Prism V.9 (GraphPad Software, Inc., La Jolla, CA), and all data are presented as mean±SD. No animals or data were excluded from the analyses. Two-way repeated measures analysis of variance with Bonferroni correction post-hoc analysis was used to determine statistical time and group differences for all blood markers, with p values of <0.05 considered to be statistically significant. All continuous data were tested for Gaussian’s normal distribution via D’Agostino-Pearson, Anderson-Darling, Shapiro-Wilk, and Kolmogorov-Smirnov normality tests. All data passed Gaussian’s assumptions and were run as parametric data. A priori and post-hoc power analyses were performed using G*Power V.3.1 Statistical Power Analysis program (Heinrich Heine Universitat Dusseldorf, Dusseldorf, Germany), to determine power for FibTEM A10, PT, and FIB. With 100% survival in all three groups and analyses showing power calculations over 0.9, sufficient group sizes were met to answer the hypothesis with a large effect size.
Results
Hemodilution
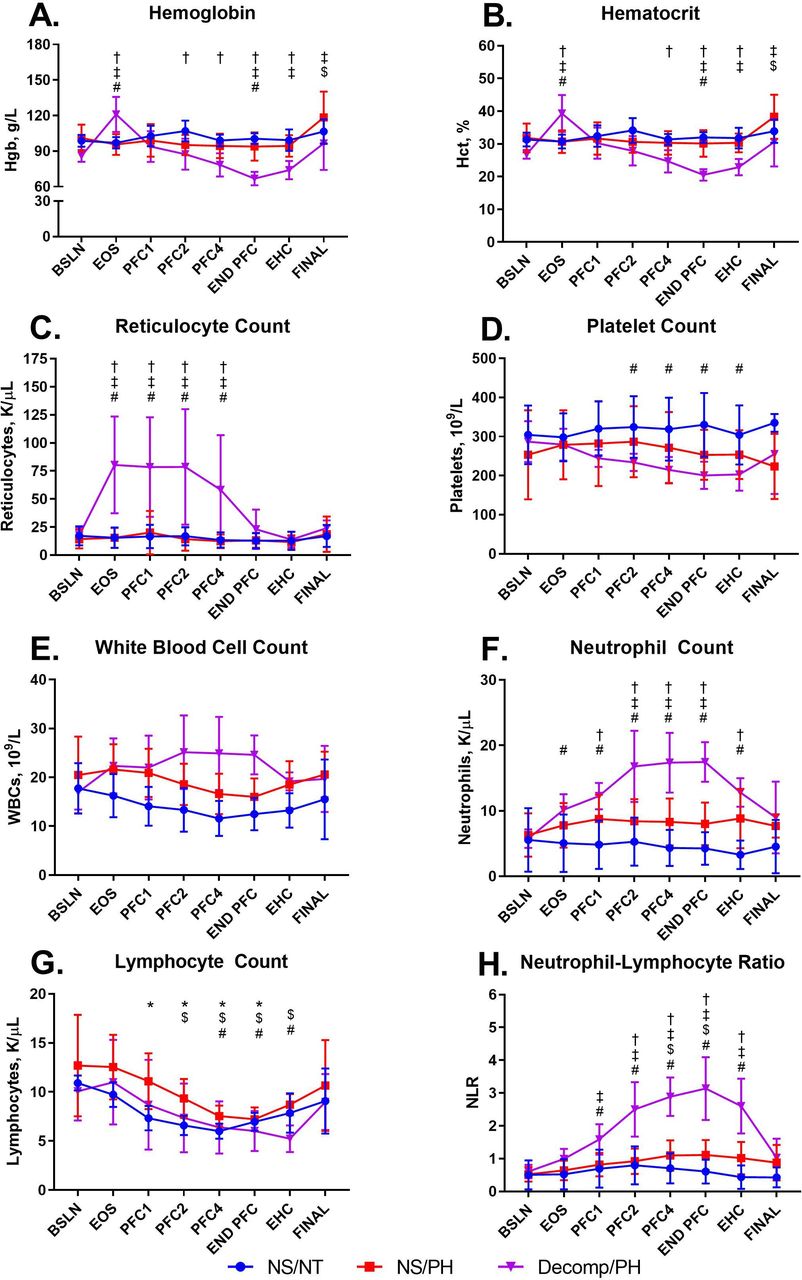
Total SBV for the Decomp/PH group was 2353.0±201.3 mL. To reduce the NS/PH group to PH, 784.6±433.0 mL of blood was removed. Throughout the 6-hour PFC, 5327.6±511.1 mL was infused in the Decomp/PH group and 1313.6±608.4 mL in the NS/PH group to maintain target pressure. The percent of blood in the circulating volume at END PFC for Decomp/PH (28.3±3.9%) was significantly lower than NS/PH (76.8±7.2%; p<0.0001). Hematocrit and hemoglobin both showed significant time and group effects (figure 2A,B). Decomp/PH hematocrit and hemoglobin were significantly increased from BSLN and both sham groups at EOS. However, as the 6-hour PFC continued, Decomp/PH hematocrit and hemoglobin started to decrease and were significantly lower than BSLN by END PFC. After WB resuscitation, both hematocrit and hemoglobin started to trend upward and were no longer significantly different at EHC. Decomp/PH hematocrit was significantly lower than NS/NT group at PFC4 through EHC, whereas hemoglobin was significantly lower at PFC2 but was resolved by Final. Compared with NS/PH, Decomp/PH hematocrit and hemoglobin were significantly lower at END PFC and continued through Final. Reticulocytes saw a significant rise from BSLN in Decomp/PH at EOS that was resolved by END PFC (figure 2C). Additionally, this rise led to significantly higher levels of reticulocytes than all other groups at these same time points. All partial pressure of oxygen (pO2) levels remained above 100 mm Hg, and all oxygen saturation (sO2) measures were above 95% (data not shown). No significant changes or differences were seen in the pO2 or sO2 throughout the protocol.

Complete blood count parameters. Complete blood count parameters were measured at all time points. Data are presented as mean±SD for (A) hemoglobin, (B) hematocrit, (C) reticulocyte count, (D) platelet count, (E) white cell count, (F) neutrophil count, and (G) lymphocyte count, (H) neutrophil–lymphocyte ratio. Colors indicate groups: NS/NT, blue; NS/PH, red; Decomp/PH, purple. P values of <0.05 were considered to be statistically significant. Significant differences between groups are indicated as: NS/NT versus Decomp/PH=† and NS/PH versus Decomp/PH=‡. Significant differences relative to BSLN are indicated as: NS/NT=*, NS/PH=$, and Decomp/PH=#. BSLN, baseline; Decomp/PH, decompensated hemorrhage+hypotension; EHC, end of hospital care; END PFC, end of PFC; EOS, end of shock; FINAL, euthanasia; NS/NT, non-shock/normotensive; NS/PH, non-shock/permissive hypotensive; PFC, prolonged field care.
Coagulopathy
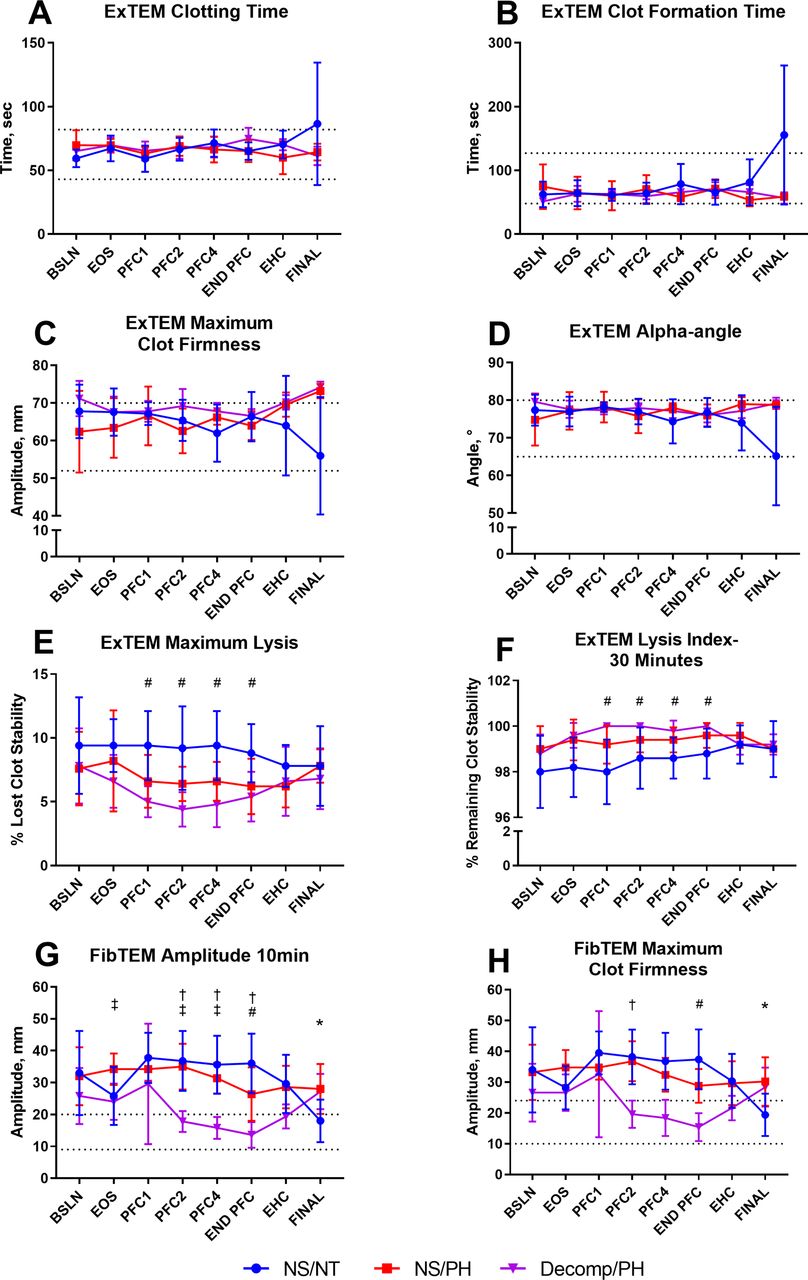
Platelets showed only a significant time difference, with Decomp/PH decreased from BSLN at PFC2 through EHC (figure 2D). No significant differences were seen between time periods or between groups in ExTEM CT, CFT, α, or MCF (figure 3A–D). The Lysis Index-30 Minutes of Decomp/PH group was significantly increased from BSLN throughout PFC, but returned to BSLN values by EHC (figure 3F). Additionally, maximum lysis was significantly decreased at the same time points (figure 3E). Both FibTEM A10 and MCF of Decomp/PH were significantly decreased from BSLN beginning at PFC1 and continued through the remainder of the protocol (figure 3G,H).
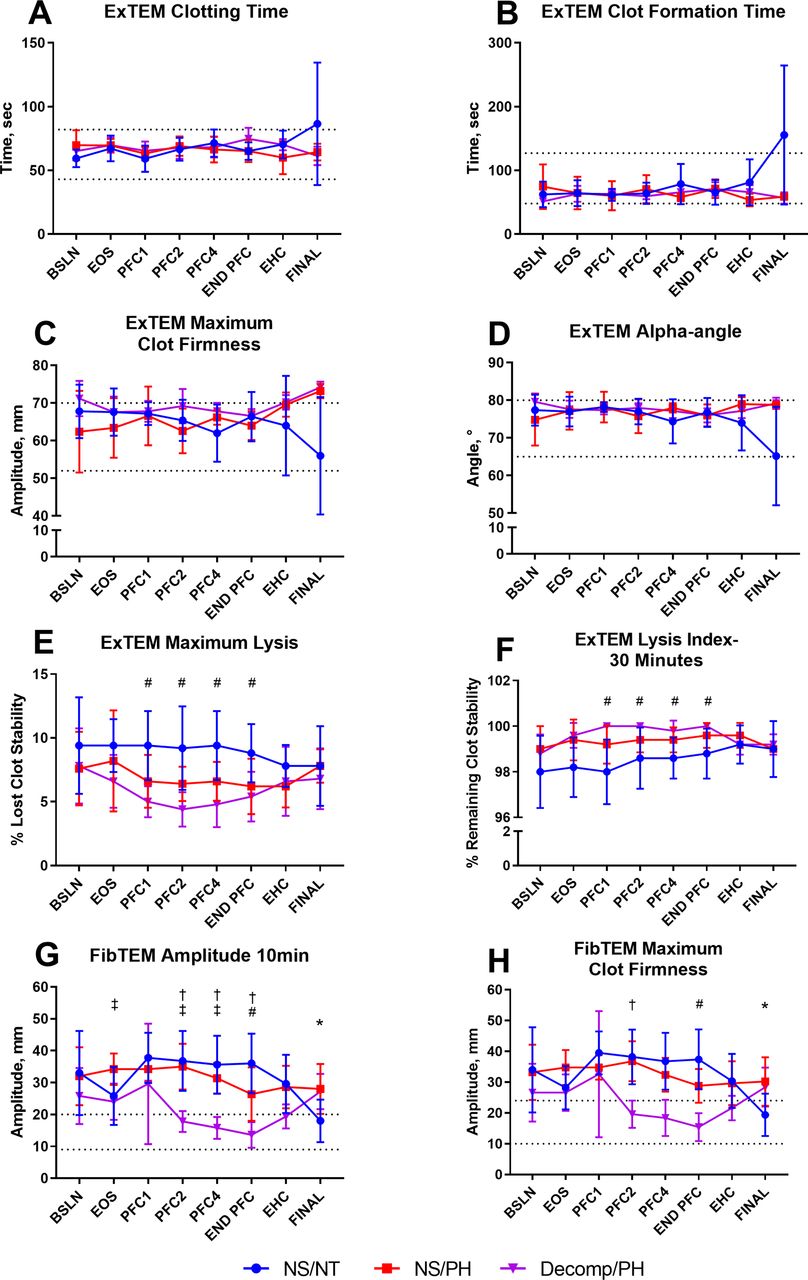
ROTEM parameters. ROTEM parameters were measured at all time points. Data are presented as mean±SD for (A) ExTEM clotting time, (B) ExTEM clot formation time, (C) ExTEM maximum clot firmness, (D) ExTEM alpha-angle, (E) ExTEM maximum lysis, (F) ExTEM Lysis Index-30 Minutes, (G) FibTEM amplitude 10 min, and (H) FibTEM maximum clot firmness. Colors indicate groups: NS/NT, blue; NS/PH, red; Decomp/PH, purple. Dotted lines represent human reference ranges as set forth by ROTEM. P values of <0.05 were considered to be statistically significant. Significant differences between groups are indicated as: NS/NT versus Decomp/PH=† and NS/PH versus Decomp/PH=‡. Significant differences relative to BSLN are indicated as: NS/NT=*, NS/PH=$, and Decomp/PH=#. BSLN, baseline; Decomp/PH, decompensated hemorrhage+hypotension; EHC, end of hospital care; END PFC, end of PFC; EOS, end of shock; FINAL, euthanasia; NS/NT, non-shock/normotensive; NS/PH, non-shock/permissive hypotensive; PFC, prolonged field care.
ATIII showed both significant time and group effects (figure 4F). Beginning at EOS, Decomp/PH ATIII was significantly higher than both sham groups and was not resolved until Final. PT, FIB, PTT, and vWF saw only significant time differences (figure 4A, C and E). Both Decomp/PH vWF and PT were significantly increased from BSLN values at EOS and PFC1, respectively. PT returned to BSLN values by Final; however, vWF remained significantly increased for the remainder of the protocol. Decomp/PH FIB and PTT showed significant reductions beginning at PFC1, but was corrected at EHC (FIB) and Final (PTT). D-dimer saw no significant changes in time or between groups (figure 4B). Factor II was significantly decreased from BSLN in the Decomp/PH group, as well as from the sham groups, at EOS through EHC (figure 5A). By PFC4, Decomp/PH had significant decreases from BSLN in Factor V that resolved by EHC (figure 5B). Decomp/PH Factor VII was significantly reduced at EOS to Final (figure 5C) and Factor X from PFC1 to EHC (figure 5F). As a result, both Factors VII and X were significantly decreased from the sham groups 1 hour into PFC and remained decreased through EHC.
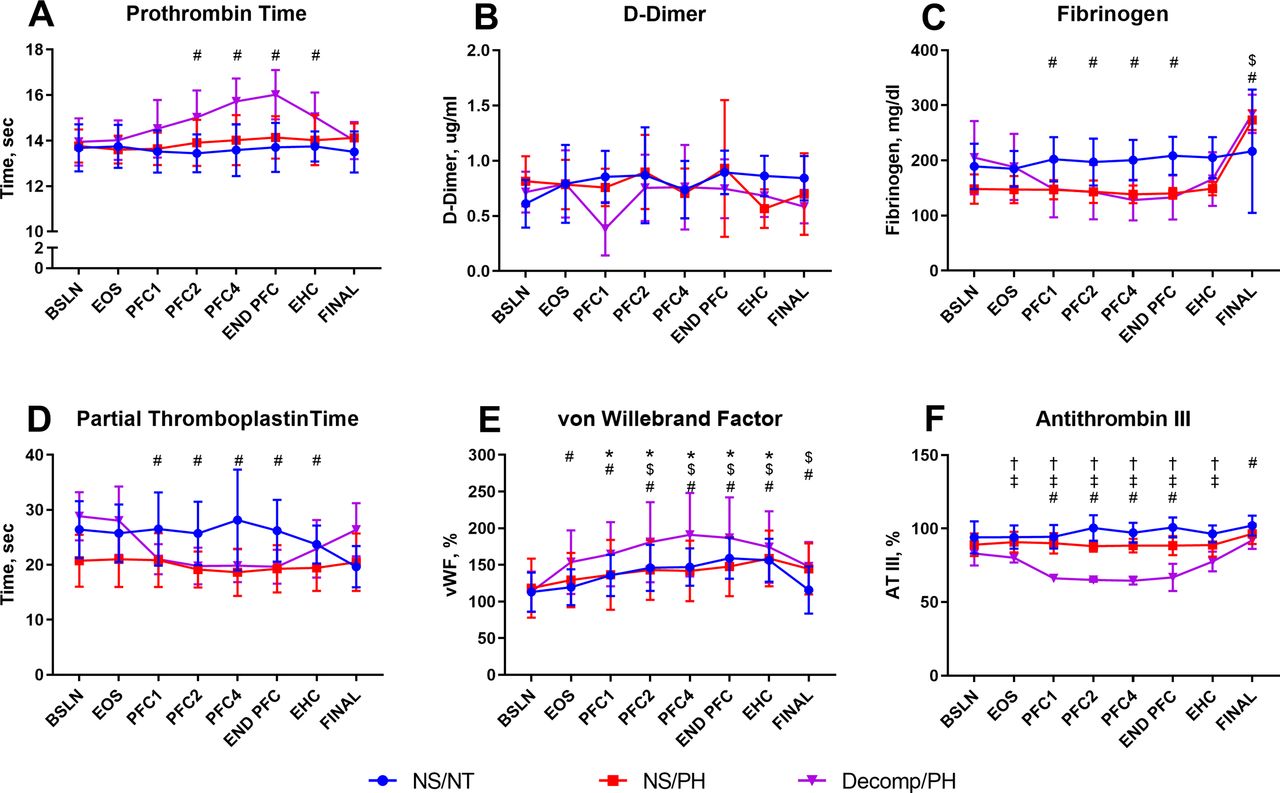
STAGO parameters. STAGO parameters were measured at all time points. Data are presented as mean±SD for (A) prothrombin time, (B) D-dimer, (C) fibrinogen, (D) partial thromboplastin time, (E) von Willebrand factor, and (F) antithrombin III. Colors indicate groups: NS/NT, blue; NS/PH, red; Decomp/PH, purple. P values of <0.05 were considered to be statistically significant. Significant differences between groups are indicated as: NS/NT versus Decomp/PH=† and NS/PH versus Decomp/PH=‡. Significant differences relative to BSLN are indicated as: NS/NT=*, NS/PH=$, and Decomp/PH=#. BSLN, baseline; Decomp/PH, decompensated hemorrhage+hypotension; EHC, end of hospital care; END PFC, end of PFC; EOS, end of shock; FINAL, euthanasia; NS/NT, non-shock/normotensive; NS/PH, non-shock/permissive hypotensive; PFC, prolonged field care.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
STAGO factors parameters. STAGO factors parameters were measured at all time points. Data are presented as mean±SD for (A) Factor II, (B) Factor V, (C) Factor VII, (D) Factor VIII, (E) Factor IX, (F) Factor X, (G) Factor XI, and (H) Factor XII. Colors indicate groups: NS/NT, blue; NS/PH, red; Decomp/PH, purple. P values of <0.05 were considered to be statistically significant. Significant differences between groups are indicated as: NS/NT versus Decomp/PH=† and NS/PH versus Decomp/PH=‡. Significant differences relative to BSLN are indicated as: NS/NT=*, NS/PH=$, and Decomp/PH=#. BSLN, baseline; Decomp/PH, decompensated hemorrhage+hypotension; EHC, end of hospital care; END PFC, end of PFC; EOS, end of shock; FINAL, euthanasia; NS/NT, non-shock/normotensive; NS/PH, non-shock/permissive hypotensive; PFC, prolonged field care.
Inflammation and biomarkers
No significant changes were seen in white cell counts (figure 2E). Decomp/PH neutrophils were significantly increased from BSLN at EOS through EHC (figure 2F). Additionally, neutrophil counts were significantly higher in the Decomp/PH group compared with NS/NT at PFC1 through EHC and NS/PH at PFC2 through END PFC. Lymphocytes were decreased in all groups throughout the protocol, but were resolved by Final (figure 2G). The neutrophil–lymphocyte ratio (NLR) showed significantly higher than BSLN values in the NS/PH group at PFC4 and END PFC and in the Decomp/PH group starting at PFC1 through EHC (figure 2H). Decomp/PH was also significantly higher than both control groups by PFC2 and remained so through EHC. Both groups were resolved back to BSLN values by Final. Monocytes, eosinophils, and basophil counts saw no significant changes over time or between groups (data not shown).
Of the nine cytokines measured, only IL-1β showed significant differences within and between groups. Decomp/PH was significantly decreased from BSLN and thus lower than NS/NT starting at EOS and continued through EHC. Levels were also significantly lower than NS/PH at EOS and PFC4. IL-12p40 of the Decomp/PH group was significantly increased from BSLN at EOS, PFC2, and PFC4. IFN-α, IFN-γ, IL-10, IL-4, IL-6, IL-8, and TNF-α showed no significant differences. No significant differences were seen in syndecan-1 over time or between groups (data not shown).
Discussion
In austere and resource-limited PFC environments, access to WB and blood products may be scarce, and although not ideal, crystalloids may be the last resort for resuscitation and bridging the time to optimal resuscitation and transfusion in casualties. The principle finding of this study is that in a simulated porcine model of PFC after decompensated hemorrhagic shock, large amounts of crystalloid solution can be used to maintain adequate perfusion during 6 hours without increased mortality in spite of dilutional coagulopathy relative to the negative control and hypotensive control groups. Additionally, in absence of tissue trauma, no inflammatory responses were seen to suggest prolonged hypotension or crystalloid volumes led to worsening endotheliopathy.
Marked reductions in hematocrit and hemoglobin revealed that hemodilution did occur during the course of the PFC phase. Although hematocrit reached 20% at the end of PFC, hemoglobin dropped below the critical threshold (80 g/L for patients not considered hemodynamically stable) 4 hours into PFC and continued to fall, indicating the immediate need for a transfusion. Despite these drops, sO2 remained above acceptable levels, indicating there were no issues with the oxygen-carrying capacity of the blood in the presence of the hemodilution. Additionally, the hemodynamic status was improved after WB transfusion at the simulated hospital care and was completely restored to BSLN levels by the end of the protocol, indicating that any deleterious effects during a 6-hour resuscitation period are still reversible with optimal resuscitation (WB) even if delayed.
At the end of the PFC, dilutional coagulopathy was not present when compared with clinical values used for humans. However, it is widely accepted that swine are more resilient to coagulopathy due to higher BSLN levels of platelets and FIB.14 15 This results in differences in coagulation measures to include PTT, CFT, and A10. Therefore, further analysis was used to better characterize changes seen in the porcine model and what those changes would look like based on human reference values16 17 that would be indicative of coagulopathy and the need for transfusion.18 After 6 hours of PFC, platelet counts were approximately 70% of BSLN values and fibrinogen dropped to 66%. If a human patient who presented BSLN values at the bottom of the normal range followed the same trend, platelet counts would still be above the critical threshold; however, FIB would be slightly below,19 20 suggesting increased need for FIB, either in the form of a concentrate, cryoprecipitate (plasma rich in FIB, vWF, factor VIII, and factor XIII), or WB.21
These same trends carried over into other ROTEM and STAGO measures. In the porcine model, none of the measures fell below critical thresholds. PT and ExTEM CT, both of which mimic normal human values, were only increased 15% and 14%, respectively, well below the threshold of 1.5 times normal to be considered ‘coagulopathic’.22–24 Interestingly, PTT was decreased to 69% of its BSLN value. This is opposite of what would be expected in dilutional coagulopathy, as the time for activated partial thromboplastin should increase as hemostasis is impaired.24 25 However, this decrease occurred during the first hour of PFC and remained stable until the end of PFC indicating there was no dilutional effect.
Likely as a result of the decreased FIB levels, FibTEM A10 and MCF saw 40% to 50% reductions in their measures. With the accepted clinical standards of A10 greater than 5 mm and MCF greater than 10 mm, the animals in the protocol remained well above these thresholds. Nevertheless, these marked reductions would leave human values at or below the critical level.
It is well established that neutrophils are increased in response to hemorrhagic shock and contribute to subsequent organ damage and failure.26 27 The Second Hit Theory postulates that hemorrhagic shock-induced ischemia and reperfusion via resuscitation activate the innate immune response before transitioning to an anti-inflammatory phenotype, thereby suppressing adaptive immune responders, and ultimately multiple organ dysfunction. The immune response observed here follows this pattern, as evidenced by the increased neutrophil counts through PFC. However, this increase is attenuated upon hospital resuscitation, and perhaps surprisingly, remains so 24 hours later. NLR was calculated due to its reported correlations with outcomes in patients with severe hemorrhage requiring massive transfusion protocol.28 The NLR of the Decomp/PH group at PFC1 of 1.6 entered the range of 1.1 to 5.2 reported for patients with hemorrhage at admission, and continued to climb to 3.1 by END PFC, surpassing the reported mean of 2.3 but still within the admission range. The study in human patients demonstrated that at day 3 and day 10 post-admission, NLR values greater than 8.82 and 13.69, respectively, were associated with increased in-hospital mortality. Comparatively, after resuscitation, the NLR of animals presented here had decreased by EHC to 2.6, reaching BSLN levels by the final time point. As such, after severe hemorrhage and 6 hours of prolonged hypotension with dilutional coagulopathy, NLR values here did not exceed the predictive cut-off thresholds for anticipated mortality.
The cytokine profile throughout PFC demonstrated no significant systemic change in the neutrophil activator IL-6 or the neutrophil chemotactic marker IL-8. Taken together with the unchanged IL-10 and syndecan-1 levels, and the previously published insignificant systemic organ damage,13 it can be concluded that 6 hours of prolonged hypotension and high volumes of crystalloid resuscitation do not generate the level of endotheliopathy or exacerbate neutrophil tissue invasion enough to create subsequent damage. However, changes in the nature of endothelial integrity, and certainly the dilutional coagulopathy, may be more detrimental in a model that uses concomitant tissue or vascular injury to induce a trauma-induced coagulopathy. The compounding effect of both dilutional and trauma-induced coagulopathies and endothelial disruption may result in more severe outcomes which WB resuscitation alone may not be able to overcome.
Limitations
The data presented here wield multiple limitations. The original study, designed to evaluate prolonged hypotension after hypovolemia, required animals to be recovered from anesthesia for neurological and behavioral monitoring. As such, neither severe traumatic injury nor uncontrolled hemorrhage could be safely incorporated into the protocol. Therefore, we used an established porcine model of pressure-targeted cardiovascular decompensation.29 30 The comparative differences in uncontrolled, pressure-targeted, and volume-targeted porcine hemorrhage modeling are discussed by Sondeen et al, who demonstrate pressure-targeted animals required more blood loss (21.5 mL/kg) to match the shock profiles of those undergoing uncontrolled hemorrhage (17.6 mL/kg).31 In our pressure-targeted model, our Decomp/PH group lost 34.4 mL/kg.13 These volumes per weight are higher than either group and additionally, for the Decomp/PH group, which spent between 60 and 90 min in shock before decompensating, levels of lactate (7.8±2.9 mmol/L) were higher here than those of Sondeen et al’s uncontrolled (6.0±0.8 mmol/L), pressure (6.7±1.1 mmoL/L), or volume (6.0±0.8 mmol/L) targeted modalities for equivalent time in shock. This controlled decompensated hemorrhage effectively mimics a clean penetrating trauma with hemorrhage, with severe hypovolemia representing the primary mechanism of physiologic burden. Hypovolemia itself has been associated with coagulopathy in clinical patients,26 and began to develop in this model as well, as demonstrated by significant declines in ATIII, Factor II, and Factor VII for the Decomp/PH group by EOS. As this injury pattern has been associated with coagulopathy due to the activation of fibrinolysis,32 combined with the anticipated dilutional coagulopathy expected from the resuscitation, rebleeding during PFC was not evaluated due to the risk of unnecessary and expected mortality. Additionally, as stated above, the coagulation profile of swine is different from humans, as they are less likely to become coagulopathic. To determine clinical significance compared with human values, percentages of BSLN values were used in the interpretation of the results as porcine blood has been shown to have similar responses to human blood.15
Conclusion
In this study, permissive hypotension was safe for 6 hours using crystalloid infusion to maintain targeted blood pressure despite resulting hemodilution in a porcine model of controlled hemorrhage shock and PFC. The effects seen on hemostasis and inflammatory markers known to contribute to endotheliopathy after hypervolemic hemodilution sustained during a 6-hour PFC phase were investigated. Although significant hemodilution occurred compared with the negative and hypotensive control groups, the impact on coagulation and endothelial function and integrity was minimal. However, the dilution of circulating volume to less than 30% approaches the critical threshold for clinically safe parameters of coagulation function and oxygen delivery (hematocrit/hemoglobin). These findings may help define in austere and resource-constrained environments an acceptable limit for hemodilution during 6 hours while maintaining the permissively hypotensive SBP target to preserve optimal perfusion of vital organs as a last resort when blood products are limited or unavailable. However, there should be further testing in different models with coagulation profiles more directly translatable to humans, to include polytrauma and uncontrolled hemorrhage injury patterns to elucidate any potential benefits or risks to optimize the translation to the warfighter and civilian casualties.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was reviewed and approved by the 711th HPW/RHD JBSA-Fort Sam Houston Institutional Animal Care and Use Committee (IACUC) in compliance with all applicable federal regulations governing the protection of animals in research. In conducting research using animals, the investigators adhered to the laws of the USA and the regulations of the Department of Agriculture.
Acknowledgments
The authors would like to acknowledge the contributions of the NAMRU-SA Expeditionary and Trauma Medicine Department, as well as LTC Kamala Rapp-Santos and Ashley Arredondo and the NAMRU-SA Veterinary Sciences Department for their excellent veterinary support.
References
Footnotes
Contributors LEN—guarantor, study design and implementation, data acquisition, analysis, and interpretation, article drafting and revisions. CGM—study design and implementation, data acquisition, analysis, and interpretation, article drafting and revisions. ENH—data interpretation and analysis, and article revisions. PJH—study implementation, data acquisition, analysis, and interpretation, article drafting. MMT—data interpretation and article revisions. SC—data interpretation and article revisions. JJG—study design and implementation, data analysis and interpretation, and article revisions.
Funding This work was supported by the Assistant Secretary of Defense for Health Affairs, through the Fiscal Year 2016 Defense Medical Research and Development Program Prolonged Field Care Research Award–Intramural (LOG number: DM167139).
Disclaimer The views expressed in this article reflect the results of research conducted by the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of the Army, Department of Defense, nor the US Government.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.