Article Text

Abstract
Objective To quantify and assess the relative performance parameters of thoracic lavage and percutaneous thoracostomy (PT) using a novel, basic science 2×2 randomized controlled simulation trial.
Summary background data Treatment of traumatic hemothorax (HTX) with open tube thoracostomy (TT) is painful and retained HTX is common. PT is potentially less painful whereas thoracic lavage may reduce retained HTX. Yet, procedural time and the feasibility of combining PT with lavage remain undefined.
Methods A simulated partially clotted HTX (2%-gelatin-saline mixture) was loaded into a TT trainer and then evacuated after randomization to one of four protocols: TT+/-lavage or PT+/-lavage. Standardized inserts with fixed 28-Fr TT or 14-Fr PT positioning were used to minimize tube positioning variability. Lavage consisted of two 500 mL aliquots of warm saline after initial HTX evacuation. The primary outcome was HTX volume evacuated. The secondary outcome was additional procedural time required for the addition of the lavage.
Results A total of 40 simulated HTX trials were randomized. TT alone evacuated a median of 1236 mL (IQR 1168, 1294) leaving a residual volume of 265 mL (IQR 206, 333). PT alone resulted in a significantly greater median residual volume of 588 mL (IQR 497, 646) (p=0.002). Adding lavage resulted in similar residual volumes for TT compared with TT alone but significantly less for PT compared with PT alone (p=0.002). Lavage increased procedural time for TT by a median of 7.0 min (IQR 6.5, 8.0) vs 11.7 min (IQR 10.2, 12.0) for PT (p<0.001).
Conclusion This simulation trial characterized HTX evacuation in a standardized fashion. Adding lavage to thoracostomy placement may improve evacuation, particularly for small-diameter tubes, with little added procedural time. Further prospective clinical study is warranted.
Level of evidence NA.
- Hemothorax
- Thoracic Injuries
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Rates of adverse outcomes, such as retained hemothorax, are high in cases of acute hemothorax initially managed with open tube thoracostomy alone.
Recent studies have shown that percutaneous thoracostomy is feasible and associated with less pain whereas adding thoracic lavage to open thoracostomy may improve outcomes.
WHAT THIS STUDY ADDS
This simulation study demonstrates the feasibility of adding thoracic lavage to percutaneous thoracostomy and quantifies the time required to complete thoracic lavage.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Thoracic lavage adds little procedural time to both chest tube and percutaneous thoracostomy and may improve initial evacuation for percutaneous thoracostomy.
Further research is warranted to analyze the effectiveness of percutaneous thoracostomy with thoracic lavage in a clinical setting.
Introduction
Acute traumatic hemothorax (HTX) and hemopneumothorax occur in an estimated 300 000 patients in the USA annually1 and occurred in 615 combat casualties from 2003 to 2011.2 Traditional open tube thoracostomy (TT) represents an important diagnostic and potentially therapeutic intervention. For patients with self-limited thoracic hemorrhage, TT placement can be definitive.3–5 However, recent prospective evidence indicates retained hemothorax (RH) occurs in up to 44% of patients with an acute HTX and that those who develop a RH have worse outcomes compared with those who do not.6
One approach that may mitigate the development of RH is warm saline lavage at the time of initial TT insertion. Compared with traditional thoracostomy, adding irrigation (1 L warm saline) significantly lowered the rate of secondary intervention for a RH from 21.8% to 5.6%.7 8
Unfortunately, open TT techniques cause significant patient discomfort. Percutaneous thoracostomy (PT) catheters, by comparison, cause significantly less patient-reported discomfort during insertion.9–12 Growing evidence also suggests that PT drainage of HTX in stable patients results in failure rates similar to open TT.13 This less invasive approach may be preferable to traditional open TT, although concerns remain over the potential for tube obstruction and inadequate drainage using small diameter catheters.14
Combining lavage with PT represents a novel approach that may minimize the rate of RH while also minimizing patient discomfort. Currently, no studies exist comparing the use of percutaneous catheters to conventional chest tubes with thoracic lavage in the treatment of HTX in civilian trauma patients or combat casualties. The feasibility of this approach remains uncertain, and the time required to add lavage to PT insertion is unknown. Thus, we designed a simulation study to lay the groundwork for future clinical studies comparing PT to open TT with and without the use of saline lavage. We hypothesize that PT will evacuate similar volumes compared with TT and that the addition of saline lavage will improve evacuation volumes of both PT and TT.
Methods
Study setting and design
This study was a 2×2 randomized controlled simulation trial in which HTX evacuation was compared between 28-Fr TT and 14-Fr PT with and without saline lavage. All research was conducted in the Penn Medicine Clinical Simulation Center, using medical task trainers in a simulated operating room.15 We followed the CONSORT reporting guidelines with the appropriate extensions for simulation studies (online supplemental digital content).16 17
Supplemental material
The primary endpoint for all evacuations was the total volume of HTX evacuated in milliliters (mL). For evacuations including saline lavage, the total time in minutes required to conduct serial lavages and evacuations was measured as a secondary endpoint. With an alpha of 0.05 and 80% power, it was calculated that 10 samples from each study arm would be necessary to detect a difference of at least 150 mL in HTX volume evacuated.
Two researchers (NRM, NMI) performed a total of 10 evacuations per study arm for a total of 40 evacuations. The order of evacuations was randomized using a block randomization method with a computer-generated random number list (created by DS), ensuring that each of the two investigators (NRM and NMI) performed five evacuations per study arm. Intraprocedural time data were collected by the investigators performing the thoracostomies, whereas a third team member blinded to the procedure performed (LTF, MMB), quantified the volume of residual HTX.
Materials
Simulated HTX
A variety of materials including animal blood, commercial moulage products, and gelatin were considered for modeling HTX. Although animal blood may have provided a higher-fidelity model, we found it would have presented insurmountable challenges in terms of maintaining consistency across trials. Gelatin provided a comparatively consistent although simpler model. A variety of gelatin mixtures, ranging from 1% to 4% gelatin by mass in water, were prepared and assessed for their qualitative likeness to partially clotted HTX. A 2%-gelatin mixture was determined to resemble the solid component of clotted HTX most closely and was used throughout the study to simulate the solid component of clotted HTX. A partially clotted HTX mixture was then simulated with a dual-density model by combining a rough slurry of 2% by weight gelatin with normal saline in a 1:2 ratio for a total volume of 1500 mL. This volume of HTX was chosen to reflect a large HTX and to adequately submerge the drainage tube within the HTX mixture. This simulated HTX slurry was placed into a Limbs & Things Chest Drain Trainer and sealed with Advanced Chest Drain Pads (Limbs & Things, Savannah, GA) (figure 1). To limit variation due to tube placement, each chest pad was prepared in advance with either a 14-Fr pigtail catheter (Cook Medical LLC, Bloomington, IN) or 28-Fr Argyle chest tube (Cardinal Health, Dublin, OH) positioned posteriorly and apically with the shallowest side hole of each tube fixed at a depth of 11 cm relative to the internal plane of the chest pad. A CLR Irrigator (CLR Medical, Calverton, MD) was used for evacuations involving warm saline lavage. Suction was applied using wall suction or a Pleur-evac Chest Drainage System (Teleflex, Morrisville, NC).

Experimental setup. (A) Schematic of CLR irrigator. (B) CLR irrigator. (C) Limbs & Things Chest Drain & Needle Decompression Trainer with chest pad and 14Fr cook pigtail catheter inserted.
Procedure
For each evacuation, a chest drain trainer was loaded with 1500 g of simulated HTX (500 g 2%-gelatin, 1000 g normal saline, 1498 mL total),18 sealed with a chest pad, and checked for leaks before proceeding with evacuation. Both procedures for evacuations performed with and without lavage were designed to take approximately 15 min to maintain appropriate blinding for the evaluator (figure 2). For evacuations including lavage, the time from beginning the initial evacuation to terminating the final evacuation varied and was recorded as the time required to perform serial lavages. As the time to perform serial lavages and evacuations varied across trials, the duration of applied Pleur-evac suction was adjusted to maintain the total procedural time of 15 min for evacuations including lavage.
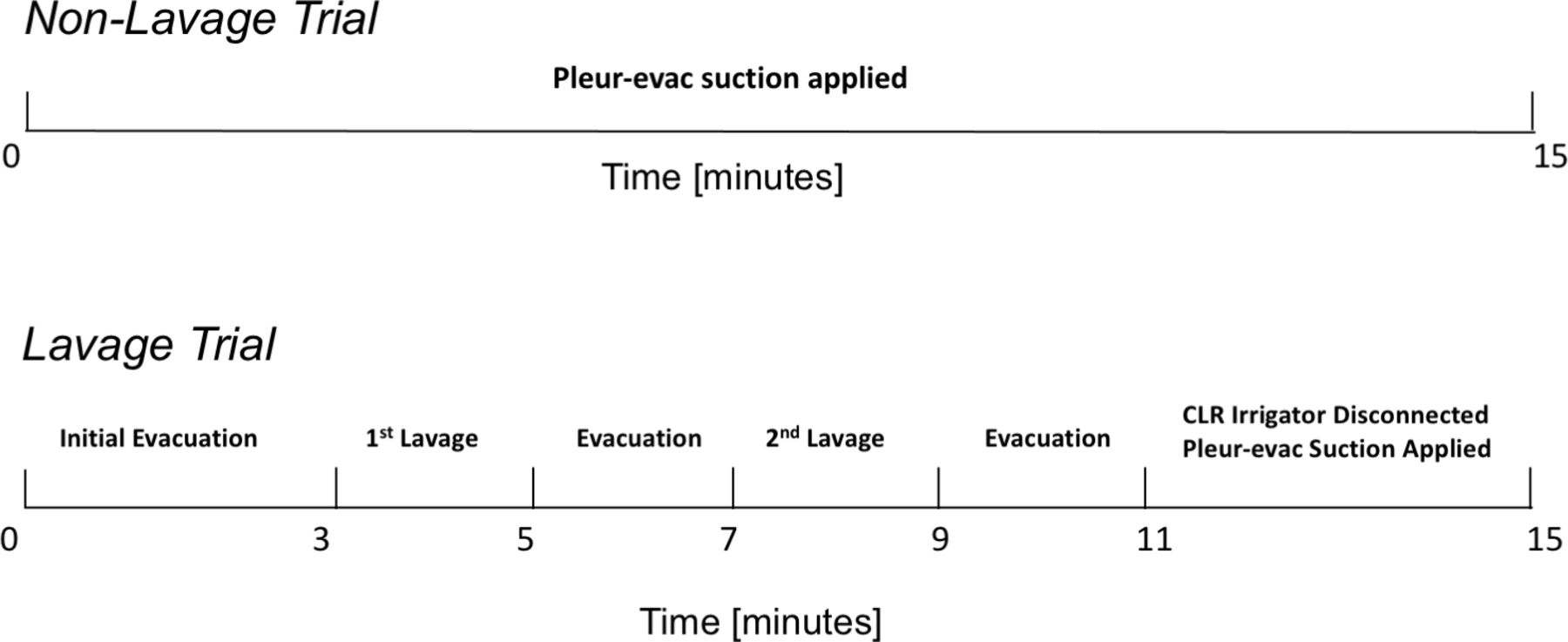
Experimental procedure timeline.
In evacuations without lavage, the chest tube or catheter was connected to a Pleur-evac Chest Drainage System with water seal. Suction was then applied at −20 cm H2O for 15 min. For evacuations including lavage, the chest tube or catheter was connected via the CLR Irrigator to both wall suction set to −100 mm Hg and a 1 L bag of normal saline elevated to a constant height of approximately 30 in. above the tabletop. An initial evacuation was performed for either 3 min or until flow ceased. Then, 500 mL of warm saline was lavaged and evacuated followed by a second 500 mL lavage and evacuation. Each lavage and evacuation were performed for either 3 min or until flow ceased for 10 consecutive seconds, whichever was shorter. After the second lavage and evacuation, suction was removed, the CLR was disconnected, and the chest tube or catheter was connected to Pleur-evac suction at −20 cm H2O for approximately 4 min or until a total procedural time of 15 min. After either evacuation procedure, the researcher that performed the evacuation removed the chest pad. Then, the blinded evaluator drained and measured the remaining simulated HTX.
Statistical analysis
Findings are presented as median and IQR. One-way analysis of variance (ANOVA) was used to determine significant variance in the amount of HTX evacuated across all study arms. All analyses directly comparing any two study arms were conducted using Wilcoxon Rank Sum. A resulting p value of less than or equal to 0.05 was considered significant. Data analysis was performed using R V.4.1.0 (R Core Team, Vienna, Austria).
Results
The results of five evacuations were excluded due to early procedural modifications including increasing the total simulated HTX volume from 1000 to 1500 mL, increasing the insertion depth of chest tubes and catheters, and moving the Pleur-evac system from the tabletop to ground level (online supplemental figure). The reduction in sample size decreased the calculated power of the study, increasing the minimal detectable difference in HTX evacuation from 150 to 180 mL. To maintain the statistical power of the study, these five trials were repeated later. The final analysis reported here is based on a total of 40 trials, including 35 trials of the initial trials and the five repeated studies. The results from an intention-to-treat analysis using the 40 initial trials as well as a per-protocol analysis using the 35 trials after procedural modification are available in the supplemental material (online supplemental figure).
Evacuation performance
The primary outcome of this study was the amount of simulated HTX evacuated, referred to as the evacuation performance (figure 3, table 1). An ANOVA showed that the effect of the study arm on the amount of simulated HTX evacuated was significant (F[3,36]=9.537, p<0.001). Wilcoxon rank sum pair-wise tests revealed that median evacuation performance for TT without lavage, 1236 mL (IQR 1168, 1294), was not significantly different than the evacuation performance for TT or PT with lavage, which evacuated volumes of 1255 and 1160 mL, respectively (table 2). PT without lavage, however, performed significantly worse than the other three study arms, evacuating a median of 912 mL (IQR 854, 1004), only 61% of the loaded HTX, leaving a median residual volume of 588 mL.
HTX evacuation data
HTX evacuation performance analysis

HTX evacuation performance. *P<0.05 compared with all others by Wilcoxon rank sum posthoc test.
Time burden of performing serial lavages
The time required to perform serial saline lavages is defined here as the time from the start of an evacuation trial to the completion of the third evacuation and the removal of the CLR device (figure 2). Performing serial lavages and evacuations with TT took a median of 7.0 min (IQR 6.5, 8.0) vs 11.7 min (IQR 10.2, 12.0) for PT (p<0.001) (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Additional procedural time due to performing lavage.
Per-protocol analysis of initial trials
The per-protocol analysis of the original 35 trials after the early procedural modifications was conducted identically to the reported analysis of the 40 trials including the five repeat studies. The addition of the five repeated trials did not significantly change the results of the study. Analysis of the original 35 trials found that median evacuation performance for TT without lavage, 1236 mL (IQR 1167, 1295), was not significantly different than the evacuation performance for TT or PT with lavage, which evacuated volumes of 1272 and 1064 mL, respectively (table 1). PT without lavage also performed significantly worse than the other three study arms, evacuating a median of 930 mL (IQR 846, 1005), only 62% of the loaded HTX, leaving a median residual volume of 570 mL (online supplemental figure).
The time required to perform serial lavages was also not significantly affected by the addition of the five repeated trials. Based on the original 35 trials, performing serial lavages and evacuations with TT took a median of 6.9 min (IQR 6.5, 7.1) vs 11.3 min (IQR 10.2, 11.8) for PT (p<0.001) (online supplemental figure).
Intention-to-treat analysis
The intent-to-treat analysis of the original 40 trials was conducted similarly to the per-protocol analysis except that evacuation performance was normalized to the percent of loaded HTX evacuated due to varying load volumes. Including the five evacuations excluded due to early procedural modifications in the analysis found that PT without lavage performed significantly worse than both TT without lavage and PT with lavage, evacuating a median 60.8% (IQR 49.8, 66.7). However, unlike in the per-protocol analysis, PT without lavage did not perform significantly differently than TT with lavage in the intention-to-treat analysis (online supplemental figure).
The time required to perform serial lavages was similar using the intention-to-treat analysis. Performing serial lavages and evacuations with TT took a median of 7.1 min (IQR 6.60, 8.45) vs 11.4 min (IQR 10.20, 12.03) for PT (p=0.015) (online supplemental figure).
Discussion
In this 2×2 randomized controlled simulation trial, we assessed the novel technique of adding lavage to percutaneous 14-Fr pigtail drainage of a simulated HTX. In this study, we found that PT evacuation alone was significantly worse than open drainage of a simulated HTX but that saline lavage improved the performance of PT to a level comparable to TT with or without lavage. We also measured the time required to add a specific lavage protocol to either open TT or PT insertion. Specifically, this lavage protocol added approximately 7 min to open TT and 12 min to PT over baseline. These findings will inform our study design as we seek to evaluate these four HTX evacuation techniques in the context of a prospective trial.
This simulation study demonstrates that combining PT and saline lavage is feasible and that this novel approach may result in HTX evacuation performance similar to TT. However, HTX evacuation performance using PT with saline lavage varied more than volumes evacuated by TT with or without lavage. The greater variability in PT performance and the significant benefit from the inclusion of saline lavage may both be due to the stochastic event of tube obstruction or mechanical properties of the evacuation holes. First, obstruction is more likely to impact PT than TT simply because obstruction is more likely to occur in tubing with smaller lumens. Depending on when the obstruction occurs, particularly if it is a complete obstruction, an evacuation procedure may be effectively cut short. Serial lavages may alleviate the effect of such obstructions by reversing the flow and flushing the tubing. That is, the benefit of the saline lavage to PT observed in this study may be due primarily to clearing the tubing.
However, the clinical experience with TT for HTX management suggests an intrathoracic benefit to lavage. High rates of retained HTX have been noted with standard TT sizes (eg, median TT size 32F in Prakash et al6 with a retained HTX noted in up to 44% of cases) without associated tube obstruction. Furthermore, lavage has been associated with a 75% relative reduction in the rate of clinically relevant RH—again in the absence of routine tube obstruction.7 8 As such, the apparent similar performance of TT with or without lavage may reflect a limitation of the simulation model in that the trainer is not an air-tight closed system and thus did not replicate the complex interplay of structures inside the live thoracic cavity, nor did our simulated HTX replicate the range of potential consistencies of congealed HTX present in a clinical setting.
Moreover, the study may have been underpowered to identify a meaningful difference between TT and TT+lavage. Similarly, the median amount of HTX evacuated in the PT with lavage falls below the first quartile TT without lavage just 10 mL above the first quartile of TT with lavage despite analysis finding no significant difference. Unfortunately, including the trials excluded due to early procedural modifications in the intention-to-treat analysis decreased the strength of statistical findings due to combining evacuations with varying procedures in single study arms. However, the results from the final analysis with five repeated studies did not differ significantly from the more limited per-protocol analysis of 35 trials after early procedural modifications, suggesting robust results for this simulation study. A larger clinical study will likely be required to assess the added benefit of lavage via TT’s and the true difference between PT with lavage and TT with or without lavage.
This study also quantified the time required to enact a specific lavage protocol involving two, 500 mL serial lavages with the CLR Irrigator. In the case of PT with lavage, that time exceeded 10 min. If this added initial procedural time investment spares the patient significant discomfort and reduces the risk of RH, it may be well worthwhile for stable patients in both civilian and military settings. However, we also recognize this may not be appropriate in all clinical settings, particularly if the patient is clinically tenuous, wherein TT use may be preferable.3
Beyond the scope of thoracic trauma, this study also provides value as an example of using simulation technologies to prepare for a clinical trial, a strategy often overlooked in favor of pilot studies. Research on acute conditions in austere settings, such as battlefield trauma or mass casualty events, requires opportunistic encounters which are complex and uncertain. Simulation provides a means to control these challenging environments to best prepare for subsequent studies in the less structured, real-world environment. As an example, a recent study on optimizing a decision support system for damage-control resuscitation used precisely this strategy to iteratively improve a tool through simulation before deploying it for evaluation in a clinical setting.19 We hope that this study will similarly lay the groundwork for further research on HTX management in a clinical setting.
Study limitations
Simulation is necessarily limited as the model’s level of complexity and, in turn, external validity must be weighed against time and resources. We analyzed that our model was adequate to mechanically challenge chest tubes and percutaneous catheters in their ability to remove a dual density mixture, and we believe that further assessment would be best performed in a live tissue model. Although this study provides valid insight into how semisolid mixtures, and thus small obstructions, may affect performance parameters between 14-Fr catheters and 28-Fr chest tubes, it has significant limitations. First, the gelatin mixture used to simulate HTX is meaningfully different than partially clotted HTX. This relatively simple dual density model of gelatin and saline does not capture the dynamic complexity of clot formation or the variability in clot characteristics that are best observed in living animal or human subjects. Second, the chest drain trainer, while a useful training tool, does not replicate the complex interplay of structures inside the live thoracic cavity. As an example, the trainer has a rigid frame and is only water-tight, not air-tight, when sealed. As a result, any simulated HTX that was removed was immediately replaced with atmospheric air, and the efficacy of any evacuation decreased drastically once any hole in the catheter or chest tube in use was uncovered. The reservoir of the trainer also fails to replicate the complex physiology created by the motion of the diaphragm and lungs. Finally, loss of data for 5 of the 40 planned evacuation scenarios, added additional confounding to our trial as these evacuations were completed at a later time.
Conclusion
In the context of this simulation model, PT drainage of HTX with lavage is feasible. Adding lavage to thoracostomy placement may improve initial evacuation, particularly for small-diameter tubes, with little added procedural time. A prospective study to assess the relative effectiveness of PT and TT with or without lavage is warranted.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors NRMcL, JWC, NMI, LTF, CBR, and CAB contributed to the design of this study. NRMcL, NMI, LTF, CBR, DS, MMB, and CAB contributed to the execution of the study. NRMcL, JWC, and ZG developed the statistical methodology. NRMcL wrote the first draft of the article. All authors provided critical revisions and approved the final version. JWC serves as guarantor of this study and as such accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This work was made possible through the generous support of the Measey Scholars Program, Department of Surgery, Perelman School of Medicine at the University of Pennsylvania. CLR Medical provided the CLR Irrigators in-kind but did not provide study funding and had no role in the study design or data analysis.
Disclaimer The views in this article are those of the authors and do not represent an endorsement by or the views of the United States Navy, the United States Air Force, the Department of Defense, or the United States Government.
Competing interests ANS is Chief Medical Officer of CLR Medical which makes the CLR irrigator. The remaining authors declare no conflict of interest. This work was made possible through the generous support of the Measey Scholars Program, Department of Surgery, Perelman School of Medicine at the University of Pennsylvania. CLR Medical provided CLR Irrigators in-kind but did not provide study funding and had no role in the study design or data analysis.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.