Article Text

Statistics from Altmetric.com
Case presentation
A 31-year-old woman with a history of Down syndrome, hypothyroidism, type 2 diabetes, and a 13-year history of extended-cycle contraceptive pill use presented to the emergency department after a syncopal episode witnessed by her mother. She also had an episode of non-bloody, non-bilious emesis earlier in the evening.
On clinical presentation, the patient was hypotensive at 90/60, tachycardic, and had a hemoglobin of 4.8 and a lactate of 11.66. Her abdomen was peritonitic on examination. Immediate management included resuscitation with fluids and blood to manage her hypotension.
CT scan revealed a 9.8×13.9 cm hematoma in the left lobe of the liver with active bleeding and hemoperitoneum and a contained 9.7×10.9 cm hematoma in the right lobe (figures 1 and 2).

Axial CT image showing the large bilateral hepatic adenomas.
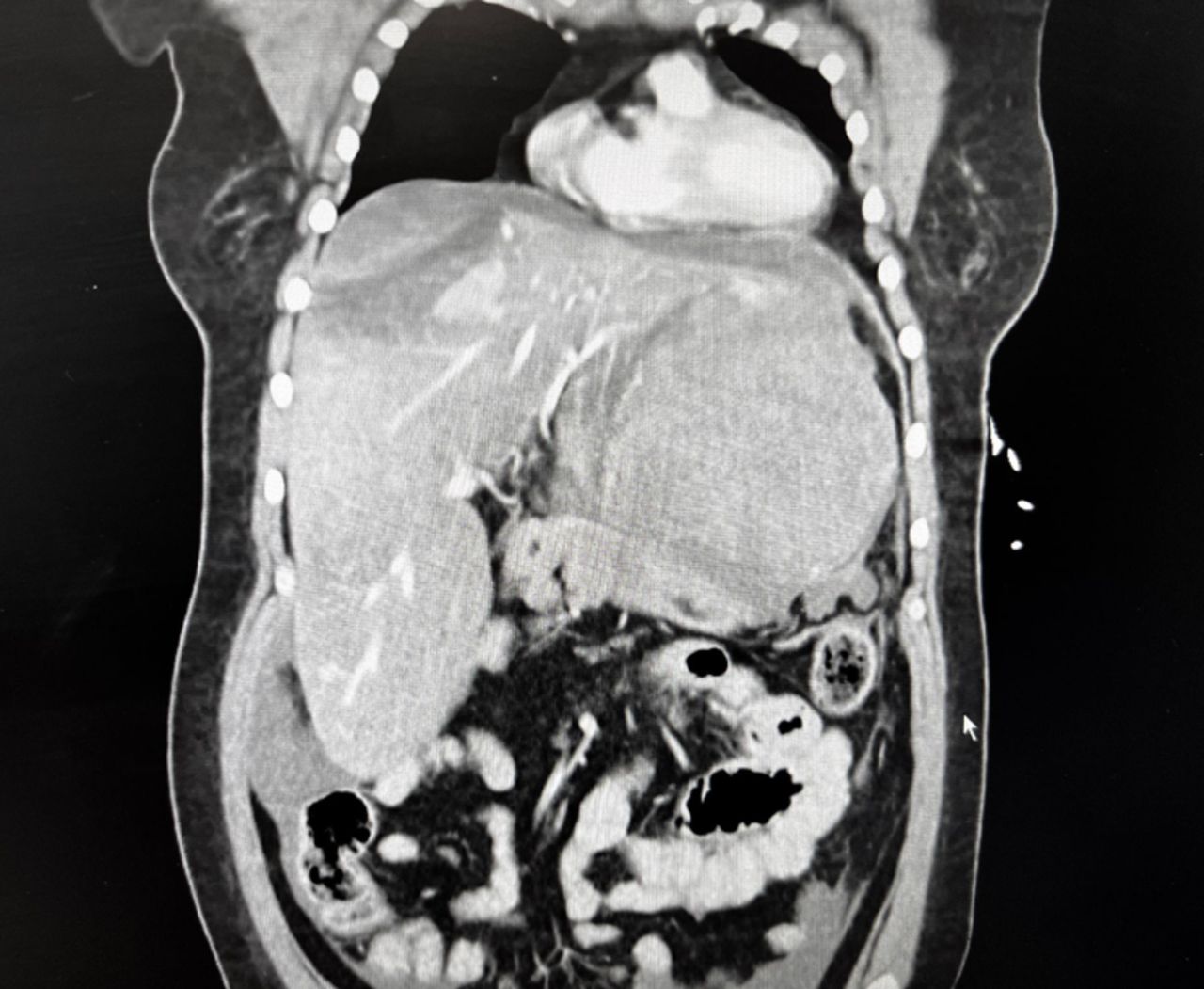
Coronal CT highlighting the ruptured left hepatic adenoma.
What would you do?
Left hepatectomy.
Damage control surgery with perihepatic packing.
Transarterial embolization.
Radiofrequency ablation.
What we did and why
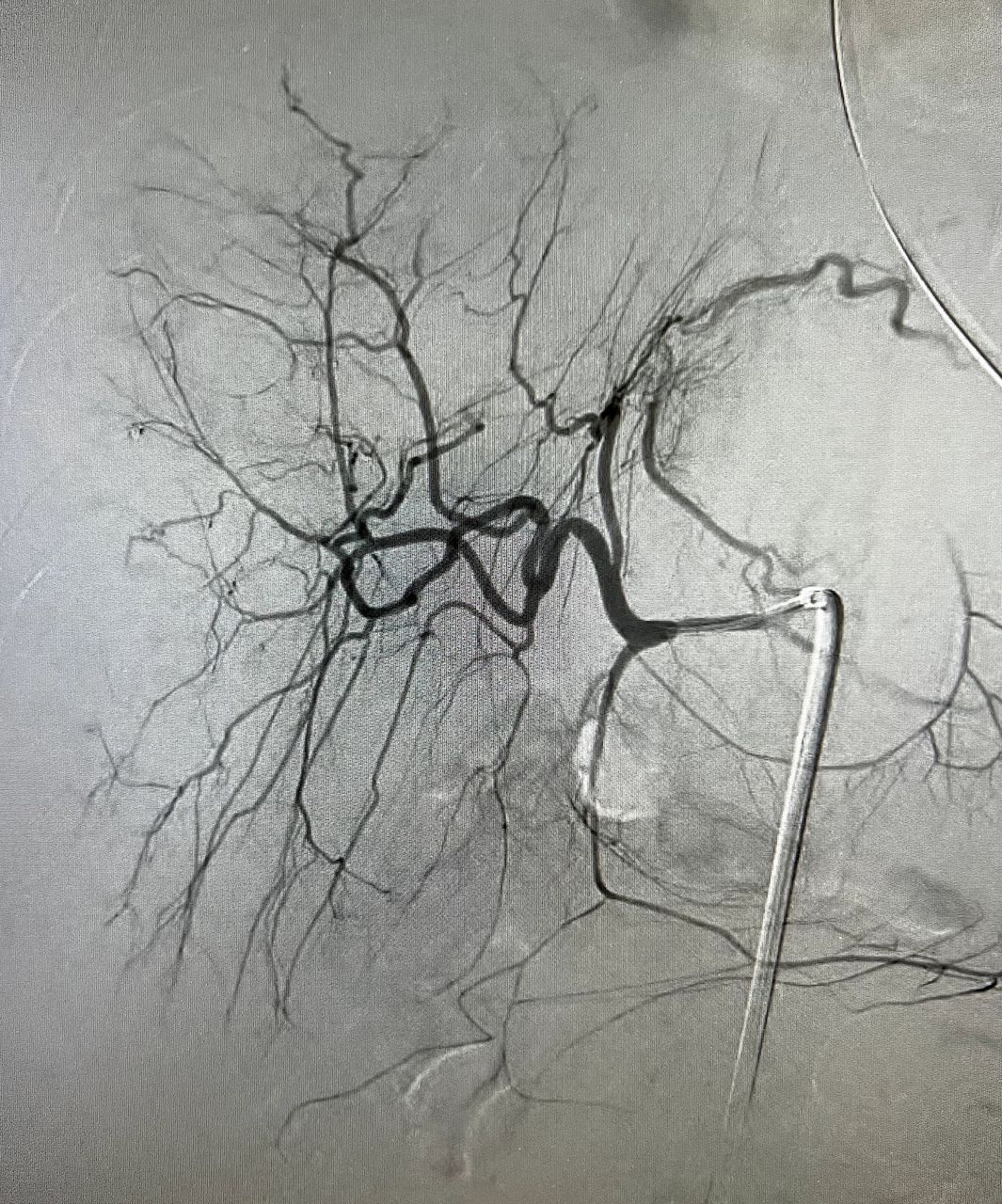
The patient was taken for emergent angiography with possible transarterial embolization (TAE). Transradial angiogram revealed bilateral large hepatic adenomas but no active extravasation (figure 3).

{kind=link}
{kind=link}
{kind=link}
Angiography did not reveal any active contrast extravasation.
Due to hemoperitoneum and continued transfusion requirements, it was decided to transfer the patient to the operating room and convert to an exploratory laparotomy.
During the surgery, 2.5 to 3.0 litres of blood were encountered in the abdomen with clear evidence of rupture of the left hepatic adenoma. The necrotic hepatic tissue was debrided, and packing was used to adequately control bleeding in a damage control fashion.
While the patient was in the intensive care unit, she developed a rebleed and returned to the operating room for an emergent exploratory laparotomy and a left hepatectomy. Delayed primary closure occurred the next day. The patient recovered without complications and was discharged home on postoperative day 10 with instructions to discontinue her oral contraceptive.
The management of hepatocellular adenomas is variable due to significant differences in adenoma size, location, number and presentation. Historically, resection has been used as a decisive way to remove medium to large adenomas and reduce their risk of malignant transformation or rupture. However, over the past 15 years, TAE has emerged as the treatment of choice for acutely bleeding adenomas. Therefore, we initially attempted embolization for our hemodynamically unstable patient before opting for an open procedure.
TAE is particularly recommended in cases where patients are hemorrhaging, largely due to its minimally invasive nature and its frequent ability to obtain hemostasis and decrease tumor burden. Patients controlled originally with TAE may later require elective removal if the adenoma fails to degenerate, but a controlled removal of a stable hepatocellular adenoma is associated with lower morbidity than an open resection of a ruptured adenoma.
Unfortunately, embolization was not successful in stabilizing our patient, highlighting the individualized care often required in the management of hepatocellular adenomas. Additionally, a question can be raised regarding the aspects of our patient’s presentation that resulted in a need for an urgent, open procedure compared with typical cases.
For example, our patient had relatively large adenomas, measuring 9.8×13.9 cm and 9.7×10.9 cm. These adenomas affected both lobes of the liver, a difference from typical cases that are resolved by TAE alone. Finally, our patient had significant medical history including trisomy 21, hypothyroidism, and diabetes, further complicating her presentation. This extensive history is particularly rare when compared with the patient population usually affected by hepatocellular adenomas, young women with presumably few prior medical diagnoses.
Overall, TAE is a well-supported technique in the treatment of hepatocellular adenomas. However, while initial use of TAE is recommended in hemodynamically unstable patients with ruptured adenomas, it is important to not exclude a possible need for more aggressive secondary measures. Potential risk factors for converting to open resection include relatively large adenoma size, involvement of both liver lobes, and pre-existing medical conditions. Further research is required to evaluate the impact of these and other risk factors on the success of embolization.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Contributors AM constructed the case report and performed the literature review. The paper was written and edited by AM, CH, and JT. JD guided the interpretation of literature and final editing. All authors approved the final version and agreed that the article is accurate.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.