Article Text

Abstract
Objectives Prior publications on pediatric firearm-related injuries have emphasized significant social disparities. The pandemic has heightened a variety of these societal stresses. We sought to evaluate how we must now adapt our injury prevention strategies.
Patients and methods Firearm-related injuries in children 15 years old and under at five urban level 1 trauma centers between January 2016 and December 2020 were retrospectively reviewed. Age, gender, race/ethnicity, Injury Severity Score, situation, timing of injury around school/curfew, and mortality were evaluated. Medical examiner data identified additional deaths.
Results There were 615 injuries identified including 67 from the medical examiner. Overall, 80.2% were male with median age of 14 years (range 0–15; IQR 12–15). Black children comprised 77.2% of injured children while only representing 36% of local schools. Community violence (intentional interpersonal or bystander) injuries were 67.2% of the cohort; 7.8% were negligent discharges; and 2.6% suicide. Median age for intentional interpersonal injuries was 14 years (IQR 14–15) compared with 12 years (IQR 6–14, p<0.001) for negligent discharges. Far more injuries were seen in the summer after the stay-at-home order (p<0.001). Community violence and negligent discharges increased in 2020 (p=0.004 and p=0.04, respectively). Annual suicides also increased linearly (p=0.006). 5.5% of injuries were during school; 56.7% after school or during non-school days; and 34.3% were after legal curfew. Mortality rate was 21.3%.
Conclusions Pediatric firearm-related injuries have increased during the past 5 years. Prevention strategies have not been effective during this time interval. Prevention opportunities were identified specifically in the preteenage years to address interpersonal de-escalation training, safe handling/storage, and suicide mitigation. Efforts directed at those most vulnerable need to be reconsidered and examined for their utility and effectiveness.
Level of evidence Level III; epidemiological study type.
- pediatric trauma
- Accident Prevention
- Firearms
Data availability statement
Data may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Pediatric firearm-related injuries disproportionally effect socially disadvantaged groups and remain a significant source of pediatric mortality.
WHAT THIS STUDY ADDS
Pediatric firearm-related injuries have increased during the past 5 years, particularly after the stay-at-home order went into effect.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Prevention opportunities were identified in the preteenage years to address interpersonal de-escalation training, safe handling/storage, and suicide mitigation.
Introduction
Morbidity and mortality from firearm-related injuries spare no demographic. Although gunshot wounds represent a small proportion of all pediatric injures seen relative to adults, they carry a high risk of severe injury.1 2 For American children 17 years of age and younger, unintentional injuries represent 46% of all firearm-related injuries, whereas assaults represent a comparable 44%.3 Male and black children disproportionality represents the vast majority of gunshot victims: 84%–89% and 55%–67%, respectively.4 5 However, given the lethality of intentional injuries, 50% of firearm-related deaths are homicides, 42% are suicides, and only 5% are unintentional.3 White children are more likely to die by firearm-related suicide than other races, thus their overall mortality rate from all gunshot wounds is higher (18% vs. 10% for black children, p<0.001).4 More than half of all pediatric firearm-related injuries occur in families with the lowest quartile of household incomes.5–7 There are significant differences in the distribution of such injuries by geographic region and population density with intentional interpersonal violence being more common in urban settings, whereas unintentional violence and suicides predominate in more rural and southern regions.8 9 National statistics are useful to discuss the scope of the problem, but effective prevention strategies must be tailored to each community. Strategic prevention efforts must be developed first by assessing epidemiologic factors, and reducing pediatric firearm-related injury is no exception.
Firearms in the home are a known risk factor for firearm-related injuries. An increased incidence in fatal firearm injury in the US death rate among 1–4 year-olds paralleled the increasing prevalence of firearms.10 The COVID-19 pandemic saw a record number of firearm sales to both previous and new owners.10 11 Gunshot wounds inflicted on and by young children increased during the first 6 months of the pandemic.11 Several trauma centers reported higher rates of firearm-related injuries during implementation of ‘Stay at Home’ orders (SAHO),12 13 but this was not reproducible in all urban centers.14
These urban disparities were previously reported in the pilot single-center evaluation of pediatric firearm-related injuries, with the majority being black male youth injured as a result of interpersonal violence.15 This initial study was not powered to be able to assess the impact of COVID-19 pandemic-related societal changes like remote learning and changing culture of firearm ownership in 2020. To better hone in on region-wide opportunities for injury prevention, we sought to expand the previous pilot study to surrounding level 1 trauma centers to create a comprehensive picture of the timing and circumstances around these injuries. Secondarily, we wanted to specifically evaluate the impact of the COVID-19 pandemic and SAHO on pediatric firearm-related injuries. We hypothesized that specific patterns may be identified that can guide future injury prevention efforts and an increase in such injuries would be seen during the initial implementation of the SAHO.
Patients and methods
A regional multicenter retrospective comparative analysis was performed at five urban pediatric and/or adult level 1 trauma centers. This project was a collaborative effort through our American College of Surgeons Committee on Trauma state chapter as part of the Chicago for the Surgery of Trauma, Advocacy, & Research (C4STAR) initiative. The Strengthening the Reporting of Observational Studies in Epidemiology statement was followed to report our observational study. Hospital trauma registries were queried for the study’s inclusion criteria: patients 15 years and under who suffered a firearm-related injury between January 2016 and December 2020. This age distinction aligns with the state Department of Public Health definition of pediatric injury. To ensure the most comprehensive assessment, the county medical examiner registry was reviewed for the same inclusion criteria by the coordinating center and cross-referenced. Deaths in the field or deaths that occurred at a non-participating hospital were also included. Deaths that occurred at participating centers were presumed to be included in the hospital data set and thus excluded.
Information collected from the registries included age, gender, and Injury Severity Score (ISS). Electronic medical records were reviewed for reported cause of injury, time of injury, and mortality. The reported circumstances surrounding the injury were divided into the following categories: intentional interpersonal, intentional self-inflicted, negligent discharge self-inflicted, negligent discharge interpersonal, bystander, and unknown. This information was gathered by the data team from free-text narration in admission notes or from supplemental notes from social work, chaplain services, intervention specialists, etc. If the situation was not clear, the final determination was made by the site principal investigator. The study principal investigator processed and made determinations on all the patients with isolated medical examiner data. When possible, reported events were correlated with publicly available reports. Investigators were instructed that any significant discrepancy should be considered as ‘unknown’. Regular study meetings with the study principal investigator for non-identifiable clarifying questions were used to limit variation in classification.
With the known limited accuracy pertaining to the events that lead to the injury, ‘intentional interpersonal’ was defined as the target of the shooting appearing to be the patient or immediately associated with the patient, for example, shots were fired at a group that included the patient. ‘Intentional self-inflicted’ was characterized by suicidal intention. A ‘negligent discharge’ followed the accepted definition of an unplanned firing of a weapon, usually as a result of unsafe handling. These were further divided into ‘negligent discharge interpersonal’ (shooting of a child either by another child or by an adult over 18 years of age) and ‘negligent discharge self-inflicted’. ‘Bystander’ was selected when the intended target appeared not to be associated with the patient, for example, a stray bullet in the street.
Timing of injury was divided into school day versus non-school day based on publicly available dates of the public school system.16 It was further characterized by time of day: during school hours (08:00–15:00 hours on school days), after school hours (15:00 hours to curfew on school days), non-school days (06:00 hours to curfew on non-school days), and after curfew.17 City-wide curfews are mandated based on age and day of the week:
Aged 12–16 years: 22:00 hours on any Sunday through Thursday and 23:00 hours on Friday/Saturday until 06:00 hours of the following day.
Aged 11 years and younger: 20:30 hours on any Sunday through Thursday and 21:00 hours on Friday/Saturday until 06:00 hours of the following day.
Exceptions exist for presences of a parent/guardian and commuting from work; however, given the granularity of the data available, the time cut-offs were used without commentary around the actual legality of potential curfew violations. To assess for seasonal variation, cumulative injuries by month were evaluated. June, July, and August were grouped to represent summer vacation from school and compared with months where school is in session. State-wide SAHO was implemented on March 21, 2020. This date was used to evaluate pre-SAHO and post-SAHO injury rates.
Statistical analysis
Data were collected by each hospital individually into comma-separated variable files. The final data set was then generated combining these files by the coordinating site. All statistical analyses were done using R V.3.5.1 of R Core Team (R Foundation for Statistical Computing, Vienna, Austria, 2018). Descriptive statistics were summarized as frequencies with percentages for categorical variables, and as median with IQR for continuous variables. P values <0.05 were considered statistically significant. Missing and unknown values were reported and excluded from analysis. Comparisons of discrete variables were performed by χ2 analysis. For continuous variables, normality was tested with the Shapiro-Wilk normality test. For non-normally distributed data sets, the Wilcoxon rank-sum test was used to compare groups. For normally distributed data sets, Student’s t-test was used to compare groups. An exponential and linear fit tests were performed on the frequency of injury by age and causes over time. Poisson regression was used to compare the number of injuries that occurred in the summer after the SAHO to those in the preceding summers.
Results
From our registries, 548 patient injuries were identified during the 5-year collection period with a mortality rate of 11.7% (figure 1). An additional 67 firearm-related deaths either in the field or at a non-participating hospital were identified from medical examiner data. This increased the total to 131 deaths in 615 encounters with an overall mortality rate of 21.3%. There were no significant differences in the demographic profiles after adding the medical examiner data. Patients were aged a median of 14 years (range 0–15; IQR 12–15, table 1). There was an exponential increase in numbers injured and numbers killed with each year over age 12 (p<0.001). Gender and racial disparities in the injury burden were clearly seen; injured children were 80.2% male and 77.2% black (9.6% Hispanic, and 7.6% Caucasian, non-Hispanic). Patients had a median ISS of 5 (IQR 1–16).

Flow diagram of inclusion and exclusion numbers. Five hundred and forty-eight patients met inclusion criteria based on hospital registry data and an additional 116 were identified in the medical examiner registry data. However, 49 died at a participating hospital and would have already been in the hospital registry and thus were excluded. Demographic, circumstance, and timing data were available for the analysis of 615 (100%), 478 (77.7%), and 594 (96.6%) incidents, respectively.
Demographic and injury characteristics for 615 pediatric firearm-related injuries
Circumstances were harder to ascertain for deaths in the field reported by the medical examiner. Some centers were more likely than others to report the circumstances surrounding the shooting than others (p<0.001); ultimately 22.3% of circumstances could not be classified. Of those that could, intentional interpersonal injuries comprised 40.8% of all injuries, whereas bystander injuries represented 26.4%. Negligent discharges were 7.8% of injuries: 4.1% by another child, 2.3% self-inflicted, 0.8% by an adult, 0.6% by unknown shooter. Only 2.6% of injuries were intentionally self-inflicted with 13 of the 16 incidences being found only in the medical examiner data and all but one being fatal (93.8% mortality rate). One child died after a police-involved shooting. Median age for intentional interpersonal injuries was 14 years (IQR 14–15) compared with 12 years (IQR 6–14, p<0.001) for negligent discharges. Regarding timing of injury, 37.1% of injuries (n=228) occurred on school days. Overall, 5.5% occurred during school hours, 20% were after school, 36.7% were on non-school days before curfew, and 34.3% occurred after legal curfew. Of the after-curfew shootings, 31.3% (n=66) occurred on school days with the remaining 68.7% (n=145) on non-school days. There were fewer negligent discharges after curfew compared with before curfew relative to the shift in intentional interpersonal shootings, but this did not reach significance (p=0.07).
When fatal injuries were compared with non-fatal ones, no difference was seen in patient gender or in the timing of the injury. Fatal injuries favored a slightly older median age of 15 years (IQR 12–15, p=0.04). In those that completed suicide, the median age was also 15 years, but the youngest reported was 11 years old. Black children were more likely to suffer non-fatal injury (p=0.004). When suicides were removed from the analysis, the racial difference between fatal and non-fatal injuries was no longer significant (p=0.23). Mortality rates significantly changed by circumstance (p<0.001): 93.8% for suicide attempts, 30.7% for unknown circumstance, 20.7% for intentional interpersonal, 14.6% for negligent discharge, and 8.6% for bystander.
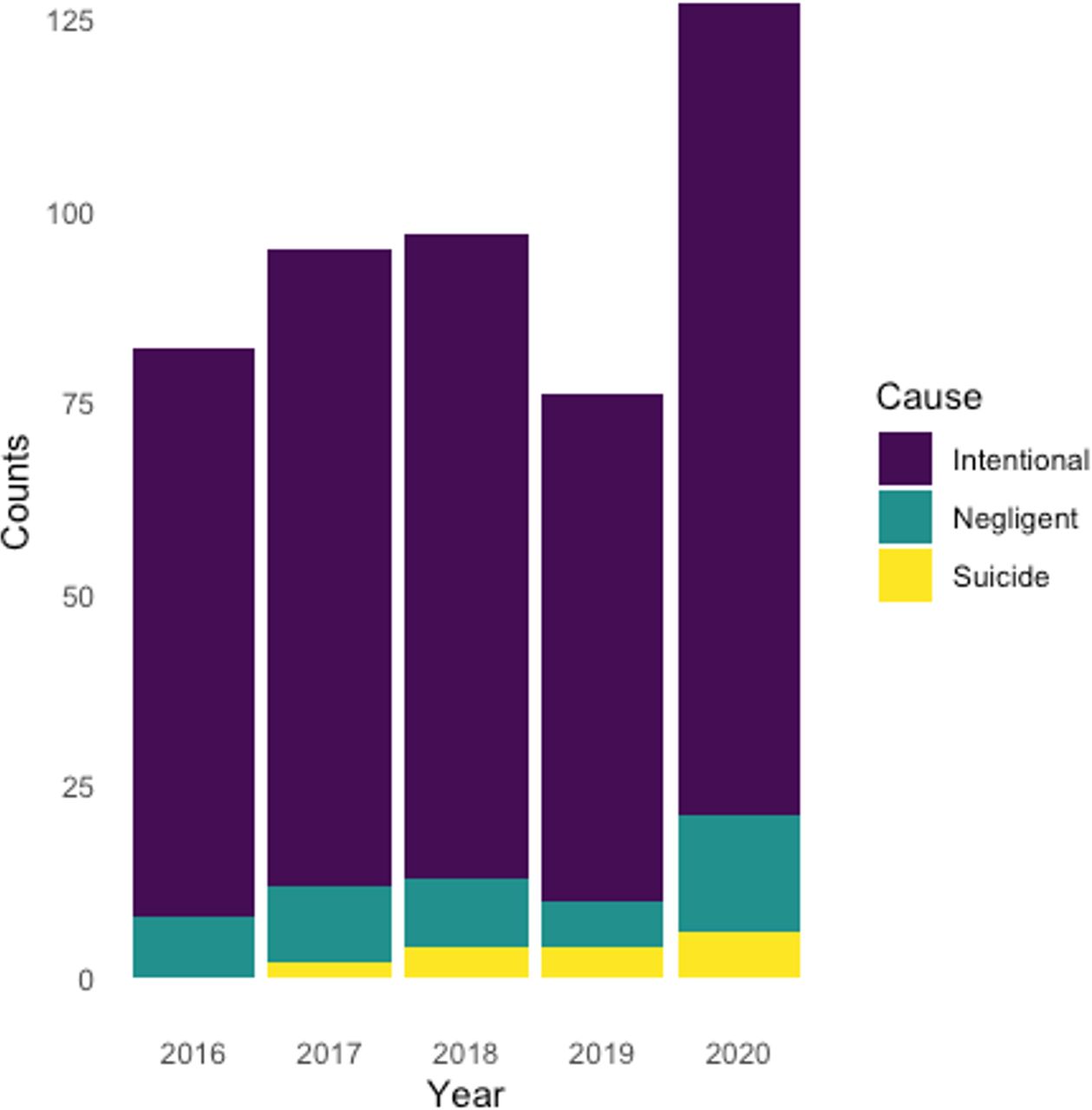
Figure 2 illustrates the number of injuries by month during the 5-year study period with the SAHO designated. An increase in firearm-related injures was seen in the summer after the SAHO (p<0.001). Evaluating the circumstance surrounding injuries over time, a linear increase was seen in intentional self-inflicted injuries (p=0.006, figure 3). There was also a significant increase in combined intentional interpersonal/bystander violence in 2020 (p=0.004) and negligent discharges (p=0.04). Compared with months when school is primarily in session, a seasonal increase is seen over summer vacation in June, July, and August (p<0.001, figure 4). Similarly, a seasonal increase in the number of injuries occurring after curfew also was seen during the summer months (p<0.001).

Pediatric firearm-related injuries by month from January 2016 to December 2020. June, July, and August (red) represent summer vacation months. Pandemic-related stay-at-home order (SAHO) went into effect on March 21, 2020 (green), and an increase in the number of injuries was seen during the summer after the SAHO (p<0.001 by Poisson regression).

Total pediatric firearm-related injuries by year broken down by reported situational cause of the shooting: intentional interpersonal/bystander violence, negligent discharge, or intentional self-inflicted (suicidal intent). There was a statistically significant increase in 2020 in community violence (p=0.004) and negligent discharges (p=0.04). Suicides also increased linearly over the time period evaluated (p=0.006).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Seasonal variation in the number of pediatric firearm-related injuries by month of the year for 2016–2020. Timing further broken down relative to school hours and designated city-wide curfew. A seasonal increase over the summer is seen in both overall injuries (p<0.001) and in those occurring after curfew (p<0.001).
Discussion
The data presented paint an epidemiologic picture that prior prevention efforts have not been able to keep up with the increased injury burden faced by our community’s youth during the pandemic. These data show that new prevention strategies must be undertaken to combat higher rates of interpersonal violence (p=0.004) and rising suicide attempts (p=0.006). Successful public health interventions are designed based on an evidence-based understanding of the scope of the problem, who is impacted by it, the influences that fuel it, and its natural history.18 The data presented reveal a complex network of factors that lead to pediatric firearm-related injuries from negligent discharges that predominate in younger children to increasing intentional interpersonal violence with age, and certainty also not exclusive of death by suicide. Organizations can use these data to focus on injury prevention efforts based on this understanding and double-down given the ground lost during the pandemic.
One of the difficult aspects of placing pediatric firearm-related trauma studies into context is the lack of standardization of what constitutes a pediatric patient and the situations surrounding the injuries. During adolescence, firearm injuries increase with age with only a reported 26% of injuries in legal minors being in our evaluated ages of under 16 years.5 A national 7-year evaluation of firearm-related emergency department visits found on average approximately 1633 visits/year for those 14 years old and younger.6 Our regional study found 70 visits/year in that same age range, representing 4.3% of the national data set presuming stable injury rates by year. This number considerably outpaces previously published data from a similar urban center with 19 injuries per year for ages under 20 years.19 We also report an overall mortality rate of 11.6% on hospital data alone for those 15 years and younger, which was more than a single-center trauma registry study that reported a mortality rate of 8% in those 17 years and younger.20 In a national hospital database review, firearm-related mortality for those aged 0–6 years was 6%,7 whereas we report an overall 18.3% mortality in that age group. However, our overall mortality rate rose dramatically to 21.2% with inclusion of the medical examiner data. Out-of-hospital firearm-related deaths must be represented.6 Studies should strive to be as comprehensive as possible to accurately represent the depth of this public health crisis and best guide injury prevention strategies.
Gender and race disparities within firearm-related injuries have been well described. Our study found 80.3% of injuries involved males, which was comparable with the previously reported 74%–84.2% male predominance.4 21 22 We found that 77% of injured children were black, disproportionally higher than the racial composition of our region’s public schools (46.6% Hispanic, 35.9% black, 10.8% Caucasian non-Hispanic).23 We have clearly yet to stem the increasing tide of firearm-related assaults on black children.24 While we only reported one clear firearm-related injury involving a police-related shooting (in a black youth), one must note that adolescent firearm-related deaths involving law enforcement intervention are thankfully rare but also disproportionally effect black children.25
When critically evaluating such large-scale epidemiologic data, it is crucial to understand that firearm-related assaults and homicides are a different entity than firearm-related suicides that primarily effect a different demographic. A cursory evaluation of our data would suggest that black ethnicity carried a reduced risk of fatal injury. However, similar to a previously reported study, this appears to be driven by highly lethal intentional self-injury that occurs at a higher rate within Caucasian race.4 This study demonstrated a 62.6% mortality rate of intentional self-inflicted injuries, while we found it to be 93.8% in our region.4 Another national report of firearm-related injuries found that while attempted suicide cases comprised only 3% of all injuries, they represented 41.9% of all firearm-related deaths.3 With the youngest child to complete suicide being 11 years old, interventions must seek to reduce the stigma surrounding mental healthcare, remove access to firearms for at-risk children, and importantly not ignore preteenage children.
For additional prevention opportunities, we must also understand the circumstances surrounding the injury of victims of interpersonal violence and negligent discharges. An evaluation of the National Trauma Databank for those 19 years old and younger demonstrated that 76% of firearm-related injuries were assaults, 14% were unintentional, and 5% were self-inflicted.22 A single-center study of 115 patients under 18 years of age during a 6-year period reported 37% of injuries were intentional assault-related injuries, whereas 57% were ‘crossfire’ injuries and 6% were from negligent discharges,20 compared with 43.9%, 20.4%, and 8.1% in our data set, respectively. Such distinction is difficult to ascertain with complete accuracy from the review of the medical records and must be interpreted with this in mind. It may be appropriate in certain circumstances to combine intentional interpersonal violence and bystanders into the distinction of ‘community violence’. Unsurprisingly, we found that intentional injuries carried a higher mortality rate than unintentional injures (p<0.001). A single-center study found that unintentional injuries were more likely to occur during the day, whereas injuries from interpersonal violence were more likely at night (p=0.01).26 A paired pediatric and adult trauma center reported that 51% of those 14 years and younger were shot on Friday, Saturday, or Sunday, and 70% were shot between 16:00 and 04:00 hours.21 The majority of those in our evaluation were shot during the non-school day or after curfew. Truancy represented a measurable but small proportion of injuries. Summer vacation months are known to have higher rates of firearm-related injures.26
The COVID-19 pandemic, school shutdowns, and remote learning changed the epidemiology of pediatric injury. While shelter-in-place policies led to a 13% decrease in overall pediatric trauma volume nationally, gunshot wounds increased, and injury severity was higher among the shelter-in-place cohort compared with controls.27 Multiple national studies have shown an increased number of injuries against and by children during the start of the COVID-19 pandemic.11 28 29 Self-inflicted pediatric shootings have been increasing,30 31 supported by our findings of a linear increase over the time period examined. Decreased parental supervision during remote learning may increase unintentional injury rates.32 33 A national survey in 2015 revealed that approximately 20% of gun-owning households with children stored at least one weapon loaded and unlocked, and this is increased from a previous report.34 The start of the pandemic saw increasing new firearm acquisitions.11 In a survey of homes with teenagers, new purchases were more likely to go to home where at least one weapon was already stored loaded and unlocked.35 Over 60% of prior firearm owners, who purchased additional weapons during the pandemic, stored at least one weapon unlocked.36 Of those who changed storage practices during the pandemic, desire to reduce access by children was the most common reason cited.36
Our study was limited in its accuracy given self-reported situations surrounding the firearm-related injury and inconsistently recorded information by center. We were not able to access police records to provide collateral information. We sought to include all regional level 1 trauma centers; however, one center had internal issues with accessing registry information and was unable to participate. Several other centers had less than one injury per year and elected not to participate. Based on a previous evaluation of resource allocation, it is thought that we were able to capture over 90% of regional injuries. Using medical examiner data ensured that all deaths within the county should have been included. As such, the only missing data would be in survivors which might result in a slight overestimation of the mortality rate. This limitation is nearly ubiquitous in all epidemiologic evaluations of firearm-related injuries, and a central database with healthcare encounters regardless of trauma center designation as well as medical examiner data would improve the quality of such studies.37 Given the deidentified nature of data collection, recidivism could not be assessed. Local hospital-based violence intervention program (HVIP) data, however, suggest that 45% of those who are shot will be shot again within 5 years (internal data). As such, efforts should be focused both on primary and secondary injury prevention. Further, the effects of social determinants of health (SDH) could not be captured in this study. HVIPs within the city do capture and work to address them, and prospective evaluations of interventions should be designed to measure impacts on SDH. Timing of injury was estimated by time of arrival at the hospital and delayed presentations may not be captured. As mentioned, injury after curfew does not necessarily mean curfew was violated as there are exceptions allowing for minors to be out and some shootings occurred at home. Circumstances collected through medical or public record may be limited in accuracy of reporting. In this evaluation, subacute presentations from outside hospitals were included in the analysis. It is speculated that a number of firearm-related injuries go untreated, and the true incidence may be higher than actually reported. While those with significant physical impact are more likely to be seen at a hospital, the psychological impact of being shot, even if just a flesh wound, cannot be ignored. In 21% of cases, the situation was unknown and there may have been variation on how this distinction may have been determined from the medical record. Finally, this dynamic epidemiologic evaluation cannot comment on the efficacy of specific prevention efforts that occurred during the study period.
Call to action
Pediatric firearm-related injury prevention strategies need to address the following areas.
Unintentional injuries primarily effect younger children and are often related to unsafe storage and handling practices.38 As trauma providers, we should advocate for trauma-informed screening and counseling of families with young children on firearm ownership and storage with a non-judgmental focus on evidence-based prevention strategies.3 39 40
Suicides can occur in the preteenage groups and are more common in rural and socially advantaged areas. Efforts must be made to expand mental healthcare, reduce stigma, and educate on lethal means.
Interpersonal violence disproportionally effects socially disadvantaged groups and is more often to occur during summer months and later in the day.41 Structural racism and SDH of health must be addressed through trauma-informed counseling of our patients and our communities through partnerships with both hospital-based and community-based violence intervention programs.42–44
Well-laid-out framework for public health approaches to advocacy and prevention but has been minimally successful translating into legislative changes or federal funding.3 45 46 States with stricter firearm regulation and child access protection laws have lower pediatric firearm-related mortality rates28 47–49; however, a proper evaluation of the legal aspect of prevention is beyond the scope of this article. Trauma and pediatric providers should be empowered to educate themselves and advocate for the health of their patients through the lens of trauma prevention.43 50 This should include funding for more comprehensive data collection repositories.
Conclusions
Children are suffering firearm-related injuries at an increasing rate. We have lost ground during the pandemic. Community violence and negligent discharges increased in 2020. We need to double-down on multifaceted prevention initiatives beginning in the preteenage years and include safe handling/storage, suicide mitigation, and interpersonal de-escalation training. Additionally, attention and funding should be focused on building a more robust firearm-related database including trauma centers, non-trauma centers, and medical examiner data to improve the quality of research moving forward.
Supplemental material
Data availability statement
Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by an ethics committee(s) or institutional review board(s). Primary: Cook County Health (IRB 20-031). Secondary: IRBs approved at all participating sites and DUAs obtained.
Acknowledgments
The authors acknowledge the efforts by our trauma surgery, pediatric surgery, and emergency medicine colleagues for their excellent care of our youngest patients. In particular, the authors acknowledge the efforts of our hospital-based and community-based violence intervention program partners for their tireless work in injury prevention and recovery. A special thank you as well to Fae B Kayarian, BS (Rush University), who assisted with the literature search, Jared Ourieff, DO (Mount Sinai), who assisted with data extraction, and Ann Ezzell, BS, for assistance with graphic design.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Press release
Footnotes
Presented at Oral presentation at 51st Annual Meeting of the Western Trauma Association, February 20–25, 2022, held in Big Sky, Montana.
Contributors LCT, JTC, MBS, GC, AS, JD, VS, and AJD created the study design. LCT, MJ, and AJD performed the literature search. All authors participated in data collection. LCT analyzed the data. LCT and AJD wrote the article. All authors participated in data interpretation and critical revision of the article. LCT is the guarantor of overall content.
Funding Monies for this project were acquired from a discretionary departmental fund. No funding was received for this work from the National Institutes of Health (NIH); Wellcome Trust; or the Howard Hughes Medical Institute (HHMI).
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.