Article Text

Abstract
Objectives Vasopressors are a cornerstone in the management of sepsis, marked by distributive shock often unresponsive to fluid resuscitation. Prior research and clinician surveys have suggested that earlier usage of vasopressors corresponds to improved outcomes.
Methods A retrospective cohort was constructed using patient data contained within the Medical Information Mart for Intensive Care-IV database. Analytic cohort included a total of 2079 patients meeting sepsis-3 criteria with a ≥2-point rise in Sequential Organ Failure Assessment score and administered norepinephrine (NE) as first-line vasopressor within 24 hours of admission to the intensive care unit (ICU). Patients receiving other vasopressors or missing documented fluid resuscitation information were excluded. Primary end points included mortality, use of invasive mechanical ventilation and length of stay which were analyzed in a multivariate logistic regression model for the primary effect of time from ICU admission to NE administration using covariates.
Results Time to NE use was defined as either early, using <6 hours from time of ICU admission or late using >6 hours to ≤24 hours. Patients who received early NE had significantly lower adjusted odds of mortality (0.75, 95% CI 0.57 to 0.97, p=0.026), higher adjusted odds of invasive mechanical ventilation (1.48, 95% CI 1.01 to 2.16, p=0.045), no significant difference in hospital length of stay (difference in days 0.6 (95% CI −3.24 to 2.04)) and lower ICU length of stay (difference in days −0.9 (95% CI −1.74 to –0.01)), as compared with the late NE group.
Conclusion Among patients admitted to the ICU for sepsis, early use of NE was associated with significantly lower odds of mortality but higher odds of mechanical ventilation, and no significant difference in length of hospital stay but less time in the ICU. Furthermore, the volume of fluids received prior to NE use may have a significant impact on optimal NE timing.
Level of evidence Level IV—therapeutic care/management.
- critical care
- sepsis
- resuscitation
- shock
Data availability statement
Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Early evidence, the Surviving Sepsis Campaign and physician practice surveys suggest that earlier use of vasopressors, even via peripheral lines may be optimal.
Although current practice and guidelines support this, there is no current specification of how much and when to administer them.
WHAT THIS STUDY ADDS
Using the Medical Information Mart for Intensive Care-IV database, this study is able to analyze the outcomes of early versus late norepinephrine administration and quantity of fluids during sepsis to better understand how much and when treatment should be initiated for patients.
This study adds to the building evidence that early administration of norepinephrine for sepsis reduces rates of mortality and length of hospital stay, irrespective of norepinephrine administration method or the amount of fluids given to patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study may add support to the importance of early norepinephrine use in patients with sepsis, help to guide sepsis protocols in hospitals and stimulate further research into the interaction between fluid use and vasopressor use.
Introduction
Sepsis is a common reason for intensive care unit (ICU) admission and a leading cause of death worldwide.1 2 Available literature suggests that sepsis accounts for >50% of in-hospital mortality annually, and those who survive develop long-term complications.3 4 Although mortality due to sepsis has steadily declined since 1991, its incidence has continued to rise and currently one-third of all ICU admissions are related to sepsis.5 This increasing incidence and prevalence of sepsis in US hospitals costs the healthcare system approximately US$24 billion annually, making it the most expensive condition to treat in the US healthcare system.6
Sepsis is organ dysfunction secondary to a dysregulated inflammatory response to infection and is often defined as a 2-point increase in Sequential Organ Failure Assessment (SOFA) score, while septic shock is ‘clinically identified by a vasopressor requirement to maintain a mean arterial pressure (MAP) of 65 mm Hg or greater and serum lactate level >2 mmol/L in the absence of hypovolemia’.7 Early detection and initiation of treatment is crucial, as sepsis causes major systemic instability and rapid deterioration often leading to death.8 Thus, patients identified with sepsis in the emergency room have poorer outcomes when they are faced with prolonged wait times causing delay in transfer to the ICU and treatment. A study in 2001 targeted toward early goal-directed therapy (EGDT) of sepsis created a systemic approach to early management in the emergency department, thereby alleviating the negative impacts of prolonged wait times—this led to improved efforts in early recognition and management of sepsis.9 These early efforts are crucial in improving the odds of survival for these patients and follow-up trials after EGDT, including Protocolized Care for Early Septic Shock (PRoCESS), Australasian Resuscitation in Sepsis Evaluation (ARISE) and Protocolised Management in Sepsis (PRoMISe), demonstrated that mortality significantly improved in both the treatment and control arms.10–12 There is evidence that improved mortality is due to increased awareness of sepsis since the early 2000s and not necessarily the EGDT protocol.11 This goal-directed management involving optimization of cardiac preload, afterload and contractility is currently used as the definitive resuscitation strategy in sepsis management.
As part of this strategy, patients are administered vasopressors to restore an adequate systemic vascular resistance that is often lacking in these ‘warm’ vasoplegic distributive shock patients. Current recommendations include starting vasopressors peripherally to restore MAP rather than waiting for a central venous access, and use of norepinephrine (NE) as a first-line agent.13 Delay in vasopressor initiation after 6 hours of sepsis detection is shown to increase 30-day mortality.14 Early NE administration to hypotensive patients with sepsis achieves target MAP earlier and decreases fluid overload which commonly complicates resuscitation efforts and hence decreases mortality rate.15
Although there are no definite guidelines for exact timing of initiation of vasopressor use with respect to time from admission or fluid status in septic shock patients, studies show early management of deteriorating MAP with vasopressors leads to better overall outcomes.14 This retrospective cohort study using a well-curated database aims to further analyze the outcomes of patients with septic shock who received early versus late treatment with NE and further to investigate the impact of the quantity of fluid resuscitation prior to NE administration on sepsis outcomes.
Methods
This study was designed using retrospective cohort of patients with sepsis admitted to the ICU obtained from the Medical Information Mart for Intensive Care (MIMIC-IV), a freely available database of ICU stays from ICUs in the Beth Israel Deaconess Medical Center from 2008 to 2019 accessible via Physionet.16 From this database, patients were included in the analytic cohort if they were admitted with a sepsis diagnosis based on the sepsis-3 definition, demonstrated a rise in SOFA score of ≥2 points, and received NE within 24 hours of their ICU stay.7 Patients who received other vasopressor agents prior to NE (epinephrine, dopamine, vasopressin, dobutamine and phenylephrine), and subjects without data available on fluids received were excluded from the study.
Our primary end points included mortality, ICU length of stay and need for invasive mechanical ventilation (IMV) in patients who were not already intubated prior to NE administration. Our primary predictor variable was time from ICU admission to first use of NE as measured in hours. A co-primary predictor variable was the volume of intravenous resuscitative fluids (normal saline, lactated ringers or colloid boluses) measured in kilograms per hour given prior to receiving NE. Additional covariates of age, ethnicity, comorbidities, risk scores (Acute Physiology Score [APSiii], Simplified Acute Physiology Score [SAPSii], Sequential Organ Failure Assessment [SOFA], Oxford Acute Severity of Illness Score [OASIS]) were also selected for analysis. Furthermore, we included data on central versus peripheral line use for NE administration, rates of IMV and collected positive culture sources for cause of sepsis in each patient where these data were available. Patients were split into early vasopressor and late vasopressor groups based on a previously used cut-off of 6 hours from ICU admission to NE administration.
Univariate statistics were calculated for each variable between groups using the most appropriate statistical test (t-test for continuous normal variables, Mann-Whitney U test for non-normal continuous variables and Fisher’s exact test for categorical variables). Those variables which significantly differed between groups (at a significance threshold of <0.1) were used as covariates in multivariate models evaluating early and late NE administration on each outcome (logistic regression for binary outcomes and linear regression for continuous outcomes).
We then split the cohort into groups based on quartiles of both fluids per kilogram per hour and for time to NE . We evaluated the effect of early and late NE use within these groups using multivariate models as in our primary analysis, including only covariates which differed significantly in univariate analysis. R-Studio V.4.1.2 and Jamovi V.2.3.21 was used for all statistical analysis and p values of <0.05 were considered statistically significant in our final multivariate model.17–21 Missing data were omitted listwise. No adjustments for multiple comparisons were made.
Results
There were 13 515 patients who met the criteria for sepsis-3, received NE and had a ≥2-point rise in SOFA score. After excluding patients who received pressors other than NE, patients who had missing fluid volume information and considering only patients receiving NE within 24 hours of ICU admission, a total of 2079 patients were available in the analytic cohort. The cohort was dichotomized based on a 6-hour cut-off from ICU admission to NE administration. The early NE group contained 1045 patients while the late NE group contained 1035 patients. Baseline characteristics were calculated between groups using the appropriate statistical tests. On univariate analysis, the following variables differed between groups (p<0.1): rheumatic disease, first day SOFA score, OASIS score, APSiii score, SAPSii score, first ICU stay, central line placement, mechanical ventilation prior to NE and fluids per kg per hour (table 1). For the primary outcomes analyzed in univariate analysis, the following outcomes were significantly different on univariate analysis (p<0.05): morality, IMV, ICU length of stay (table 1). Patients with the central lines had significantly lower mortality in the early NE group versus the late NE group (15.4% vs 21.7% p=0.0041) and those without central lines had non-significantly lower mortality in the early NE group versus the late (14.4% vs 19.6% p=0.078).
Baseline characteristics of early and late NE groups
Positive culture data were collected for 779 patients among the entire cohort. The highest proportions of positive source cultures were obtained from blood (235 patients, 11.3%), sputum (162 patients, 7.8%) and urine (146 patients, 7.0%) (online supplemental table 1). Statistically significant differences were observed between early and late NE groups for the following cultures: urine (5.7% vs 8.3% p=0.022), tissue (0.5% vs 1.4% p=0.036), blood (13.1% vs 9.5% p=0.0091) and Staphylococcus aureus screen (0.1% vs 0.7% p=0.032) (online supplemental table 1).
Supplemental material
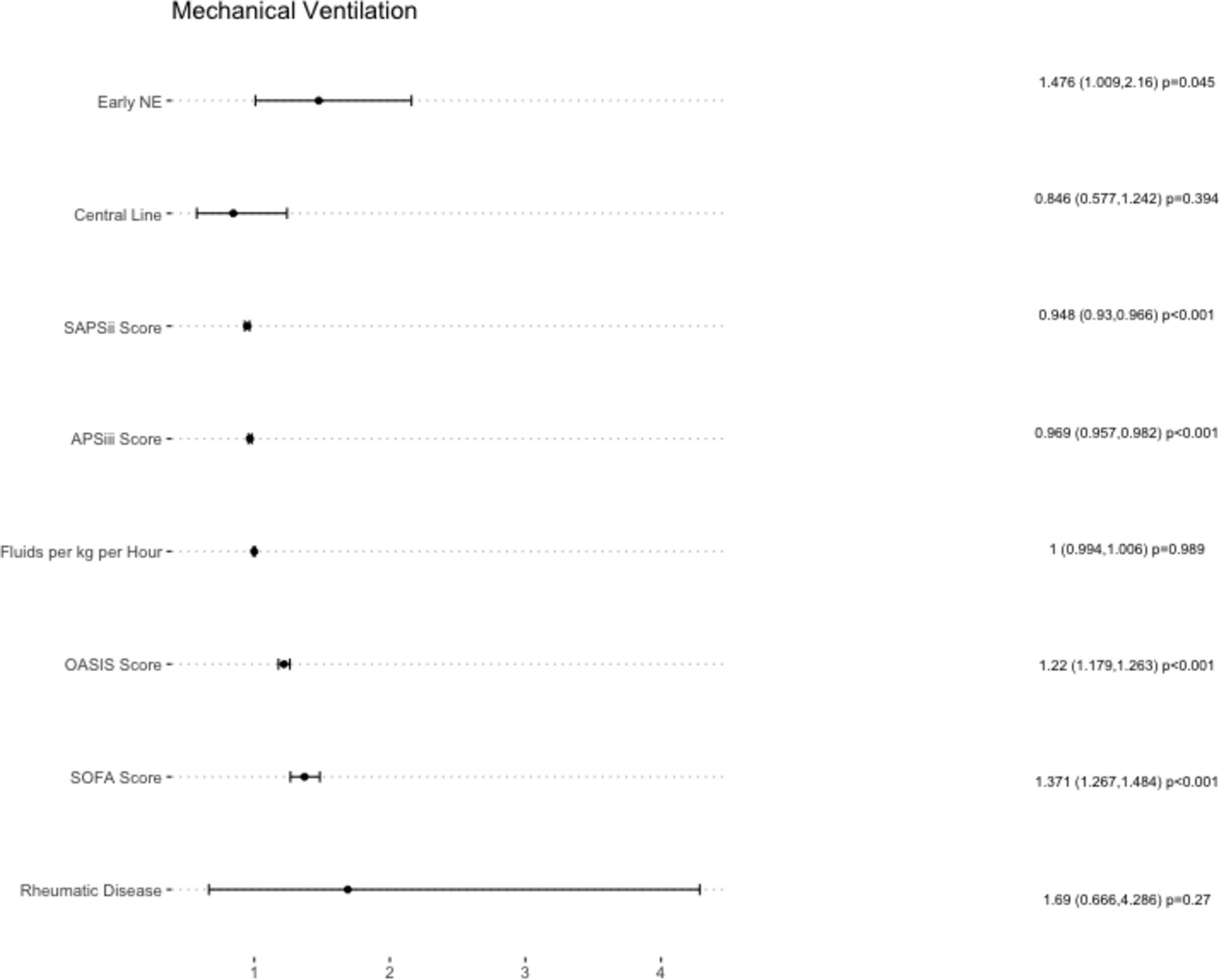
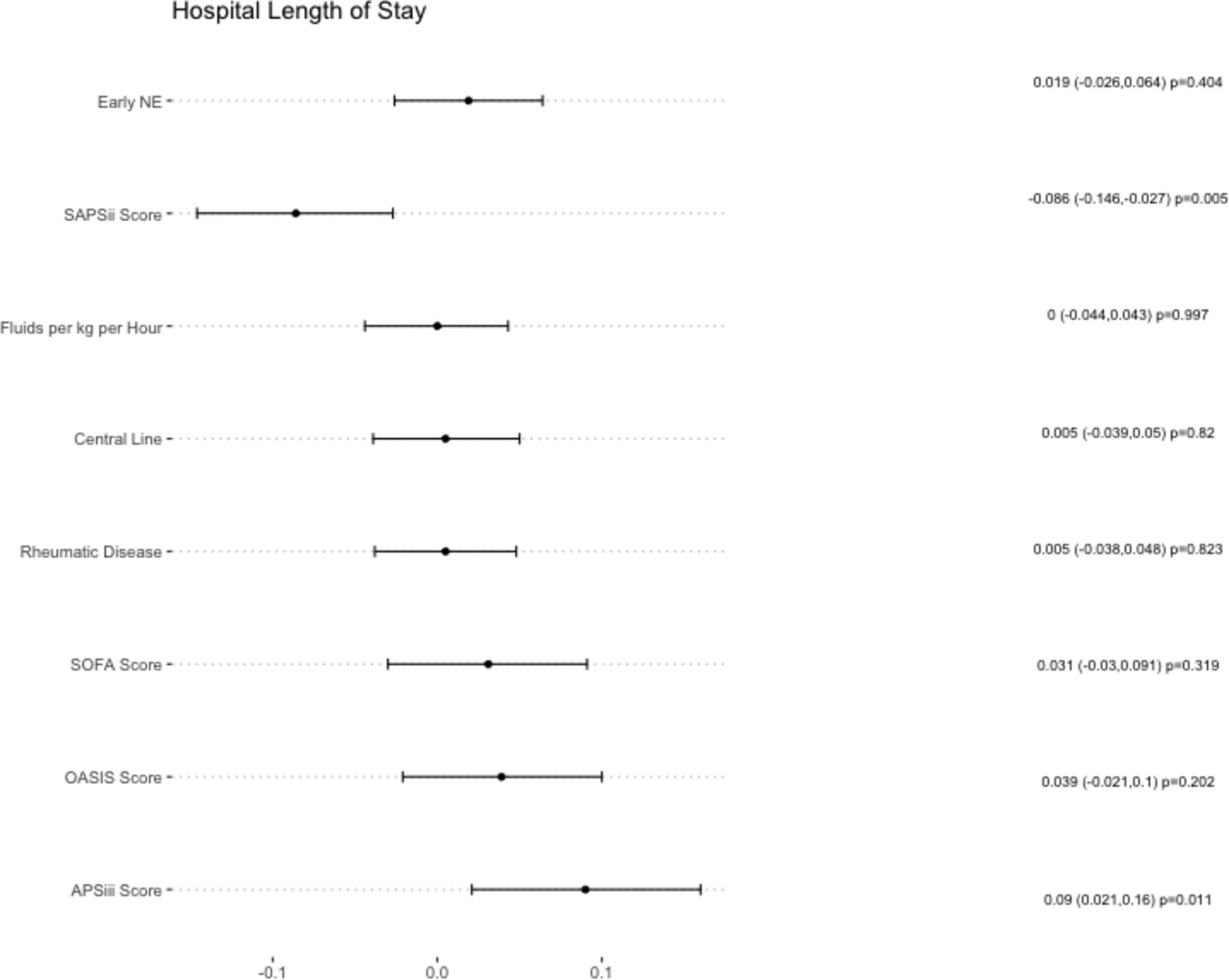
Multivariate logistic regression showed that patients in the early NE group had 0.75 (95% CI 0.57 to 0.97) (reported as OR, OR with 95% CI) times decreased risk of 28 days in hospital mortality (table 2, figure 1) and 1.48 (95% CI 1.01 to 2.16) (OR) times increased risk of requiring IMV among patients who were not already requiring IMV (table 2, figure 2). Patients in the early NE group had no significant difference in hospital length of stay (difference in days 0.6 (95% CI −3.24 to 2.04)) (table 2, figure 3) and lower ICU length of stay (difference in days −0.9 (95% CI −1.74 to –0.01)) (table 2, figure 4).
Early versus late NE association with outcomes in multivariable logistic regression or linear regression models

Adjusted ORs of 28-day mortality logistic regression model covariates. NE, norepinephrine; SOFA, Sequential Organ Failure Assessment.
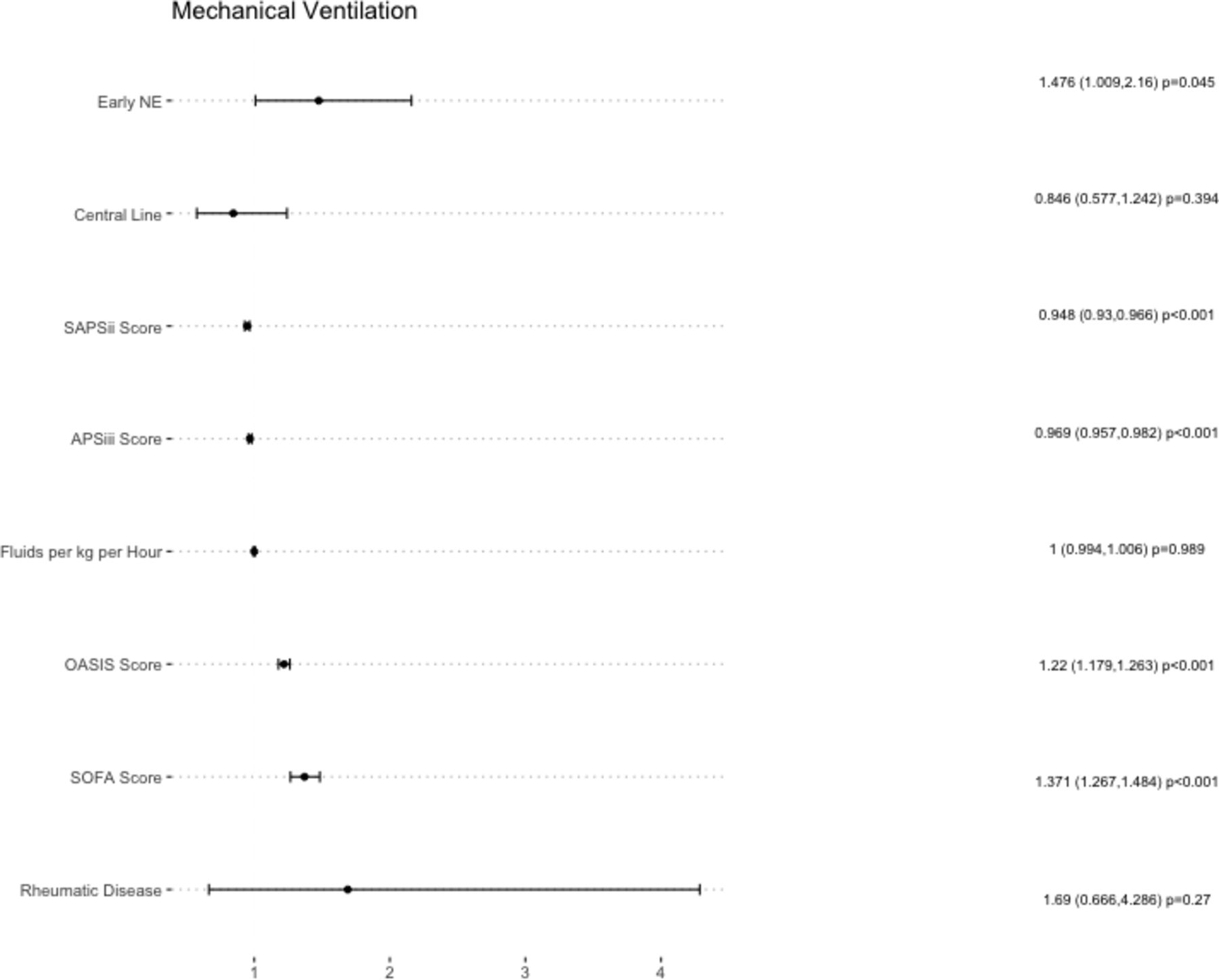
Adjusted ORs of invasive mechanical ventilation logistic regression model covariates. NE, norepinephrine; SOFA, Sequential Organ Failure Assessment.

Standardized estimate of hospital length of stay linear regression model covariates. NE, norepinephrine; SOFA, Sequential Organ Failure Assessment.
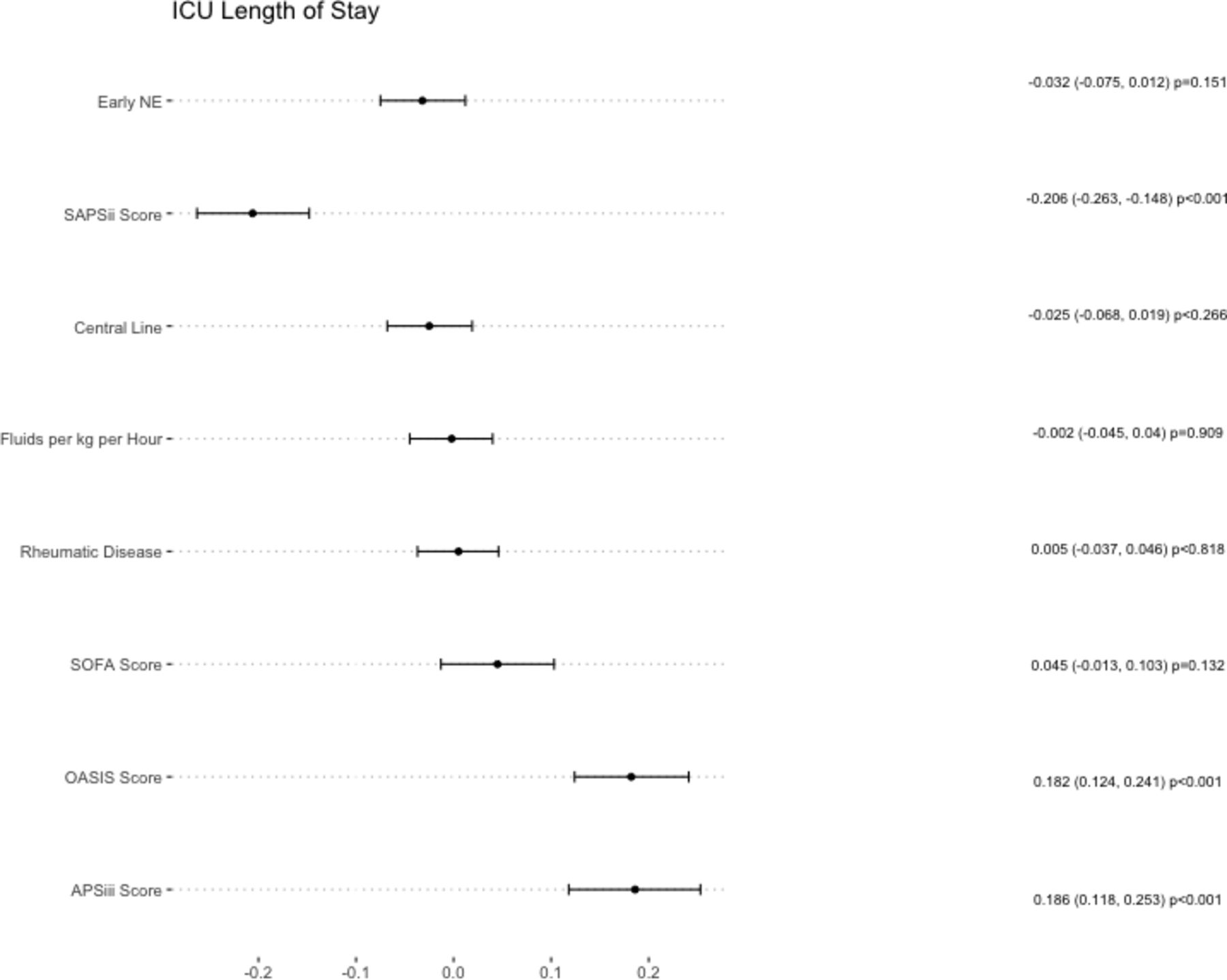
Standardized estimate of ICU length of stay linear regression model covariates. ICU, intensive care unit; NE, norepinephrine; SOFA, Sequential Organ Failure Assessment.
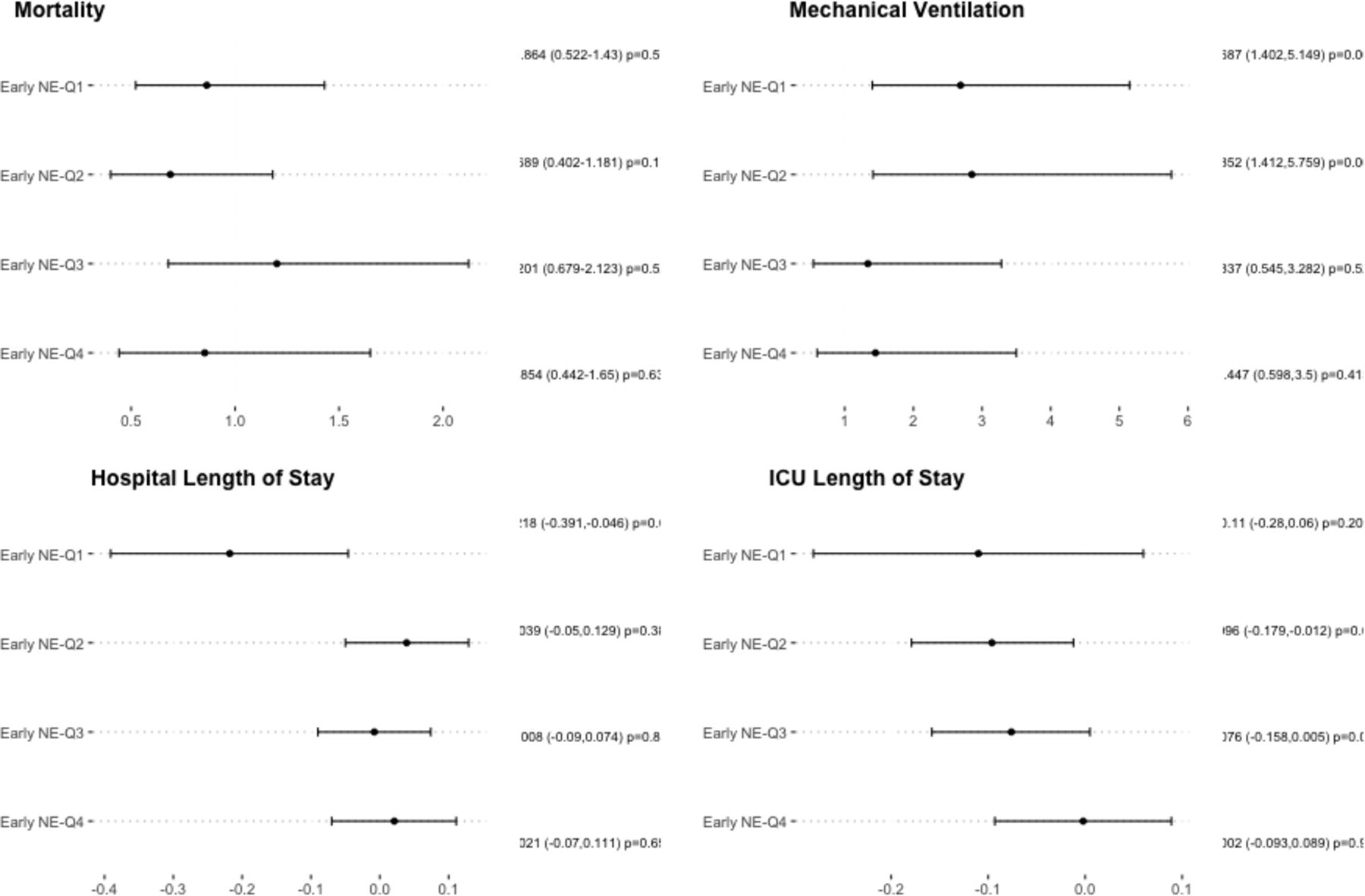
Patients were then placed into quartile groups based on the volume of fluids received per kilogram per hour prior to NE administration. Quartile 1 consisted of patients receiving <0.815 mL/kg/hour, quartile 2 consisted of patients receiving between 0.815 mL/kg/hour and 2.334 mL/kg/hour, quartile 3 consisted of patients receiving between 2.334 mL/kg/hour and 5.075 mL/kg/hour and quartile 4 consisted of patients receiving >5.075 mL/kg/hour of fluids. For each group, multivariate logistic regression or linear regression was used to assess the effect of early versus late vasopressor use on primary outcomes. Figure 5 shows that there was no statistically significant difference in mortality in any of these fluid quartiles, however in quartiles 1, 2 and 4 the ORs were 0.864, 0.689 and 0.854, respectively while in quartile 3 the odds of mortality was 1.201. Patients in quartiles 1 and 2 of fluids had significantly higher odds of IMV (2.687 (95% CI 1.402 to 5.149) and 2.852 (95% CI 1.412 to 5.759)) while in quartiles 3 and 4 there were increased odds of IMV which was not statistically significant (1.337 and 1.447). Patients in quartile 1 in the early NE group had significantly lower hospital length of stays (difference in days −4.9 (95% CI −7.80 to –0.99)) while in all other quadrants, there were no statistically significant differences in hospital length of stay, although ICU and hospital length of stays were higher. Patients in quartile 2 in the early NE group had significantly lower ICU length of stays (difference in days −1.70 (95% CI −2.82 to –0.58)) while in other groups there were lower ICU length of stays which did not reach statistical significance (figure 5). Additional outcomes as well as characteristics of patients in each quartile may be found in online supplemental tables 2–9.

Outcomes in late versus early NE groups by multivariate logistic or linear regression, stratified by total volume of fluids per kg per hour given before vasopressors, expressed as quartile groups. ICU, intensive care unit; NE, norepinephrine.
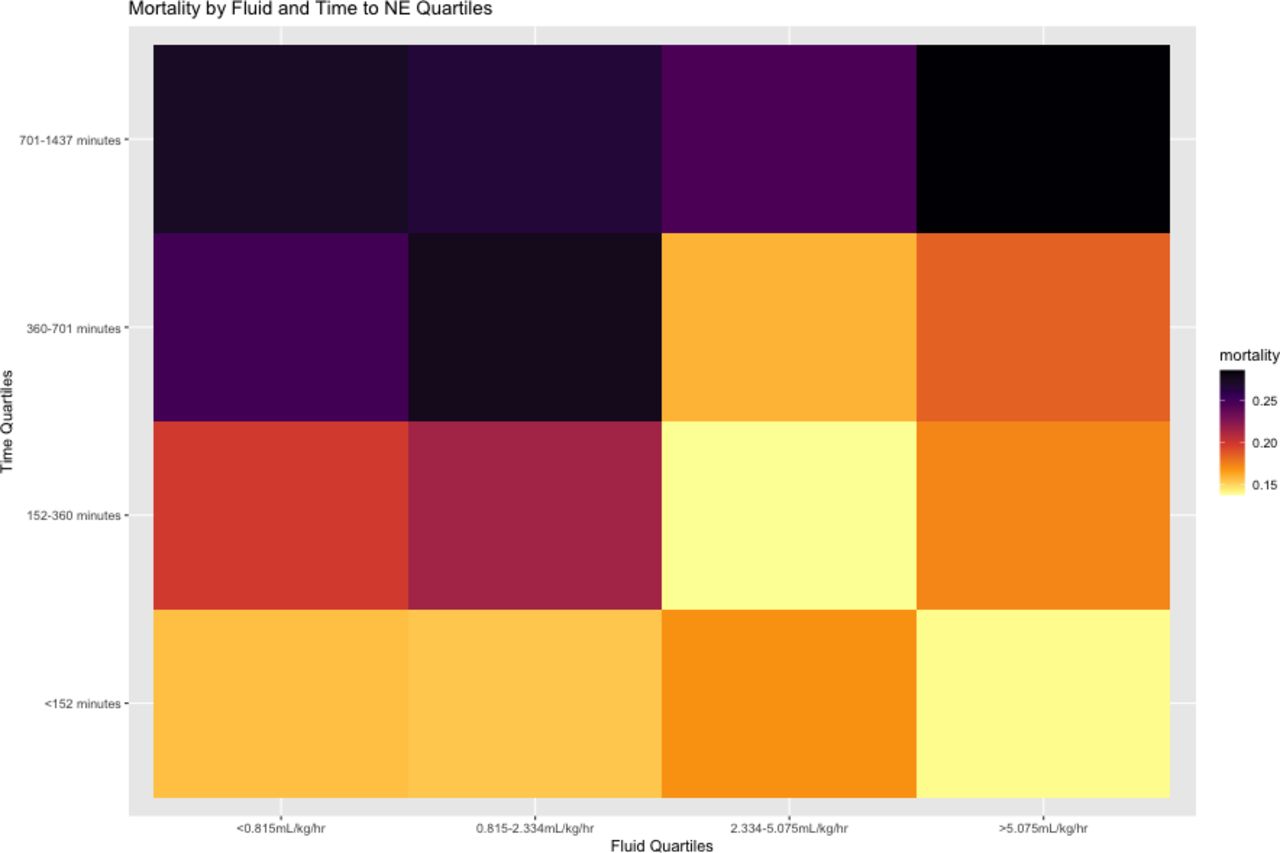
To further explore the effect of NE timing and volumes received, the cohort was further grouped into quartiles of minutes from ICU admission to NE administration as well as quartiles of fluid volume per kilogram per hour. Mortality was calculated within each time and fluid quartile, shown in figure 6. Mortality tended to be lowest in the patients who received high volumes of fluids and NE earlier. Mortality appeared highest in those receiving lower volumes of fluids, but with later NE usage. This analysis also demonstrated that the lowest mortality overall occurred within the patients with the earliest NE use (<152 min), while the highest mortality occurred in patients with the latest NE use (701–1437 min).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mortality heat map based on quartiles of fluids received prior to vasopressors and quartiles of time from admission to vasopressor administration. NE, norepinephrine.
Discussion
The Surviving Sepsis Campaign guideline compilation produced by the Society of Critical Care Medicine aligns with the findings of this study, recommending the early use of vasoactive agents to support MAP without any specific time guidelines.13 However, in 2018, a new updated 1-hour bundle suggested starting vasopressors after initial fluid resuscitation if unresponsive to initial fluids.22 In particular, the use of NE as the first-line vasopressor is highly recommended, as well as the possible addition of other agents depending on the response and status of the patient in the most recent guidelines.13 Generally, there is some consensus among clinicians that earlier use of vasopressors, after initial fluid resuscitation or before completion of fluid resuscitation is optimal.23 This is likely due in part to the decreased risk of fluid overload and increased vascular permeability, which may decrease organ damage and the incidence of procedures such as thoracentesis, paracentesis and diuretic use which come with increased risk to the patient.24 25 There is limited evidence to support the ideal window for initiating vasopressor administration in the setting of septic shock, thus the decision to begin using NE is mostly guided by a high clinical suspicion for further deterioration despite aggressive fluid resuscitation, signs and symptoms of tissue malperfusion and thorough consideration of any coexisting risk factors or comorbidities. Given this, it is difficult to establish clear factors to determine the optimal time for initiation of NE or vasopressor support.
Guidelines do not specify the timing and volume of fluid resuscitation and initiation of vasopressor use. To our knowledge, only one study has investigated the interaction between fluids received and vasoactive agent use. This study suggested that at least 1 L of fluids prior to vasopressor use was associated with lower mortality.26 Additionally, studies have also suggested that negative fluid balance is associated with decreased mortality.27 28 Sepsis is not primarily a volume depleted state and thus many patients with sepsis are not responsive to fluids.2 29 Many patients are however volume resuscitated without assessment of responsiveness which can lead to delay in the administration of vasopressors needed to increase MAP.
In our analysis, we found that patients receiving early NE had significantly lower mortality and ICU length of stay than those who received late NE but the need for mechanical ventilation was higher. This result aligns with several other smaller studies and trials which show that early NE improves overall outcomes.15 30–32 Importantly, the mortality benefit was controlling for several important factors which differed between groups. Multiple risk stratification scores including SOFA score, APSiii, SAPSii and OASIS were significantly higher in the late NE group and thus were included in our final model. Additionally, we saw that significantly fewer patients in the early NE group (52.9% vs 77.3%) had invasive intravenous lines placed prior to NE being administered and significantly fewer patients in the early group were mechanically ventilated prior to NE (51.7% vs 60.4% p<0.001). We found that in univariate analysis, lower mortality was observed in patients receiving early versus late NE via a central line while there was a lower mortality without quite reaching significance in patients receiving early versus late NE via a peripheral line (14.4% vs 19.6% p=0.078). This factor was included in our multivariate model, and suggests that the potential mortality benefit remains after controlling for peripheral versus central line administration of NE. This result aligns with current recommendations that peripheral vasopressor usage is appropriate in the correct clinical setting in order to prevent delay of vasopressor administration. In the analysis of mechanical ventilation, we excluded patients who were already ventilated by the time NE was started. In the late NE group, 625 patients (60.4%) were already intubated, while in the early NE group, 540 patients (51.7%) were intubated. Among all patients irrespective of NE timing, 685 in the early NE group (65.56%) and 713 in the late NE group (68.96%) were intubated. Although more patients in the late group were intubated overall, the fact that they had more time from admission to NE administration likely played a role in their requirement for intubation. Overall, it appears that the increased time between admission and delay in NE use increased the window for patients to require ventilatory support.
Culture data suggested that the highest proportions of positive cultures were from blood, sputum and urine cultures. This could suggest that the most common etiologies of sepsis in this cohort were bacteremia, pneumonia and urinary tract infections. There were more positive blood cultures in the early NE group and fewer positive urine cultures when compared with late NE group suggesting a higher proportion of bacteremic patients compared with patients with urosepsis. As blood cultures are in the initial sepsis bundles and urine cultures are not, this could explain in part why patients got earlier NE treatment, however this is very limited in that we only were able to obtain positive culture results in 779 patients of our total cohort. This information thus was not included in our final model, however we support further investigation into this explanation.
Literature has previously suggested that there may be an optimal fluid volume of resuscitation prior to using vasoactive agents.26 Our study suggests the opposite, that receiving vasoactive agents such as NE earlier in their ICU stay regardless of the amount of fluids received has a positive impact on mortality. Overall, we saw no statistically significant differences in these subgroups which could point to mediation of our observed decrease in mortality with early NE use based on the quantity of fluids received. We did observe a non-significant increase in mortality among patients with fluid use of 2.334–5.075 mL/kg/hour, however this trend did not remain in those receiving >5.075 mL/kg/hour. The odds of requiring mechanical ventilation after NE was increased in some cases, likely due to the timeframe where intubation could be required was ≤6 hours in the early group and up to 24 hours in the late NE group, therefore more of the late NE patients were excluded as more already were mechanically ventilated. This may suggest that NE timing does not have a significant effect on mechanical ventilation needs, which may be more of a function of the source of sepsis and pre-existing pulmonary pathologies. The difficulty in assessing this variable given that timeframes in which mechanical ventilation could be required is significantly different between groups indicating that more research focused on this primary outcome would likely be needed in a prospective design. No notable trends were demonstrated in length of stay based on fluid quartiles that differed from our main results. In sum, it did not appear that fluids received had significant effects on our main outcomes, and that the early use of NE had a greater impact on mortality in patients meeting sepsis-3 criteria and did not appear to be mediated in large part by fluid quantity.
We further investigated the interaction between fluid volume received and time to NE use on mortality in a more granular way. This revealed that in general, lower times to NE use were associated with lower mortality, regardless of fluid amount received. In figure 6, the bottom right quadrant shows patients with higher fluid use as well as lower time to NE resulting in lower mortality than those in the top left quadrant, who were given lower volumes of fluid use and higher time to NE. When comparing the bottom left quadrant where patients received lower fluid volumes and had less time before NE to the top right quadrant where patients received higher fluid volumes and had more time before NE, it appeared that NE timing may have a more significant impact on mortality than fluids. Current fluid resuscitation guidelines recommend 30 cc/kg as an initial fluid bolus. Using these data, we can infer that patients in certain quadrants received <30 cc/kg or >30 cc/kg as an initial fluid bolus, but cannot make a direct comparison as many patients had multiple boluses given over different time periods. Therefore, a possible strategy may be using NE very early (quartile 1) irrespective of fluid use, but giving adequate amounts of fluids may become more beneficial to outcomes when vasopressors are administered late. It is important to note that this analysis was not controlling for other covariates, and does not consider time over which boluses were administered, nor the number of total boluses received.
The determination of adequate response and achievement of fluid resuscitation is another component of sepsis management that requires the insight and clinical supervision of a physician. This distinction is not made lightly and depends on thorough review of patients’ vitals, labs, physical exam with an emphasis on volume status and thoughtful consideration of coexisting conditions and comorbidities. Future studies may be aimed at determining the most important indicators of adequate fluid resuscitation with respect to patients with sepsis and the etiology of their source of sepsis, however this particular topic was outside of the scope of this study.
We note several important limitations to this study. The retrospective nature of the study, which prevents inferences of causality and the single center data source limits generalizability. This database may also contain incomplete or inaccurate information secondary to inaccurate charting of real-time events. This required us to exclude patients from the analysis where we lacked information on fluid boluses or vasopressor use which may impact the generalizability or accuracy of our results. We were not able to obtain sufficient information regarding culture data, or source control to make conclusions or to control for sepsis sources in our cohorts. Lastly, we did not have access to cause of death information and thus were limited to all cause in-hospital 28-day mortality as our primary outcome of interest. Despite these limitations, this well-known clinical database provides a large sample size and numerous comorbidity variables, as well as risk stratification scores which allow for increased control of potential confounding factors. We believe this strengthens our interpretation of these observed associations.
Future research on this topic could clarify several aspects which we did not address. Although fluid volume per kilogram per hour seemed a reasonable way to quantify fluids in patients of differing weights and who were admitted for different periods of time, it is an imperfect measure given that resuscitation fluid boluses are often given at irregular intervals in response to blood pressure. Furthermore, we do not know of the initial fluid status of patients in this study. We suggest that measures such as ultrasound assessment of fluid responsiveness or even central venous pressure should be used in future research.33 Randomized clinical trials with differing fluid guidelines are likely needed, however care must be taken to ensure patient safety in the design as serious consequences could result from high or low deviations from typical fluid use.
Conclusion
Our research adds to the building evidence in favor of early use of vasoactive compounds (primarily NE) in severe sepsis and septic shock. We cannot conclude causation of the lowered mortality, nor the optimal timing of vasoactive agent usage. In this cohort however, lower 28-day mortality was associated with NE use within 6 hours of ICU admission for sepsis and septic shock as defined by sepsis-3 criteria, as well as a >2-point increase in SOFA score. We further found that early NE use was associated with decreased mortality compared with later NE and that this effect did not appear to be mediated by volume of fluids received. Although on univariate subgroup analysis, patients receiving early NE via central line reached statistical significance and patients with peripheral administration did not, in both cases mortality was lower in the early NE group, and this factor was controlled for in our multivariate model. We suggest that the association between early NE use and mortality remains in spite of the route of administration of NE, in line with current recommendations. NE administration did not appear associated with ICU or hospital length of stay in our multivariate model, while the patients in the early group had higher rates of mechanical ventilation after NE use, which may be attributed to the fact that far fewer patients were mechanically ventilated prior to NE use compared with the late group. We support additional research to elucidate the optimal balance between fluids and vasopressors in sepsis.
Data availability statement
Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TRF, FZM and CH contributed equally to this paper. TRF: conceptualization and study design, data access, data analysis, data interpretation, manuscript writing and submission. FZM: conceptualization and study design, data interpretation, manuscript writing and submission. CH: conceptualization and study design, data interpretation, manuscript writing. HA: figures and tables. MR: conceptualization, study design, data access and supervision. FS: the guarantor of the paper, responsible for the conceptualization, data interpretation, manuscript writing, and oversight of the project as supervising author.
Funding Funding for open access publication was provided by the University of Nevada, Reno School of Medicine Open Access Fund
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.