Article Text

Abstract
Background Trauma patients frequently come into contact with law enforcement officers (LEOs) during the course of their medical care, but little is known about how LEO presence affects processes of care. We surveyed members of the American Association for the Surgery of Trauma (AAST) to assess their perspectives on frequency, circumstances, and implications of LEO presence in trauma bays nationwide.
Methods Survey items addressed respondents’ experience with the frequency and context of LEO presence and their perspectives on the impact of LEO presence for patients, clinical care, and public safety. Respondent demographics, professional characteristics, and practice setting were collected. The survey was distributed electronically to AAST members in September and October of 2020. Responses were compared by participant age, gender, race, ethnicity, urban versus rural location using χ2 tests.
Results Of 234 respondents, 189 (80.7%) were attending surgeons, 169 (72.2%) identified as white, and 144 (61.5%) as male. 187 respondents (79.9%) observed LEO presence at least weekly. Respondents found LEO presence was most helpful for public safety, followed by clinical care, and then for patients. Older respondents rated LEO presence as helpful more often than younger respondents regarding the impact on patients, clinical care, and public safety (p<0.001 across all domains). When determining LEO access, respondents assessed severity of the patient’s condition, the safety of emergency department staff, the safety of LEOs, and a patient’s potential role as a threat to public safety.
Conclusions Respondents described a wide range of perspectives on the impact and consequence of LEO in the trauma bay, with little policy to guide interactions. The overlap of law enforcement and healthcare in the trauma bay deserves attention from institutional and professional policymakers to preserve patient safety and autonomy and patient-centered care.
Level of evidence IV, survey study.
- resuscitation
- policy
- Surveys And Questionnaires
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Law enforcement presence is common in the trauma bay, and little policy exists to guide clinicians and officers in this context.
WHAT THIS STUDY ADDS
American Association for the Surgery of Trauma members commonly encounter law enforcement officers (LEOs) in the trauma bay, and their perspectives on the impact of LEO presence varied widely, with older and male respondents having more authority over LEOs and finding their presence more helpful.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The overlap of law enforcement and healthcare in the trauma bay deserves attention from institutional and professional policymakers to preserve patient safety and autonomy and patient-centered care.
Background
Trauma patients frequently come into contact with law enforcement officers (LEOs) during the course of their medical care for several reasons.1 LEOs may transport or accompany injured patients who are in police custody or incarcerated to the hospital. LEOs also provide direct transport to trauma centers in municipalities where ‘scoop and run’ is an authorized prehospital management strategy for penetrating injuries.1 LEOs enter hospitals to investigate potential crimes that led to trauma, such as violence or intoxicated driving. LEOs are also called to the hospital to address security concerns for patients and/or staff. The incidence of LEO presence and interactions in trauma resuscitation bays is not well established, but a recent observational study found that LEOs interacted with 40% of trauma patients at a level I trauma center in Philadelphia.2 In this study, our objective was to evaluate trauma surgeons’ experiences of and perspectives on LEO presence in trauma bays.
It is imperative to understand LEO presence in the trauma bay, as the intersection between criminal legal systems and the healthcare sector has the potential to impede equitable care.3 4 A recent publication developed by the American Association for the Surgery of Trauma (AAST) committee on injury prevention lays out ethical considerations for these interactions, calling for hospitals to work with community and law enforcement to develop just, transparent guidance that safeguards patient autonomy.5 In another recent study, emergency medicine physicians reported concerns about privacy violations when the police were present in emergency care settings. They expressed particular concern for intentionally or inadvertently granting police access to patients’ belongings and their protected health information in violation of the Health Insurance Portability and Accountability Act privacy rule (HIPAA).6 Beyond HIPAA, patients have the constitutionally protected right to consent to police questioning, but medical vulnerability, limited mobility, and impaired decision-making may keep them from advocating for themselves effectively.7
LEO presence may be helpful to address public safety concerns and to support patients who seek LEO assistance or protection during hospitalization. For other patients, particularly those who have had prior negative experiences with LEOs, avoiding LEO interaction may be preferred.8–11 Exposing injured patients to LEO contact without their explicit consent may erode patient autonomy, trust in the healthcare team, and can worsen patients’ experience of care. LEO presence may also impede care if it discourages patients from sharing clinically relevant, legally risky information with clinicians (eg, drug use or injury circumstance).6 8 9
Minimal legal, ethical, professional, or institutional guidance applies to the complex interplay between law enforcement and clinical trauma care.7 In the absence of clear policy, ad hoc decision-making at the bedside may be the default, but may not optimally serve patients’ medical, ethical and legal needs.12 Little is known about the frequency or circumstance of LEO presence in the trauma bay or about how physician characteristics and experience may influence their perceptions of LEO activity during clinical care. We therefore conducted a survey of trauma surgeons recruited from the membership of the AAST to evaluate respondents’ perception on law enforcement presence in the trauma bay.
Methods
Data collection
This was a cross-sectional, descriptive, survey study. Items included in the survey instrument were developed collaboratively by the research team and piloted internally to assess clarity and content validity. Survey items included the frequency and context of LEO presence and perspectives on the impact of LEO presence on public safety, clinical care, and patients. Respondent demographics, professional stage, and practice setting were solicited. Prior to deployment, the survey was approved by the AAST Secretary-Treasurer. The survey was distributed by email to all AAST members in September and then again in October 2020. Responses were collected electronically using Qualtrics. The survey instrument is included as online supplemental digital content. Respondents provided informed consent to initiate survey data collection and no individually identifying information was collected as part of the survey. Participants were able to skip questions at will. As an incentive, survey respondents were entered into a lottery and one respondent received an Apple watch. To be entered into the lottery, recipients entered contact information into a separate form that was not connected to their survey responses. This study was reported using the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Supplemental material
Analysis
All quantitative data were tabulated descriptively. Responses were compared by participant age, gender, race, ethnicity, urban versus rural location using χ2 tests. Pearson’s correlation coefficients, which enumerate the linear correlation (from −1 to 1) between two normally distributed quantitative variables, were used to compare the association of responses across domains with the goal of understanding how responses to one question might relate to responses to another. The Consensus-Based Checklist for Reporting of Survey Studies guideline was used to ensure proper reporting of methods, results, and discussion (SDC 1).13 Analysis was conducted using Stata (V.15, StataCorp, College Station, Texas, USA).
Open-ended questions posed at the end of the survey were analyzed using content analysis.14 15 Two independent members of the research team open-coded these data to create an initial coding schema describing the aggregate content of participants’ responses. This coding schema was described in a codebook through comparative and consensus building. A third member of the research team independently used the codebook to verify a final coding schema. The research team then identified overarching categories that summarized codes from all open-ended responses.
Results
Respondents
We received responses from 234 AAST members (14.5% of 1612 who were emailed a survey) who worked in clinical roles in 43 US states, Washington, DC, and Canada. The majority were attending surgeons (189, 80.7%). Of the cohort, 169 (72.2%) identified as white or European American and 144 (61.5%) as male. Respondents had extensive clinical experience: more than half had been in their current role for at least 15 years. Full respondent characteristics are in table 1.
Respondent characteristics
Incidence of LEO presence
One hundred eighty-seven respondents (79.9%) observed LEO presence at least weekly, including 51 (21.8%) who observe LEOs in trauma resuscitation areas on a daily basis. Only one respondent reported that they never observe LEOs. Respondents had observed LEOs in a range of context. A total of 87.6% had encountered LEOs accompanying patients who were under arrest or incarcerated, 83.3% questioning patients as witnesses to a crime and 76.9% questioning patients as suspects. A total of 81.6% observed LEOs accompanying a patient from jail or prison, and 74.4% had observed LEOs collecting evidence from patients. A total of 5.6% had encountered LEOs bringing a suspect to the hospital for identification by a patient. Other activities included providing security, securing the body of a deceased patient, or responding to a call from hospital staff. Other activities identified by respondents provide insight into context-specific LEO activities. Respondents observed LEOs investigating accidents, being on hand to ‘lock down the facility’, collecting information from victims or potential victims of crime, or collaborating with social services when a child is injured. LEOs were also observed when they themselves were injured or accompanying another injured officer. Two respondents mentioned officers seeking blood samples from patients who were suspected to be intoxicated.
Perspectives on law enforcement presence
Two hundred eighteen respondents (93%) provided input on how helpful or harmful they found law enforcement presence in the trauma bay for the public, for healthcare providers and the course of clinical care, and for patients. Respondents judged that LEO presence was most helpful for public safety, with 94 (43.1%) rating it very helpful or helpful, and 11 (5.0%) finding it harmful or very harmful in this domain. In clinical care, 65 (29.8%) found LEO presence helpful or very helpful, and 22 (10.1%) found it harmful or very harmful. For patients, 57 (26.1%) found LEO presence helpful or very helpful, and 29 (13.3%) found it harmful or very harmful. Complete responses are shown in figure 1.
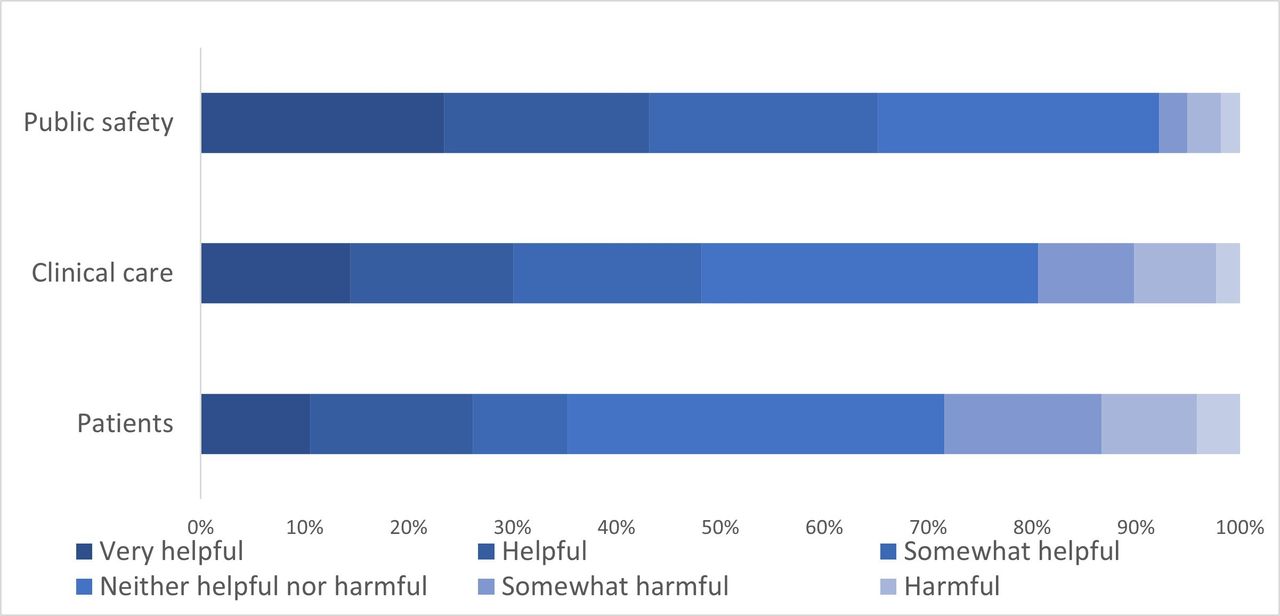
Impact of law enforcement presence on patients, clinical care, and public safety.
Responses were generally correlated across domains. There was a correlation of 0.68 between the domains of clinical care and patients, 0.69 between clinical care and public safety, and 0.54 between patient care and public safety (p<0.05 for all). No respondent who found LEO presence helpful for patients found it harmful for public safety, whereas 22 who found it helpful for public safety found it harmful for patients.
One hundred seventy-five respondents (74.7%) provided a brief open-ended description of the ways in which they perceive the impact of LEOs on patient care in the trauma bay. Responses fell into three overarching categories describing negative effects, positive effects or no/minimal effects.
Respondents who perceived that LEO presence had a negative effect on patients described several aspects (subcategories) of negative impact. These respondents described: interruptions to clinical care including difficulties that emerge when patients are handcuffed or shackled; potential violations of patient privacy when LEOs are within earshot of clinical procedures and conversations; and most commonly, added emotional distress and agitation in patients. Respondents whose responses fell in this category noted that LEO presence ‘brings unnecessary tension’ by ‘intimidating’ patients or causing ‘anxiety/agitation’, or even just in ‘distracting the patient while you’re trying to obtain a history’. One respondent described LEO presence as ‘…the antithesis to Trauma Informed or Patient Centered Care. Patients, who are mostly African American in my center do not feel safe or comforted by the presence of police in the bay.’ Other respondents noted that LEOs ‘do not understand the acuity in patient injury’ leading them to ‘obstruct clinical care’ including when patients are critically ill or have impaired consciousness. Another respondents described the concern that LEO involvement ‘degrades the credibility of the trauma team’ and ‘engenders unconscious and conscious bias in providers, potentially labeling patients as criminals or ‘bad’.’
Respondents who described the effect of LEOs on patient care positively described: the added safety and security that LEOs provide; a context of mutual respect and collaboration; and the ways in which LEOs are helpful for gathering pertinent patient information and contacting family and next of kin. In providing security, one respondent described that ‘Patient violence against hospital staff in our facility is an ever-present danger. Their (LEO) presence to bolster our own security has preserved worker safety on many occasions.’ Another respondent reported valuing ‘the job they [LEOs] need to do’, for example, in collecting fresh evidence from patients for illegal behaviors, such as in prosecuting intoxicated drivers. Several respondents noted that they thought that LEOs treated surgeons with deference and were ‘helpful’ and ‘respectful’. One wrote that the collaboration with law enforcement ‘makes the team members proud to serve the public along with the brave law enforcement officers’.
Associations of respondent characteristics with perspectives on law enforcement presence
The range of respondents’ ages is shown in table 1. In general, older respondents rated LEO presence as helpful more often than younger respondents regarding the impact on patients, clinical care, and public safety (as shown in figure 2, p<0.001 across all domains). The 59 women who responded to the survey rated LEO presence as harmful more often than the 144 men who responded (as shown in figure 3, p<0.01 across all domains). No comparisons could be made to include the one respondent who identified as another gender, and the 30 respondents who did not indicate a gender identity were excluded from this portion of the analysis. Twenty-nine respondents (12.4%) identified as black, Asian, Native American, and/or Latinx. There was no significant association found between respondent race or ethnicity and survey responses. There were no associations between respondents’ institutional affiliations at urban versus suburban versus rural trauma centers or workplaces and survey responses.

Respondent perspectives according to age.
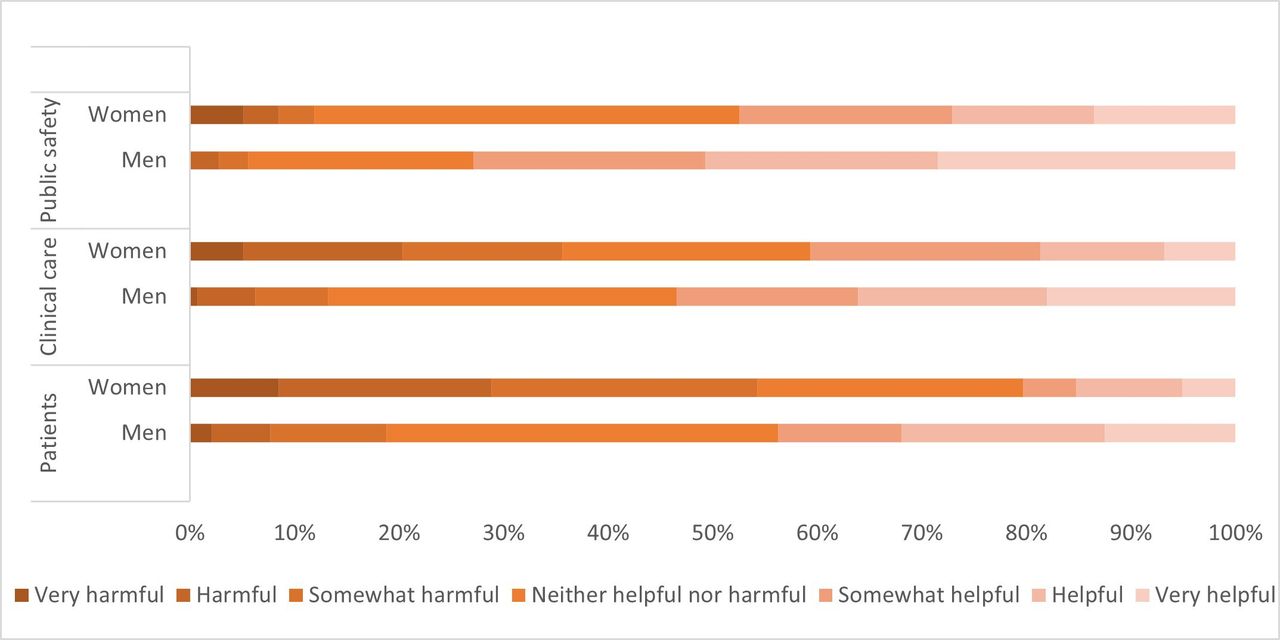
Respondent perspectives according to gender.
Determining LEO access to patients
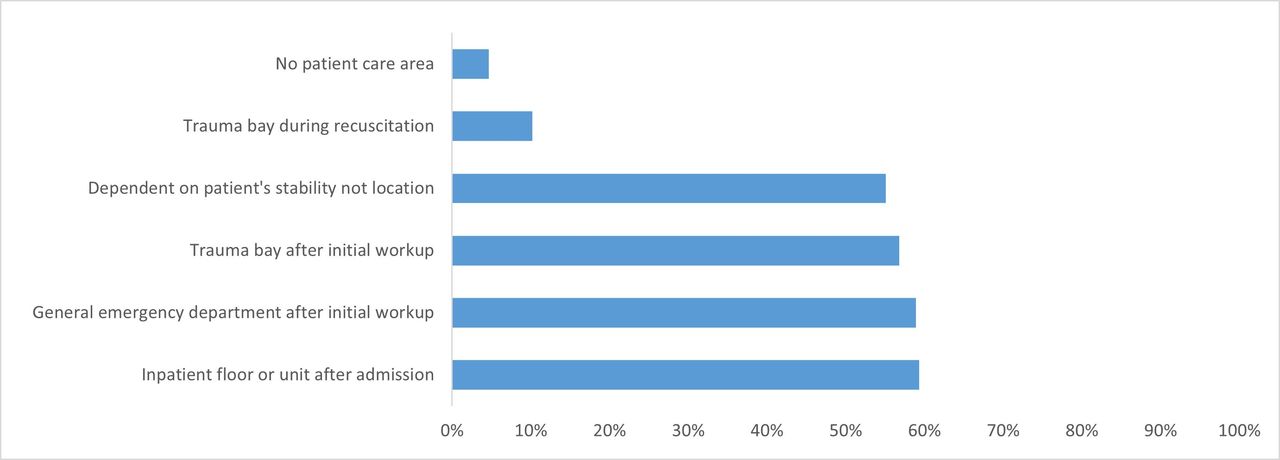
When determining whether to permit LEOs access to patients, the severity of the patient’s condition was most often endorsed very important, followed by the safety of emergency department staff, the safety of LEOs, and a patient’s potential as a threat to public safety. Patients’ preferences were least commonly considered very important. Figure 4 shows the relative importance of various factors that respondents considered in permitting LEO access to patients among 182 respondents who completed these questions. Figure 5 shows respondents’ preferences for when and where LEOs ideally should interact with patients.
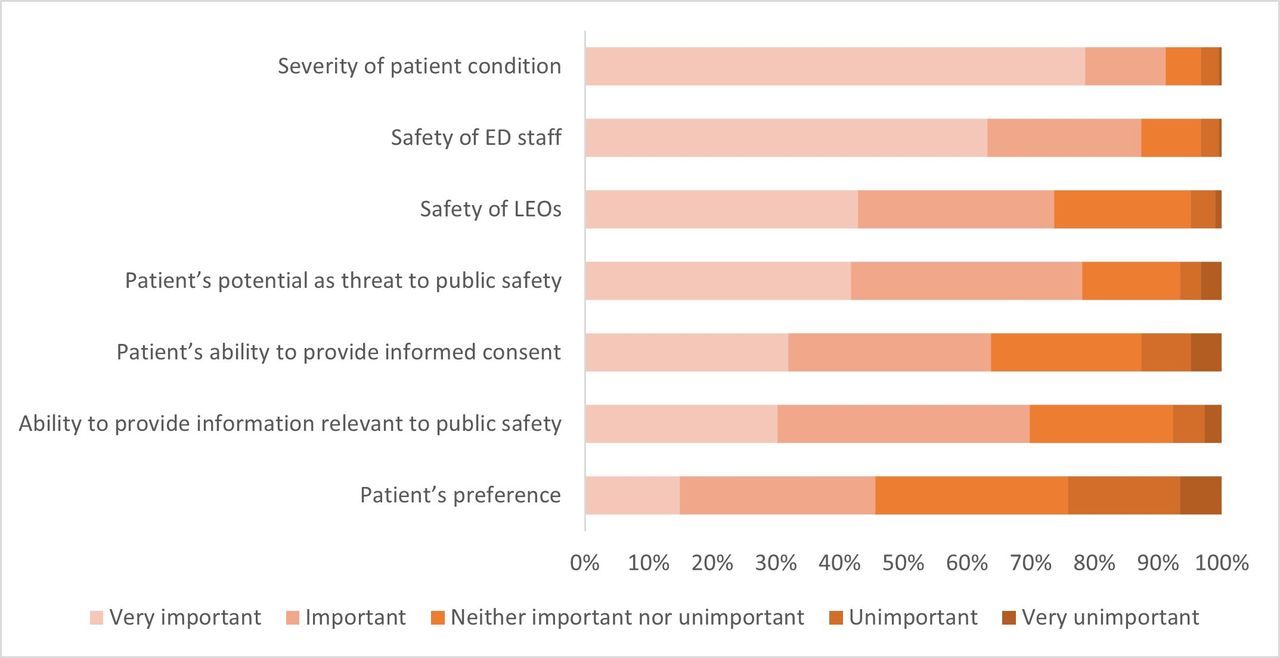
Factors respondents consider when deciding on LEO access to patients. ED, emergency department; LEO, law enforcement officer.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
When and where law enforcement officers should interact with patients.
One hundred seventy-three respondents (79.4%) thought that they had oversight or influence over LEO access to patients. Older (87.8% of those aged ≥45 years vs. 62.7% of those aged ≤44 years, p<0.001) and male (85.4% of men vs. 66.1% of women, p=0.008) respondents were more likely to report having oversight or influence. Respondents who reported having oversight over LEOs were more likely to find LEO presence helpful when compared with respondents who reported not having oversight (38.2% vs. 18.8%, p=0.01). Perceptions of oversight were also correlated with perceptions of the effect of LEO presence on patients.
Forty-four respondents (20.7%) reported that their institutions had a policy in place to guide police interactions with trauma patients, 44 (20.7%) reported no policy, and 125 (58.7%) did not know if a policy existed. One hundred fifty-six (72.9%) reported that there was a need for such policies or guidelines. Respondents provided few details on existing policy in a follow-up open-ended item. Several noted only that a policy existed or that their institution’s policy followed applicable laws such as requiring patient consent or a warrant for blood work. Some noted that policy allowed LEO access as long as it did not interfere with care, or at the discretion of the attending physician or trauma team. Others noted that hospital security or contracted police officers acted as an intermediary with outside, unaffiliated LEOs, but did not describe an explicit policy. Three respondents mentioned specific policies. Of these, two noted that the police are allowed in the emergency department, but not the trauma bay, and one reported that the police must check in with security and be escorted by them, and also described staff training on HIPAA, mandatory reporting, and applicable state law.
Discussion
Trauma surgeons provide oversight for the clinical care and well-being of patients in the trauma bay. In this survey of AAST members, respondents described a wide range of perspectives on the incidence and consequences of LEOs in the trauma bay, noting the rarity of guiding policy or standard procedure. The perception of LEO presence as helpful versus harmful demonstrated age and gender-based associations. Older and male participants were more likely to report that they had oversight over LEO access to patients and were more likely to rate LEO presence as helpful for public safety, for clinical care, and for patient well-being.
More respondents perceived LEO presence as helpful for public safety than for clinical care or patient well-being. This corresponds with the results of a recent survey of emergency medicine physicians, who prioritized staff and public safety most highly in navigating these interactions.16 This indicates then when clinicians think about LEO presence, they may be focused on issues outside of the core patient-centered mission of healthcare. Consistent with patient perspectives in previous research,8 9 11 many respondents found LEOs’ presence a detriment, by disrupting clinical care, causing emotional distress to patients, or leading patients to minimize symptoms or withhold medically pertinent information that could pose legal risks.
Though not explicitly explored in this current survey, the risks posed by law enforcement in the trauma bay cannot be considered independently of the consequences of structural and institutional racism in the USA. The same young men of color who are at highest risk of injury due to interpersonal violence are also at higher risk of previous adverse experiences with law enforcement,9 17 and of LEO contact during clinical care. These same patients, who may be stereotyped on the basis of their age, race and violent injury, also often have the least access economic and legal resources to support their rights and recovery. Implicit biases abound in clinical care, but can easily be amplified when clinicians are under high mental load as they care for critically injured patients.18 In particular, when clinicians implicitly or explicitly assume that their patients have committed a crime, they may treat them as less deserving of care and consideration.19 LEO presence can reinforce these assumptions.9 20 21 Likewise, local conditions including racial segregation may impact relationships between community and law enforcement and may have influenced survey responses in ways we cannot directly assess.
Clinicians and hospitals have the opportunity to advance patient-centered care by ensuring that law enforcement presence promotes patient safety, autonomy, and healing, or at least does not impede these goals. Nearly three in four respondents identified a need for policy to guide interactions with law enforcement. Only one in five were aware of any institutional policy relevant to the issue, and their policy descriptions indicate that clear guidance is rare. The American College of Emergency Physicians’ statement on the topic states that physicians should prioritize patient privacy, but allows latitude for physicians to use their judgment in sharing information with law enforcement.22 To our knowledge, other professional organizations responsible for the clinical care of injured patients have yet to issue such guidance, leaving LEOs and clinicians in the position of reinventing processes of care at the bedside. Professional organizations in trauma surgery have the opportunity to lead by establishing best practices for LEO presence during injury care.
With the legal background provided by Song,7 the Georgetown University Health Justice Alliance has laid out areas that such policies should address: visitor access; sharing information; LEO requests for procedures and tests; and use of handcuffs, shackles, and other restraints. This is essential, as patients’ medical condition may impair their capacity to consent to police questioning or involvement, including pain, pain education, head trauma, and more.7 These challenges can be addressed at least in part by making sure that LEOs are identified; avoiding providing consent on the patient’s behalf to information disclosure, search, seizure, and questioning; requiring formal processes, warrants, and court orders where protected health information is involved; and designating administrative routes for addressing LEO requests and concerns.23 The details of a guideline or policy will depend on individual healthcare institutions and systems as well as local and state law. Furthermore, the development of an institutional policy that is adopted widely requires input and buy-in from many stakeholders including nursing, physicians, security, legal affairs, and local law enforcement agencies. However, shared principles and best practices have the potential to advance patient rights, patient safety, and patient care across the nation.
Survey responses provide a good starting point for policy development. Respondents’ stated priority in allowing LEO access was patient condition and stability, in line with the paramount priority of healthcare institutions. When asked where LEOs should interact with patients, few clinicians thought that the trauma bay was an appropriate location, but many agreed that location was less important than stability. The second most highly ranked consideration was staff safety, followed by LEO safety, and the patient’s potential as a public safety threat. Patients have threatened or injured clinicians in the emergency department,24 and this is a major source of staff concern. Policies that guide LEO presence in the trauma care settings should exist within the context of evidence-based strategies to reduce emergency department workplace violence, such as ensuring adequate staffing and providing training in de-escalation techniques.25 Of course, patients who seek support from the police or who seek to work with the police to meet their goals or to address the circumstances of their injury should be supported to do so, in ways that do not impede their clinical care or their legal well-being.
This study is limited by its survey methodology. The response rate was low, and we cannot know how non-respondents may have differed. Non-respondents may have more insight or different perspectives on these issues, and may differ in terms of demographics and practice settings. Survey respondents were AAST members, and their perspective may not be representative of other trauma clinicians. Respondents commonly represented urban, level I centers, and other contexts might provide different perspectives. Policy development should take into account the perspectives of a broad range of stakeholders, outcomes, and local conditions, not simply those represented here. No specific actions were taken to prevent a respondent from answering the survey more than once, though given the limited distribution list, we expect this is unlikely. The impact of clinician race and ethnicity could not be clearly assessed given the large proportion of respondents who were non-Hispanic white. We cannot determine from this study how much of the variation in perceptions of the presence of LEOs in the trauma bay that we identified reflects straightforward differences of opinion and how much reflects differences in experience based on participant positionality.26 This is true for both quantitative and qualitative open-ended survey responses, the latter of which provides exemplars of the polarity (negative to positive) of perceptions and cannot be interpreted as representative of trauma surgeons across health systems, geographic location, and the larger social context in which they work. Moreover, we cannot determine the nature or effect of variation in LEO practices across the wide range of geography and jurisdictions represented here. The USA has more than 16 000 local law enforcement agencies. State and local policies regarding policing vary widely,27 and it is likely that this extends to the trauma bay. Lastly, these results reflect respondent perspectives, rather than actual measurements of the impact of law enforcement presence on patient care, experience, or outcomes.
Trauma surgeons lead the care of patients in the trauma bay and should supervise the ways in which they experience trauma resuscitation and emergency care. This purview should include the impact of law enforcement presence on patient care. Law enforcement presence is common in the trauma bay. Survey respondents provided a wide range of perspectives on the role of LEOs. Policy guidance to standardize LEO–patient–clinician contact is rare, and respondents expressed both an appetite for such guidance and some principles that can contribute to policy that safeguards the key features of patient-centered care.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
The Institutional Review Board of the University of Pennsylvania determined this study was exempt from the requirement for review, as it was an anonymous survey.
Acknowledgments
The authors are grateful for the support of the AAST in distributing this survey, and for the assistance of Nikita Patel and Emily Seeburger in preliminary data analysis.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors EK, UK, JB, and SFJ developed the concept and study design. EK, UK, SFJ, and RA analyzed the data. EK drafted the article. All authors contributed to critical review. EK accepts full responsibility for the conduct of the study, had access to the data, and controlled the decision to publish.
Funding There was no specific funding for this study. EK is supported by the Agency for Healthcare Research and Quality (K12-HS026372).
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.