Article Text

Statistics from Altmetric.com
Case summary
A 59-year old woman presented to the emergency department (ED) after sustaining injuries in a head-on motor vehicle collision. A supraglottic airway was placed in the field secondary to a depressed Glasgow Coma Scale score and airway protection. The patient initially presented to the ED with hemodynamic instability, as defined by tachycardia (153 beats/min) and hypotension (87/67 mm Hg). During the primary and secondary surveys, the supraglottic airway was exchanged for an endotracheal tube; a left-sided chest tube for large pneumothorax was placed; the pelvis was sheeted; and the patient received whole blood. Following these interventions, her heart rate was 87 beats/min with a blood pressure of 106/81 mm Hg. Focused assessment with sonography for trauma exam was positive for fluid in the right upper quadrant. Physical examination was significant for crepitus along the left chest wall, and venous oozing was identified from a vaginal laceration. Pelvic radiography showed multiple pelvic fractures.
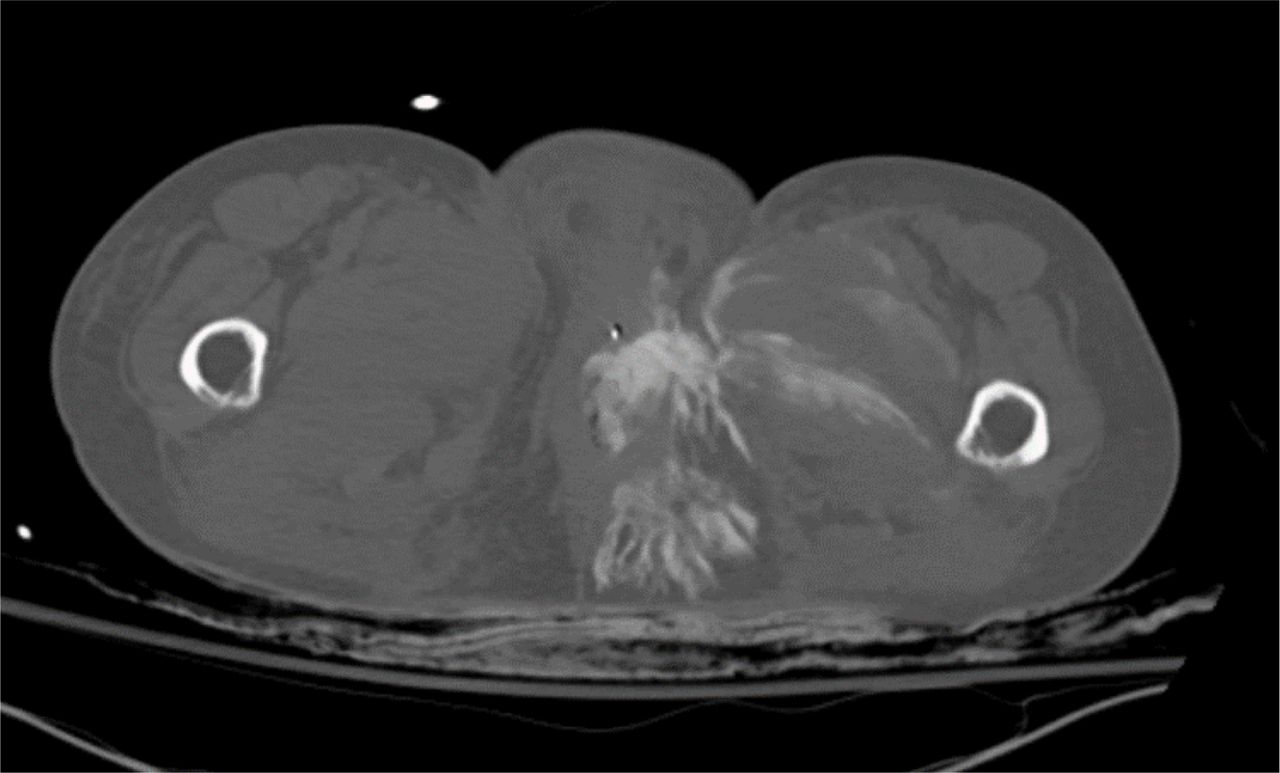
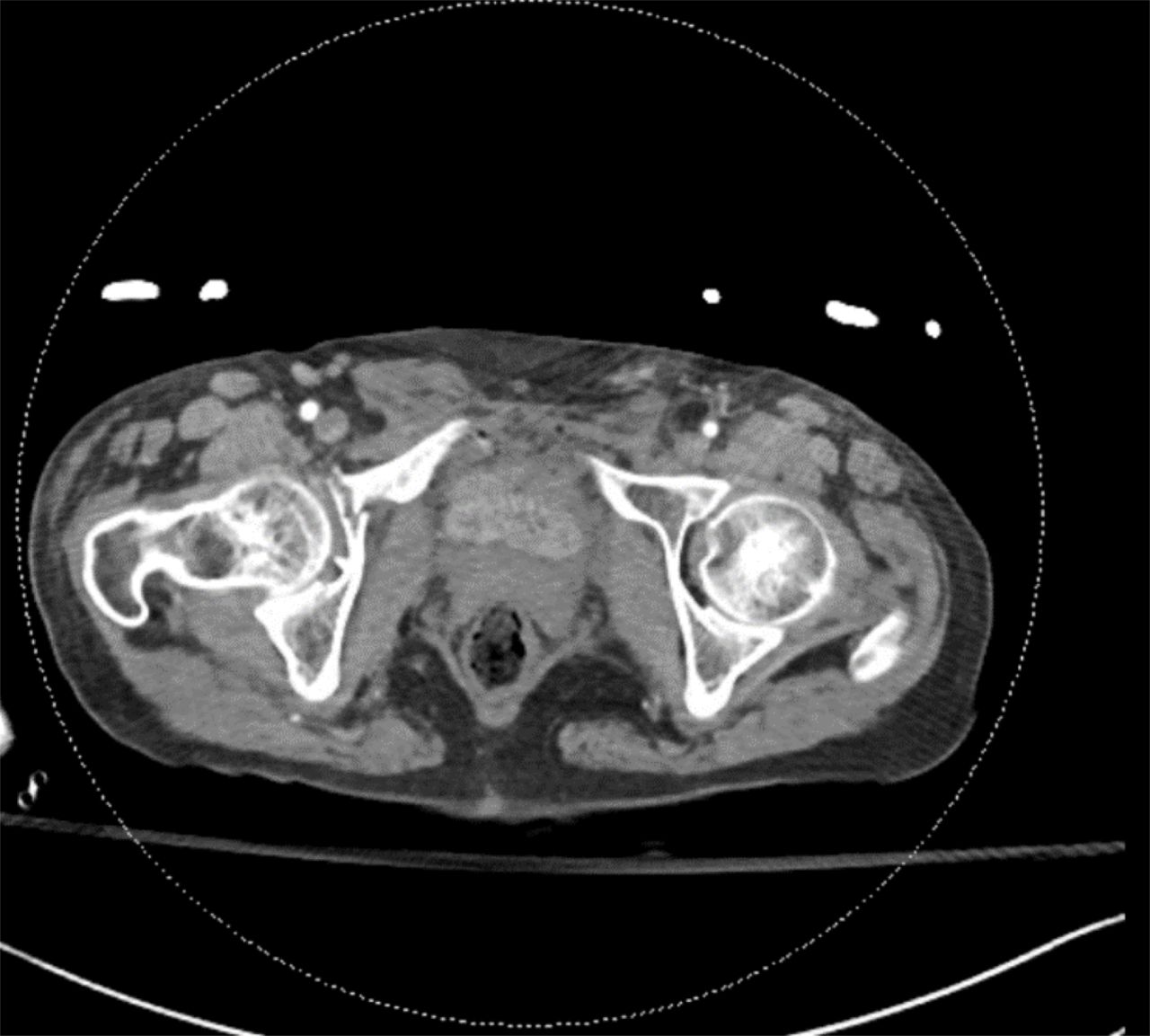
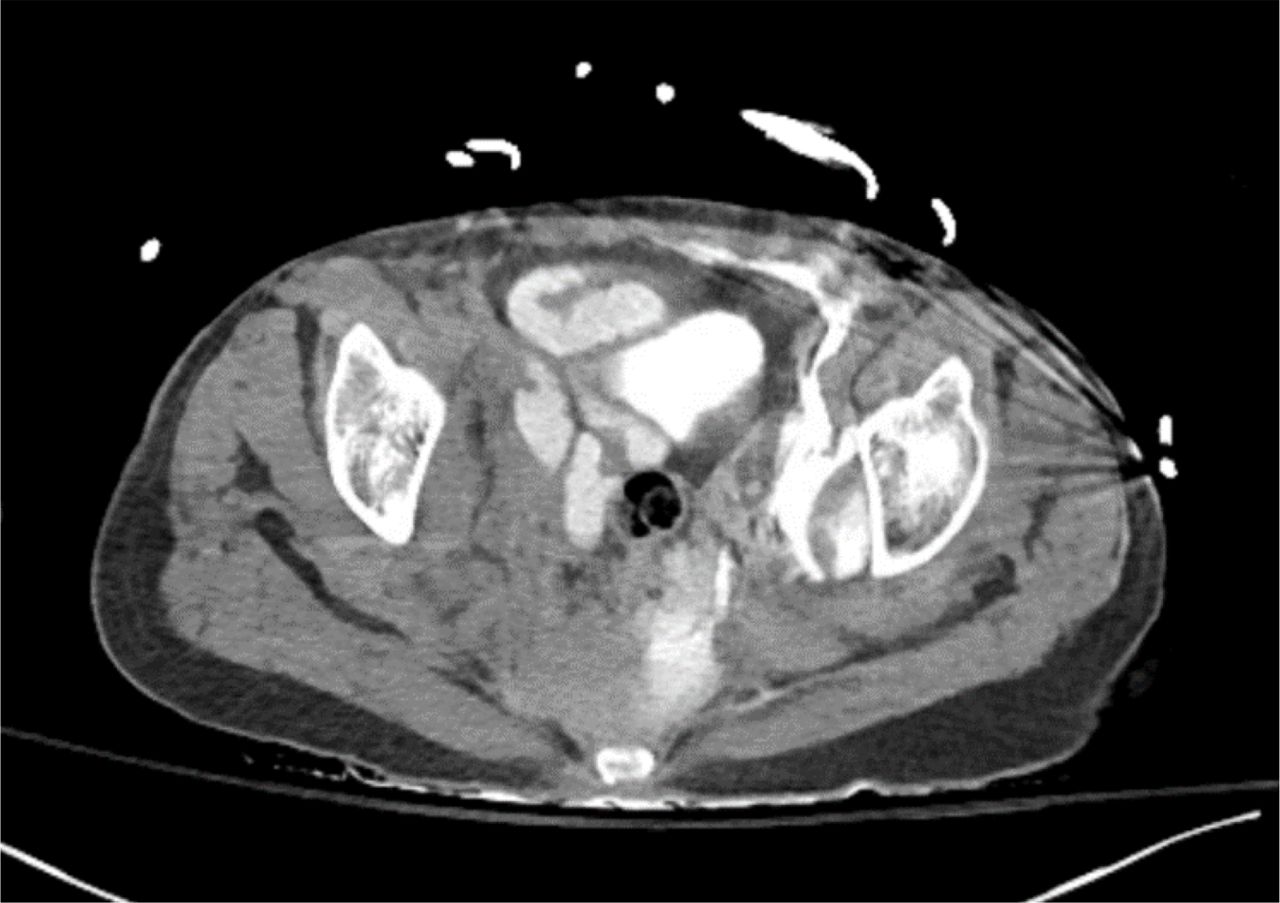
CT imaging was performed, which revealed multiple left-side rib fractures, small volume intraperitoneal fluid layering in right paracolic gutter and complex pelvic fractures with a decompressed bladder (figure 1). Given these constellation of findings, there was concern for a bladder injury and a CT cystogram was obtained. Prior to administration of contrast into the bladder, the non-infused CT scan revealed concern for a urethral and bladder base injury with extensive contrast in the extraperitoneal space (figure 2). The Foley catheter extended into the urethral defect, and there was contrast in the distal small bowel (figure 3).
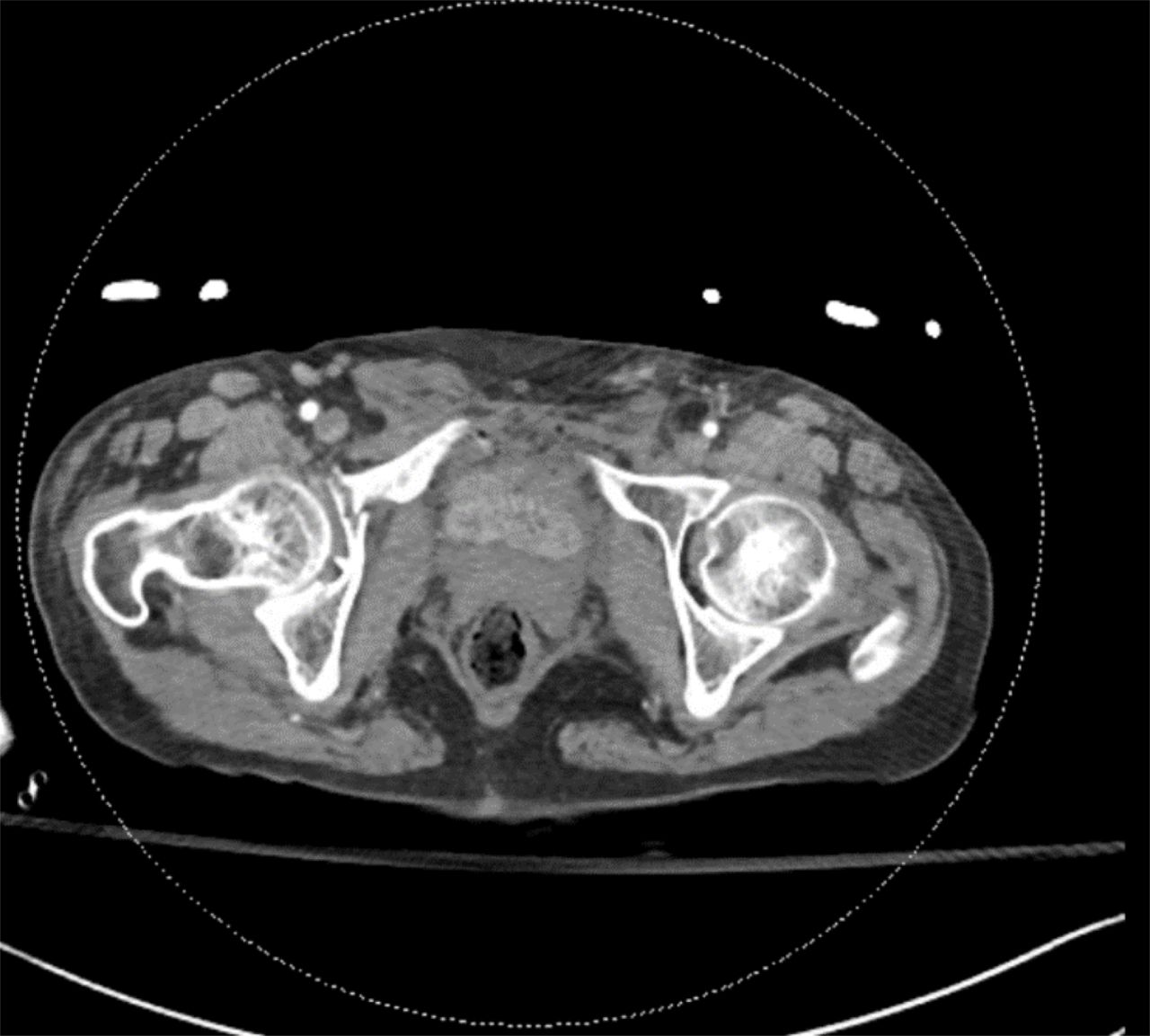
Initial pelvic CT scan demonstrating a decompressed bladder, pelvic fractures, and small dots of air in the extraperitoneal space anterior to the bladder.
Dry CT scan prior to instillation of bladder contrast for CT cystogram showing previously administered IV contrast pooling in the extraperitoneal space.

{kind=link}
{kind=link}
{kind=link}
Dry CT scan prior to instillation of bladder contrast for CT cystogram. Previously given IV contrast is seen in the bladder and distal small bowel.
What would you do next?
Proceed with CT cystogram.
Proceed to the operating room for abdominal exploration and concomitant genitourinary exploration.
Reattempt Foley catheter placement.
Placement of suprapubic tube and admission to the intensive care unit with delayed plans for genitourinary and orthopedic repair.
What we did and why
B. Proceed to the operating room for abdominal exploration and concomitant genitourinary exploration
Our decision to expeditiously explore the abdomen was made based primarily on the concern for a genitourinary–enteric fistula or small bowel injury. Given the presence of intraluminal contrast in the distal small bowel and intraperitoneal free fluid. Because of this, we elected to proceed with exploration of the abdomen with concomitant urinary tract repair. In this case, completion of a formal CT cystogram would not provide further actionable information. Similarly, a CT cystogram would have required replacement of the Foley catheter, which would necessitate operative attempts by urology, given the urethral/bladder neck injury seen on non-infused CT scan. Finally, while suprapubic tube placement would allow for bladder decompression, this approach would fail to address the concern for genitourinary–enteric fistula.
In the operating room, a flexible sigmoidoscopy was negative for rectal injury and the vaginal laceration was primarily repaired. We then attempted to perform diagnostic laparoscopy, but due to adhesive disease, the small bowel was not able to be adequately evaluated and required conversion to laparotomy to rule out a genitourinary–enteric fistula or small bowel injury. No injuries to the bowel were identified. With the assistance of the urological surgeons, an avulsed bladder neck and traumatic cystotomy were identified. The urethra was completely avulsed and could not be cannulated with a cystoscope. Ultimately, a successful approach required passage of a wire antegrade from inside the bladder, across the injury, and into the uretha. A 20 Fr catheter was inserted over the wire with subsequent urethral repair. The traumatic cystotomy was repaired primarily. Due to pelvic coagulopathic bleeding and acidosis, the patient’s pelvis was packed and temporarily closed. She was taken to the ICU to complete her resuscitation. She returned to the OR the next day after normalization of her physiology for washout and abdominal closure.
The primary challenge in this case was diagnostic, pertinent to the possibility of bowel injury or genitourinary-enteric fistula. In the absence of these clinical findings at the time of operation, the identification of enteric contrast exemplifies a rare case of vicarious elimination of intravenous contrast. Less than 1% of intravenously administered contrast is excreted through vicarious pathways and most commonly excreted through the gallbladder. Though this was a consideration of ours, the constellation of findings revealing intraluminal contrast, pelvic free fluid, and close proximity of contrast containing small bowel to the injured bladder necessitated prompt abdominal exploration for potential bowel injury and/or genitourinary-enteric fistula.
The patient ultimately underwent repair of her pelvic fractures 2 days after initial presentation. Postoperatively, the patient’s course was complicated by a urinary anastomotic leak, requiring placement of nephrostomy tubes. However, she otherwise recovered well and was discharged on hospital day 26.
Ethics statements
Patient consent for publication
Footnotes
Contributors GRS, AH, JH, and SPC participated in the care of the patient and wrote and critically revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.