Article Text

Statistics from Altmetric.com
Case presentation
A female patient in her 80s presented to the emergency department with 1-day history of severe abdominal pain associated with nausea and vomiting. Her medical history was notable for hypertension, insulin-dependent type II diabetes mellitus, end-stage renal disease secondary to polycystic kidney disease (hemodialysis-dependent) and coronary artery disease with distant history of two drug-eluting stents (on daily clopidogrel). Prior surgical history included appendectomy and bladder suspension.
On arrival, the patient was hemodynamically stable and her abdomen was distended, but soft and non-tender. Laboratory assessment was notable for leukocytosis (19.3 K/µL), elevated lactate (3.31 mmol/L), baseline renal impairment (creatinine 3.33 mg/dL), and hyperglycemia (240 mg/dL).
CT angiography of the abdomen and pelvis showed a strangulated, poorly enhancing bowel loop interposed between the right obturator internus and pectineus muscles with severe dilation of proximal bowel loops (figure 1).
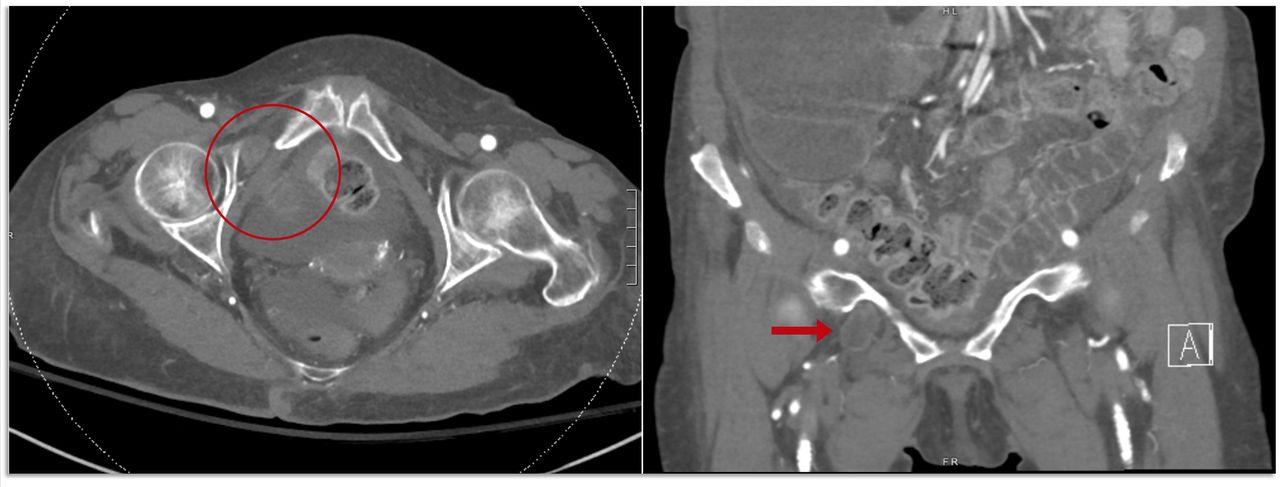
CT angiogram showing a right-sided obturator hernia in axial (red circle, left) and coronal (red arrow, right) views.
What would you do?
Attempt manual reduction with adduction and internal rotation of the thigh.
Laparoscopic hernia repair.
Open hernia repair via low midline laparotomy.
Open hernia repair via right inguinal incision.
What we did and why
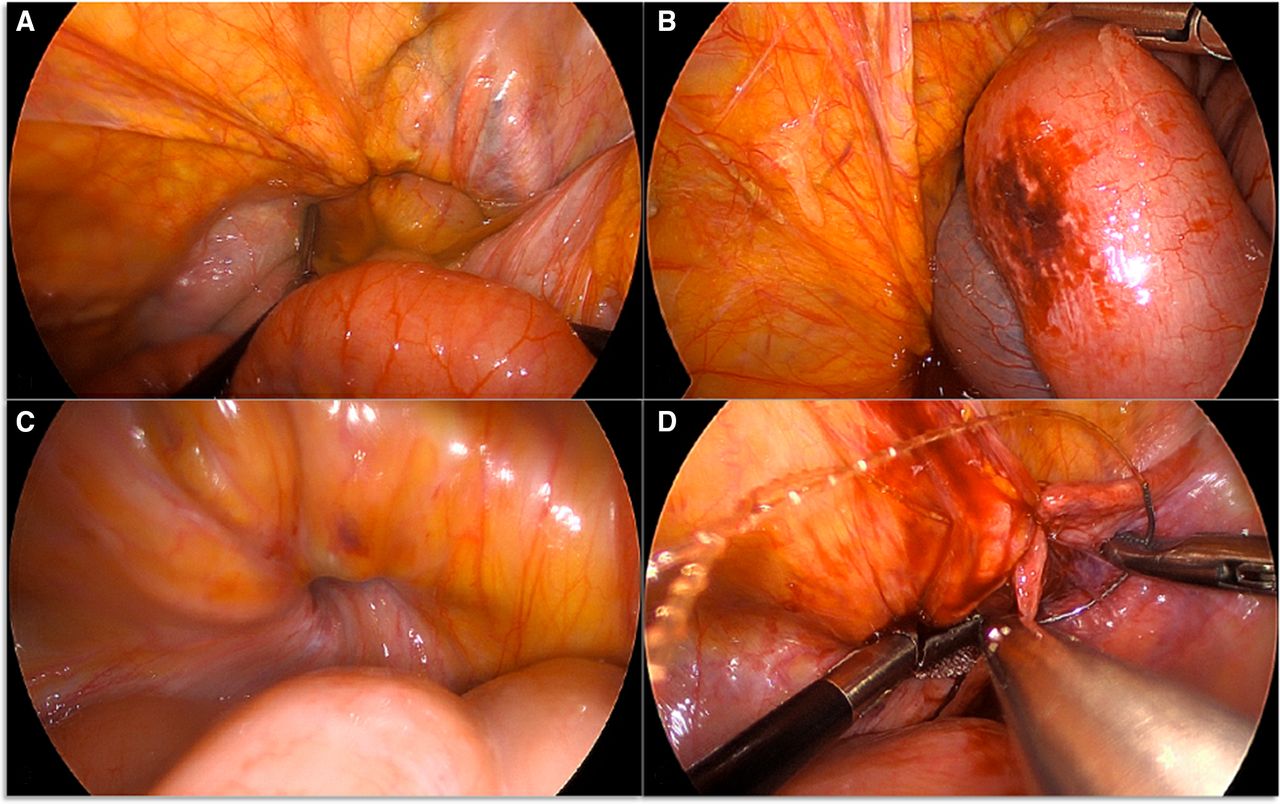
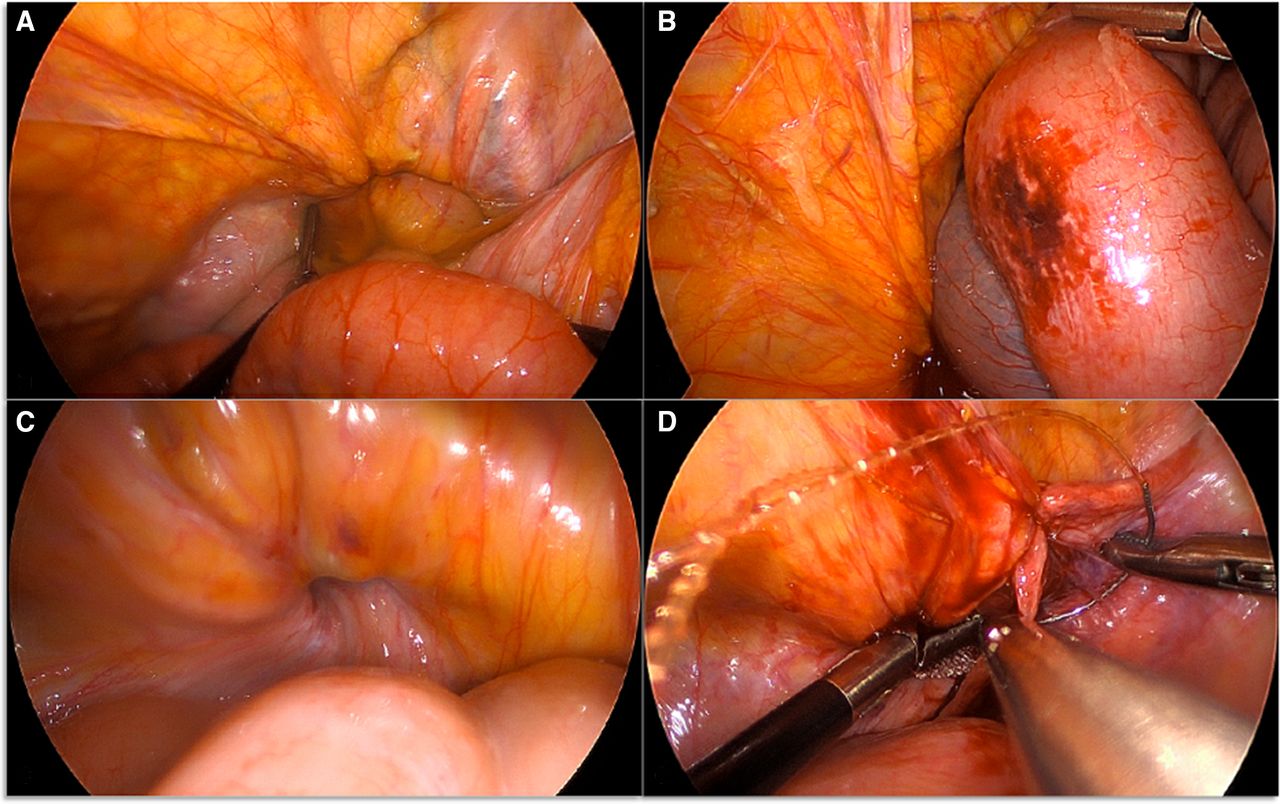
Our patient’s presentation was consistent with an incarcerated obturator hernia causing small bowel obstruction. After nasogastric tube decompression, we proceeded to the operating room for emergency laparoscopic obturator hernia reduction and repair (online supplemental video). On entry, we observed a loop of small bowel protruding through the obturator foramen, which we reduced with gentle traction. This bowel segment had a small ecchymotic area but did not appear ischemic or have serosal tears (figure 2A,B). We occluded the hernia defect with a prolene mesh plug and the overlying peritoneum was closed with a running v-lock suture (figure 2C,D). We placed a plug mesh to minimize operative time and mitigate potential bleeding associated with extensive dissection. The patient tolerated a diet by postoperative day 2.
Supplementary video
{kind=link}
{kind=link}
(A) Small bowel herniating through the right obturator foramen. (B) Bowel segment that was incarcerated through the obturator foramen, after reduction. (C) Obturator foramen defect post hernia reduction. (D) Peritoneal closure over obturator foramen plugged with mesh.
Obturator hernia occurs when abdominopelvic contents enter the obturator canal, an osteofibrous passage within the obturator foramen (bordered by the ischiopubic rami at the anteroinferior pelvic margin).1 Howship-Romberg sign—pain on ipsilateral thigh adduction and internal rotation due to obturator nerve compression—is only present in half of cases.2 Most obturator hernias present with bowel obstruction and require emergency operative management; almost half require resection of strangulated bowel.3 Obturator hernias account for only 0.2%–1.6%4 5 of mechanical bowel obstructions but are associated with high mortality (12%) due to delayed diagnosis.3 Contralateral obturator hernias (25%) and concomitant groin hernias (inguinal 19%, femoral 11%) are not infrequent.6 Abdominal CT is the diagnostic gold standard.3
Open primary repair through a midline laparotomy facilitates rapid exposure and is useful in cases of suspected perforation.6 7 However, laparoscopic repair should be considered in hemodynamically stable patients without suspected perforation. A recent meta-analysis (74 studies, 146 patients) found that compared with laparotomy, laparoscopic repair is associated with lower morbidity (OR 0.29, 95% CI 0.09 to 0.78) and mortality (OR 0.84, 95% CI 0.75 to 0.95).3 Another meta-analysis reported no recurrences among 299 laparoscopic obturator hernia repairs with mesh.6
Total extraperitoneal (TEP) repair and transabdominal preperitoneal (TAPP) repair facilitate bilateral obturator, femoral, and inguinal hernia repair with extraperitoneal mesh placement.8–12 The abdomen should be explored if there is concern for bowel ischemia after reduction (ie, TEP would be inadequate).
The Kugel approach provides access to the external obturator canal opening and distal hernia sac using a single suprainguinal incision.13 Opening the sac prior to hernia reduction facilitates bowel inspection, potential resection, and preperitoneal mesh placement. This technique is useful when an abdominal approach would be challenging.14
Overall, current evidence suggests that an initial laparoscopic approach is appropriate for obturator hernia repair in patients without suspicion for perforation. Mesh should be considered, either at initial presentation or as a second-stage procedure if the operative field is contaminated.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TA participated in background research, data acquisition, article writing, and article editing. KEB and DS participated in conceptualization, planning, and article editing. JC participated in conceptualization, planning, design, and article editing. All authors provided final approval of the article and figures prior to submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.