Article Text

Statistics from Altmetric.com
- extracorporeal membrane oxygenation
- thoracic surgical procedures
- fracture fixation, internal
- rib fractures
Case presentation
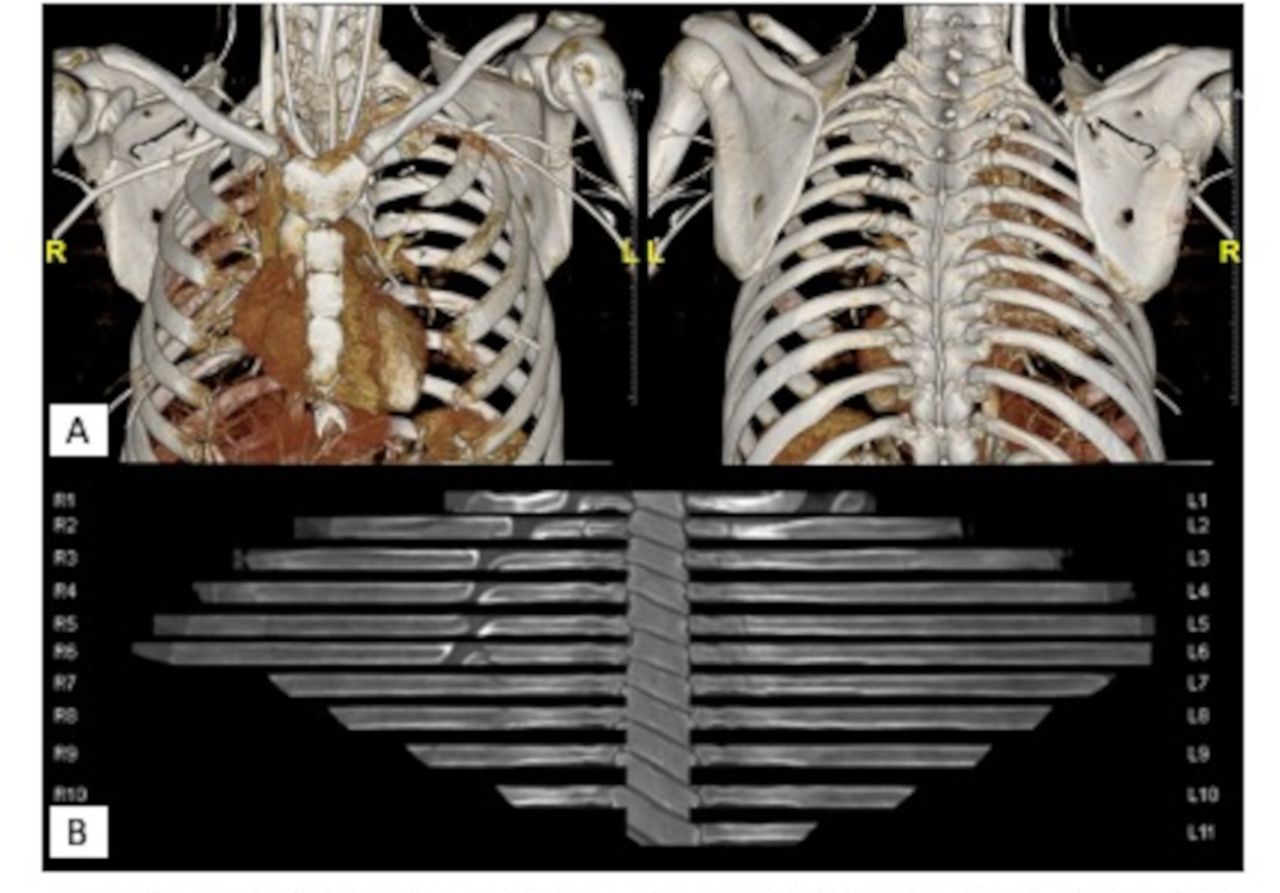
An individual in their 20s presented to our trauma center via flight transfer from an outside hospital after sustaining multisystem trauma as a helmeted motorcyclist. The patient arrived intubated with two right-sided chest tubes and one left-sided chest tube. Clinical exam identified flail chest and flail sternum, right pneumothorax with right pneumomediastinum, and extensive subcutaneous emphysema (see figure 1). The patient’s persistent hypoxia prompted bedside bronchoscopy, which revealed a 25% circumferential tear in the right middle lobe bronchus proximal to takeoff.
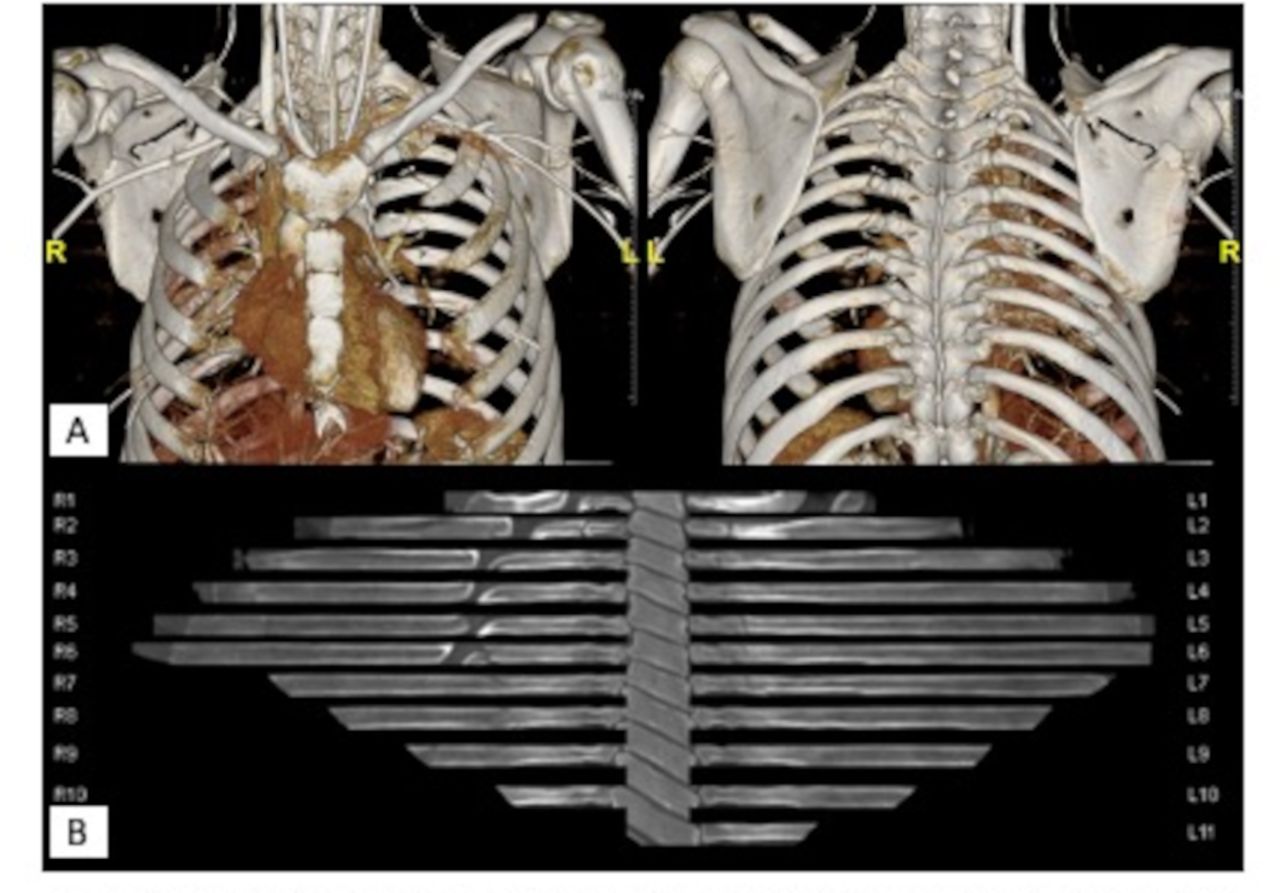
Bilateral rib fractures with flail segment, as seen in (A) three-dimensional reconstruction of initial CT and (B) flattened image of the chest wall.
Additional injuries identified after CT included left grade 1 kidney injury, right superior pubic ramus fracture, left sacral fracture, left L5 inferior facet fracture, left sacral ala fracture with extension to left S1 and S2 foramina, right L1 to L4 transverse process fractures, right scapular body fracture, severe contusions of the right lung (severe blunt pulmonary contusion with >20% of the lung contused), and multiple comminuted and segmental rib fractures of right ribs 2 to 10 and left ribs 2 to 7.
After resuscitation, the patient was brought to the operating room on hospital day 3 for surgical stabilization of their rib fractures and sternomanubrial separation, given the presence of flail chest and sternum. During positioning, the patient became profoundly hypoxemic, at which point the procedure was aborted. Despite repeat bronchoscopy and initiation of inhaled nitric oxide, the patient’s ability to oxygenate worsened.
What would you do next?
Abort to procedure and return to intensive care unit (ICU).
Abort procedure, return to ICU, and reattempt plating when pulmonary contusion is improved.
Abort procedure, initiate Venovenous (VV) extracorporeal membrane oxygenation (ECMO) .
Abort procedure, initiate VV ECMO, perform rib plating once the patient is hemodynamically stable.
What we did and why
Abort procedure, initiate VV ECMO, perform rib plating once the patient is hemodynamically stable.
The patient was initiated on VV ECMO and on hospital day 7, they were hemodynamically stable, but the paradoxical chest wall movement of their chest wall and sternum persisted. They were taken back to the operating room where they underwent open reduction and internal fixation of right ribs 5 and 7 to 9 and left ribs 2 and 3 and sternal fixation as well as cryoneurolysis of right intercostal nerves 4 to 8 (see figure 2). Rib plating was performed with the patient in the right lateral decubitus position for right posterior repair, with left anterior and medial fractures being repaired with the patient supine.

Postoperative posterior to anterior chest X-ray demonstrating hardware placement.
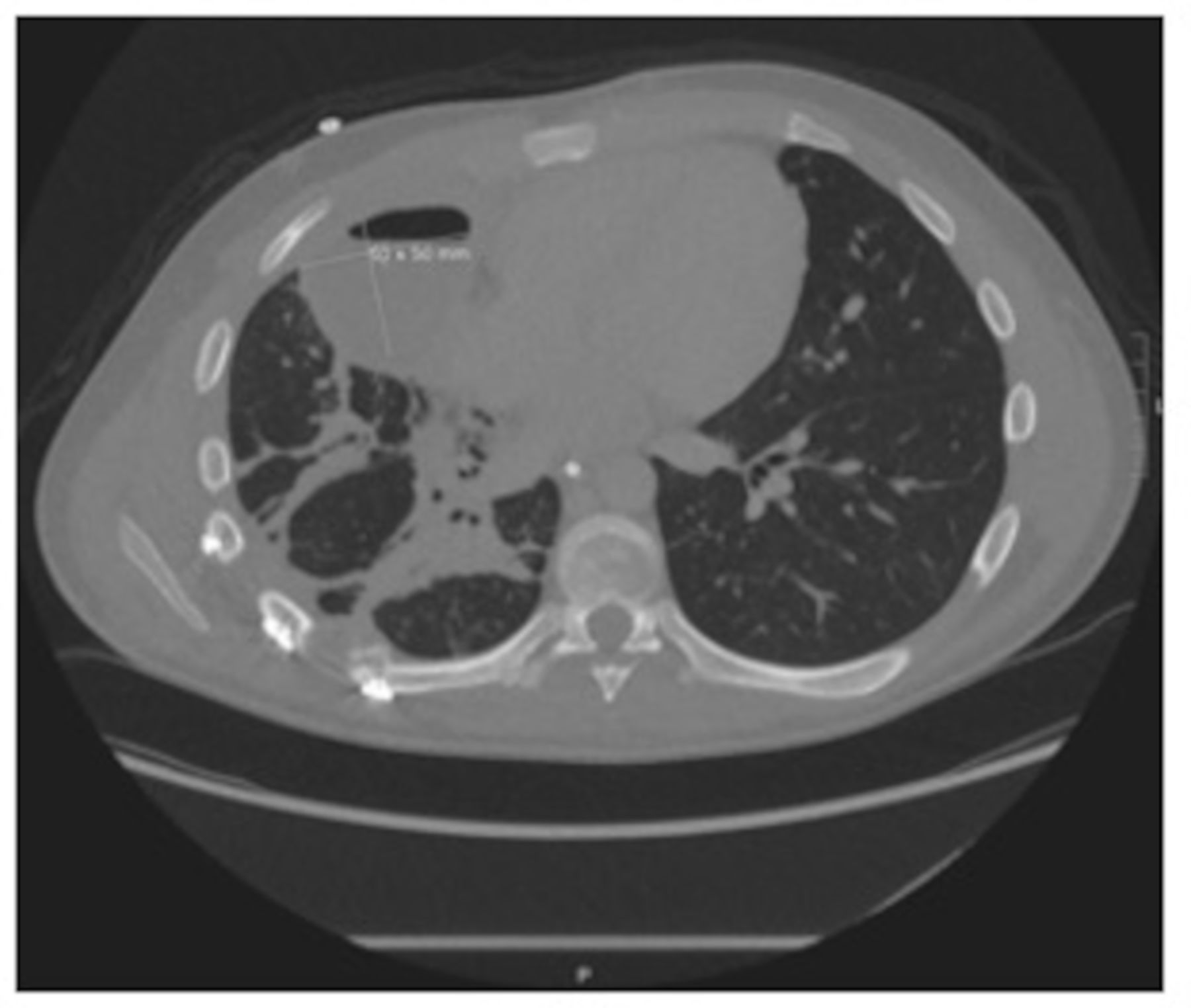
The patient’s subsequent hospital course was notable for the development of polymicrobial pneumonia. By hospital day 15, an empyema had developed (see figure 3). This was treated with antibiotics, a placement of a right-sided pigtail and administration of tissue plasminogen activator/dornase to assist with drainage. Their leukocytosis, fever, and other systemic signs of infection gradually improved without hardware explantation. The patient was decannulated from ECMO on hospital day 24. Tracheostomy collar trials were initiated within 48 hours of decannulation and were well tolerated. They were ultimately discharged to home.
{kind=link}
{kind=link}
{kind=link}
CT of the chest demonstrating anterior right chest empyema.
The application of surgical stabilization of rib or sternal fracture to patients requiring VV-ECMO is rare. Review of the literature revealed a single report of rib plating in a patient on VV-ECMO.1 In our case, using ECMO provided an opportunity to stabilize the patient’s physiology enough to treat their otherwise mobile chest and sternum. An empyema should be treated according to the American Association for Thoracic Surgery guidelines. A recent dual society best practice guideline statement underscores no evidence for additional antibiotics or drainage, beyond that which is already done for empyema management in the setting of surgical stabilization of rib fractures.2 While active infection adjacent to surgically implanted hardware would typically prompt hardware explanation, we demonstrate here that non-operative treatment, using antibiotics and local drainage for source control, may present a viable alternative option to avoid removal of hardware.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Twitter @davidhindin
Contributors YF was responsible for planning, conduct, conceptualization, writing of the original draft, reviewing, and editing. DH was responsible for planning, conduct, conceptualization, writing of the original draft, reviewing, editing, and figure preparation. BF and JT were responsible for reviewing and editing. JDF was responsible for reviewing, editing, and supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.