Article Text

Abstract
Objectives Multiple temporary abdominal closure (TAC) techniques are currently used to manage the open abdomen (OA) in severely injured trauma patients, with variability in efficacy and cost. We evaluated the clinical outcomes of two commonly used TAC methods: ABTHERA Negative Pressure Therapy System and whipstitch suture closure (WC).
Methods We conducted a retrospective review of patients who had blunt or penetrating trauma from 2015 to 2021 with OA managed using either ABTHERA, WC, or both. Primary outcomes included overall and intensive care unit length of stay, ventilator days, number of laparotomies, time to definitive fascial closure, and complications (bleeding, evisceration, wound dehiscence, and reoperation). Univariate and multivariate analyses were used to compare baseline characteristics, outcomes, and complications. Potential mediators of the relationship between the type of TAC and outcomes were explored using mediation analyses.
Results A total of 112 TAC were analyzed; 86 patients had a single type of TAC placement (either WC or ABTHERA), whereas 26 had both types. A majority of patients had blunt trauma in both WC (77%) and ABTHERA (76%) cohorts. There were no differences in baseline characteristics, including injury severity (27.5±12.4 and 27.5±12.0 for ABTHERA and WC, respectively). There was no statistically significant difference among individual complications and overall complications (OR=0.622 (0.274 to 1.412)). No differences were found between the outcomes, and any apparent differences seen were mediated by factors such as a higher number of laparotomies.
Conclusion WC is a low-cost option for TAC in trauma, with similar clinical outcomes and complications to ABTHERA.
Level of evidence Level III therapeutic/care management study.
- abdomen
- Wound Closure Techniques
- abdominal injuries
- treatment outcome
Data availability statement
Data are available upon reasonable request. Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Several temporary abdominal closure (TAC) methods exist for the management of the open abdomen (OA) in trauma. In recent years, ABTHERA has become the TAC method of choice, particularly in the USA, although there are limited data comparing it with whipstitch closure (WC), a simple and cost-efficient choice.
WHAT THIS STUDY ADDS
We conducted a retrospective review of trauma patients who underwent TAC of the OA with either WC or ABTHERA. WC patients had similar outcomes and complication rates to ABTHERA.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
In appropriate trauma patients, we demonstrate that WC is an effective and cost-efficient option for TAC of the OA. This has implications for clinical management of the most severely injured abdominal trauma patients. In a global context, the ready availability of WC in low/middle-income countries allows high-quality management of OA to be accessible to all.
Background
Damage control surgery is performed in critically injured patients to control hemorrhage and limit contamination as quickly as possible, prior to the development of the vicious triad of hypothermia, acidosis, and coagulopathy.1–3 Open abdomen (OA), first described in 1897, is part of this approach and facilitates resuscitation after the initial damage control operation, prior to returning to the operating room (OR) for completion of necessary procedures and definitive closure.1 Although OA is not without complications, and has the potential to be overused, it can be a lifesaving measure in appropriate circumstances. Temporary abdominal closure (TAC) techniques are used to minimize complications related to OA. All these measures aim for primary closure of the fascial defect as soon as clinically feasible, after addressing emergent surgical and resuscitation concerns.4 The ideal TAC technique should be quick and easy to apply and remove, facilitate eventual primary fascial closure, be readily available, and affordable.1 3 5 6 Primary skin closure with either running suture (whipstitch closure (WC)) or towel clips is the oldest TAC technique described, and remains the simplest and most inexpensive method.6
More sophisticated TAC techniques evolved as damage control laparotomy with OA became a mainstream approach for severe trauma and emergency general surgery cases. The Bogota bag, essentially a plastic silo, is another relatively simple method where a non-adherent plastic sheet is sutured between the fascial edges of the skin.1 6 The Wittman patch, first described in 1993, consists of two opposite Velcro sheets sutured to the fascia and connected at the midline allowing fast access to the abdomen.1 7 Soon after, in 1995, Barker first described the use of negative pressure in temporary closure with the vacuum pack.1 6 The development of commercially available devices that employed the principle of vacuum-assisted wound closure using a special sponge and self-contained suction machine, such as the KCI VAC Pack, ABTHERA, and other commercially available devices, has led to increased ease of use and rapid growth in popularity of this TAC method.1 4 6
Each TAC method has advantages and drawbacks. Potential complications include wound dehiscence, intestinal evisceration prior to return operation, recurrent abdominal compartment syndrome, loss of abdominal domain with failure to achieve primary closure due to fascial retraction, and enteroatmospheric fistula formation.1 Direct and indirect costs associated with each method also vary substantially. There is currently no consensus on the optimal TAC method. To help address this knowledge gap, we evaluated outcomes and complications in trauma patients who received one of two commonly used TAC methods: ABTHERA or WC.
Methods
Study population
After Institutional Review Board approval (#L20-191), we performed a retrospective review of patients who had OA after blunt or penetrating trauma, managed using either ABTHERA or WC between January 1, 2015 and April 30, 2021. The study was conducted at an American College of Surgeons-verified level I trauma center that serves as the primary teaching hospital and tertiary referral center for a large rural population. There are approximately 4000 trauma admissions per year, of which 10% are penetrating trauma. All trauma cases are managed by a resident team led by board-certified and fellowship-trained trauma critical care attending surgeons, using a 12-hour shift-based full acute care surgery model.8 During the period of this study, there was no formal protocol on when to choose damage control laparotomy, OA, or which type of TAC to use. There was no formal protocol for fluid resuscitation, de-resuscitation, or direct peritoneal resuscitation on these patients in place during the study period. WC was not used in cases of abdominal compartment syndrome; however, in all other cases, the choice of WC versus ABTHERA or another method was guided mainly by the attending surgeon’s preference. The senior author (SD) primarily used WC, whereas other surgeons at the institution tended to opt for ABTHERA, thus allowing a natural comparison to evolve.
Data acquisition
The trauma service maintains a prospectively collected data registry of all trauma patients, including demographics, procedures, injury, and injury severity. Since the type of TAC is not routinely coded, we obtained a list of patients who had exploratory laparotomy plus another abdominal surgery during the study period using the trauma registry. The list was then manually screened, and all patients who had OA and underwent TAC with ABTHERA or WC were included in the study.
Data were obtained from the electronic medical record. Operative reports were reviewed for the TAC method: ABTHERA or WC. The indication for TAC of the first OA was recorded from the surgical operative note, and categorized based on most commonly described indications. These were: diffuse ooze that was packed, questionable intestinal viability/intestinal anastomosis/delayed anastomosis and the surgeon wanted a second look, inability to approximate fascia due to edema, the patient was unstable, or the patient had a poor prognosis and was not expected to survive. Patients were defined as unstable if the operative note indicated that the patient was hypotensive, coagulopathic and hemodynamically unstable on pressors. Outcomes included length of stay (LOS), intensive care unit (ICU) LOS, ventilator days, time to definitive closure, duration of TAC placement, number of laparotomies, number of reoperations, and mortality. Here, the time to definitive closure was defined as the time from TAC placement to definitive fascial closure. Duration of TAC placement was defined as the time from TAC placement to the time of TAC removal. The number of reoperations was defined as the number of operations after TAC removal. Complications including bleeding episodes, intestinal evisceration, surgical site infection (SSI), organ space infection, and wound dehiscence were recorded after review of the operative reports and follow-up notes up to postoperative day 30.
When extracting complications, bleeding episodes were defined as bleeding requiring unplanned re-exploration of the abdomen. Evisceration was defined as the protrusion of bowel between WC sutures and through the sponges of the ABTHERA; only cases that required intervention (ie, reoperation) were included. Wound dehiscence was defined as clinically apparent separation of the wound edges at the suture line. SSI and organ space infection were defined according to Centers for Disease Control and Prevention guidelines.9
Statistical analysis
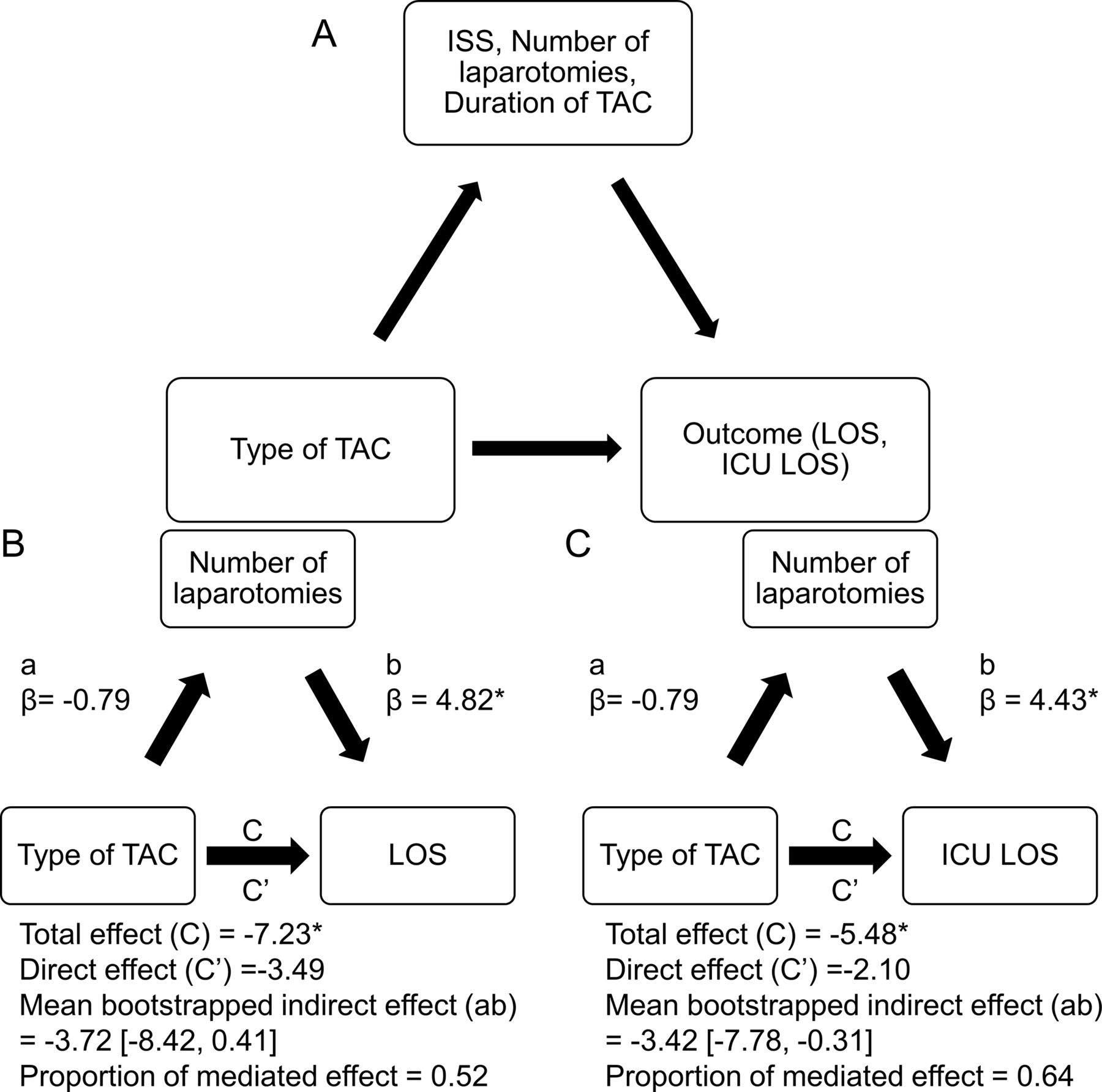
All analyses were conducted using R statistical software (R V.3.5.3). The normality of the distribution for the continuous variables was assessed using Shapiro-Wilk normality test and QQ plots. If the Shapiro-Wilk normality test was significantly different (p<0.05) or QQ plots indicated that the distribution of the data was significantly different from a normal distribution, non-parametric tests (eg, Wilcoxon rank-sum tests) were conducted. Independent sample t-tests with Welch-Satterthwaite correction or Wilcoxon rank-sum tests were performed to compare continuous variables, and Fisher’s exact test or χ2 test was used to compare categorical variables. Summary statistics were represented as mean±SD for parametric variables or median (IQR) for non-parametric variables. Considering the nested nature of the data within subjects, a mixed-effects model was attempted. However, since the mixed-effects model did not converge, necessity of using such model for the analysis was examined by computing intraclass correlation coefficient (ICC). As informed by extremely low ICC linear regression, modes were used for analyses. Univariate and multivariate linear regression analyses (continuous variables) and logistic regression were performed to compare baseline characteristics and examine the linear associations between each TAC type and outcomes and complications. Complications related to TAC method were compared using a logistic regression model after adjusting for patient-hours associated with having each technique. Mediation analysis was performed to detect if differences in demographic and management-related factors mediate the association between two different TAC methods (ie, ABTHERA, WC) and outcomes. This analysis tested the effect of the type of TAC method on the mediator (a), as well as the effect of the mediator on each outcome (b) (figure 1A). Potential mediators were identified using multivariate regression (online supplemental table S1). Mediation of the association between TAC type and continuous outcomes was examined using the Sobel’s method.10 CIs were computed using a preseeded bootstrap approach using mediation package in R.
Supplemental material

(A) Path diagram for mediation analysis to determine the indirect effect of ISS, number of laparotomies, and duration of TAC placement on the outcomes (LOS and ICU LOS). Mediation models for (B) LOS and (C) ICU stay. *Indicates statistical significance p<0.05. ICU, intensive care unit; ISS, Injury Severity Score; LOS, length of stay; TAC, temporary abdominal closure.
Results
Patient characteristics
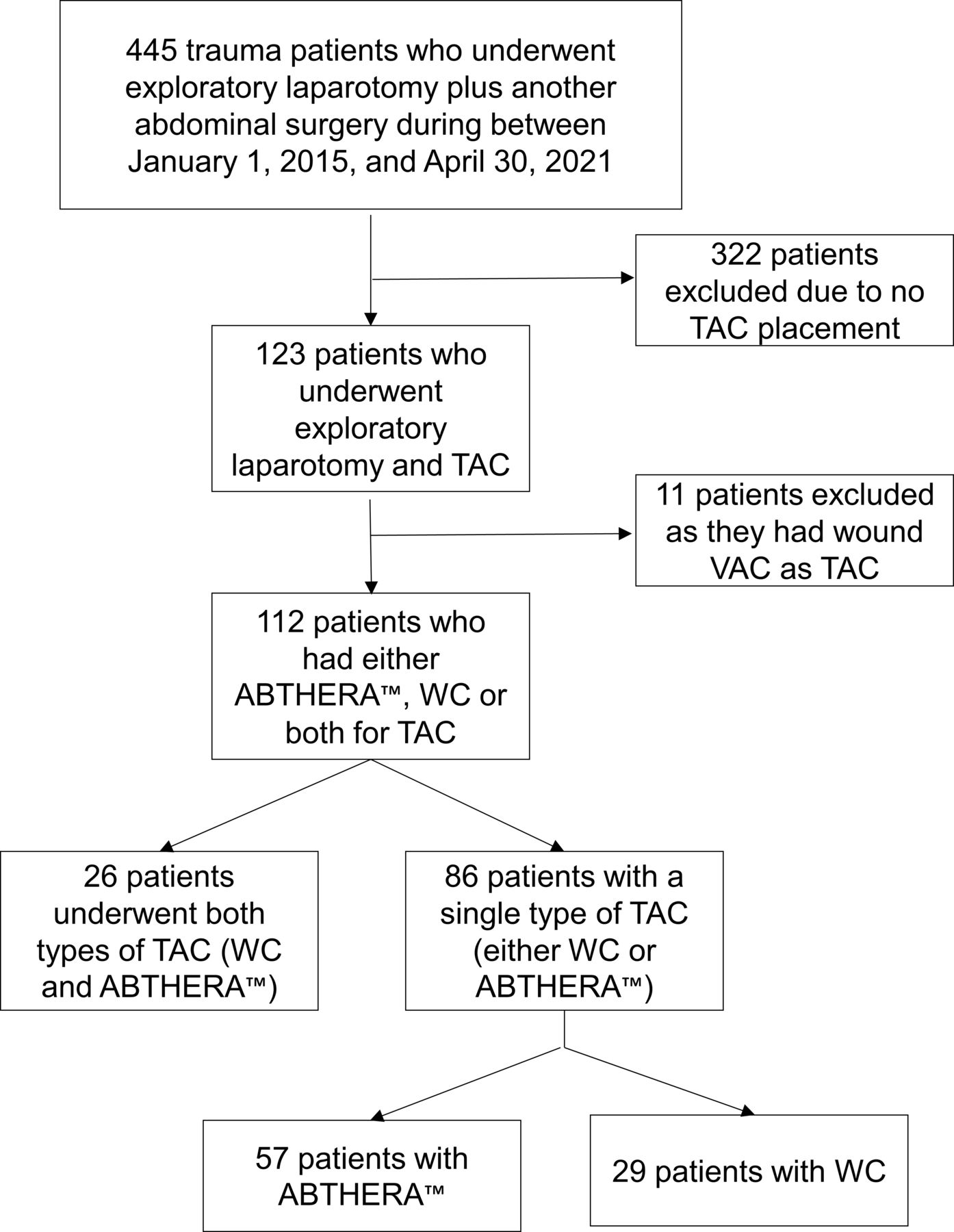
A total of 112 TAC were analyzed: 86 patients had a single type of TAC placement (either WC or ABTHERA), whereas 26 had both types during the stay (figure 2). Among patients who had both methods, 17 (65%) had WC first, then ABTHERA. For patients who had WC first, the switch occurred an average of 3.3 days after the index operation, and for those who had ABTHERA first, the switch occurred an average of 0.8 days later. When considering the whole sample, a median of 95.3 (319.6) patient-hours were managed by applying ABTHERA and a median of 30.45 (28.9) patient-hours were managed by WC (p<0.001) (table 1). There was no significant difference between patients with ABTHERA or WC in terms of age, body mass index, Injury Severity Score (ISS), American Society of Anesthesiologists, or mechanism of injury (table 1). There was a difference in the indication for TAC of the first OA among patients receiving either WC or ABTHERA (p<0.001) (table 1). The most common indication for WC patients was diffuse ooze that required packing (49%), whereas the most common indication for ABTHERA patients was hemodynamic instability (26%). A comparison between patients receiving a single type of TAC (either ABTHERA or WC) and patients who had both TAC methods is presented in the online supplemental tables S2 and S3.
Patient demographic characteristics
{kind=link}
{kind=link}
CONSORT diagram of screening methods for inclusion of trauma patients who underwent exploratory laparotomy and TAC placement. CONSORT, Consolidated Standards of Reporting Trials; TAC, temporary abdominal closure; VAC, vacuum-assisted closure; WC, whipstitch closure.
Postoperative outcomes and complications
Univariate analysis showed a shorter LOS (p=0.026) and ICU LOS (p=0.030) with WC (table 2). Multivariate analyses showed no association after correcting for ISS, the number of laparotomies, and TAC placement duration. However, the mediation analyses showed that the association between type of TAC and LOS and ICU stay was mediated by having a higher number of laparotomies only. The estimated proportions of mediated effects for LOS and ICU LOS were 52% and 64%, respectively (figure 1B,C). There was no difference in ventilator days and time for definitive closure between the two groups (p=0.183 and p=0.071, respectively). Similarly, no significant difference was seen in mortality among ABTHERA (21%) or WC (27%) (p=0.476).
Patient outcomes
Bleeding, wound dehiscence, evisceration, and reoperation rates were not different with WC (table 2) than ABTHERA when controlled for the duration of TAC applied. Moreover, the overall complication rate was not different with WC than ABTHERA (OR=0.622 (0.274 to 1.412)) when controlled for the duration of TAC applied.
Discussion
When evaluating TAC techniques, WC had similar outcomes to ABTHERA in terms of ventilator days and time to definitive closure. However, duration of TAC placement was significantly shorter in the WC cohort. The differences in LOS and ICU LOS between the two groups were governed by trauma and injury-related confounding factors (eg, the number of laparotomies). Further, complications including bleeding, wound dehiscence, evisceration, and reoperation were comparable between WC and ABTHERA. Given similar outcomes and complication rates, this study demonstrates that WC is a reasonable option for TAC of the OA in appropriate trauma patients.
Similar to other published literature of OA in trauma, this is a relatively small series of patients. Although the study was conducted at a high-volume, high-acuity level I trauma center, with approximately 4000 admissions per year, only 112 patients were treated with OA in 6 years. This represents fewer than 1% of our patient population. The low utilization of OA reflects a consensus among our trauma team that damage control surgery, although lifesaving in certain situations, is not without its drawbacks. There is an increasing awareness in the global trauma community, reflected in recent literature, of the downsides of an OA, especially when maintained for a prolonged period.11
In recent years, several studies have established ABTHERA as the TAC method of choice, especially in the USA.3 5 12–15 Ease of use of a prepackaged device and uniformity of a commercially available device across institutions, which allows surgeons to perform the same procedure each time in the same way as their peers, are likely responsible for this popularity and rapid increase in use during the past decade. However, negative pressure dressing systems such as ABTHERA are not without their limitations, including the relatively high costs of commercial dressings compared with ‘home-made’ alternatives that use existing OR supplies.4
Only a handful of studies provide an evaluation of ABTHERA and WC, which is not surprising given that WC is a very old, basic surgical technique with no associated propriety or commercial interest, and investigators tend to focus on what is novel and innovative. Several systematic reviews have attempted to determine the optimal TAC technique, but results are limited due to their small sample size of WC patients.7 16–18 Other retrospective reviews have focused on negative pressure devices only, stating that skin-only closure techniques have largely been abandoned due to increased risks of evisceration, infection, and recurrent abdominal compartment syndrome.3 4 16
Several retrospective studies comparing WC closure against other methods such as Bogota bag, modified Barker’s vacuum packing, and ABTHERA6 19 have shown beneficial outcomes with WC. For instance, Patel et al19 found that LOS, number of explorations, time to closure, and ventilator days were significantly lower in patients undergoing skin closure than bridge (Bogota bag, artificial burr) vacuum-assisted devices. However, only 11% were trauma patients in their cohort of patients who underwent TAC. Similarly, Hu et al6 found that patients with skin-only closure had significantly higher rates of fascial closure and lower hospital mortality compared with patients receiving ABTHERA, Bogota bag, or a modified Barker’s vacuum pack for TAC. However, in their study, the cohort who underwent primary skin closure had a lower injury burden than the other TAC methods, which should be recognized when evaluating their results.
In contrast, both cohorts in the current study had comparable injury severity at presentation, with similar proportions of blunt and penetrating trauma, and a larger sample size than prior literature. Indications for the first OA in each group were similar, except there was a higher proportion of WC patients with diffuse bleeding that was packed, or with a poor prognosis who were not expected to live, suggesting a higher injury burden in these patients. Despite this, we found no difference in outcomes of WC to ABTHERA in terms of ventilator days, time until definitive closure, or death. Even though univariate analysis showed superior outcomes related to LOS and ICU LOS, these results were mediated by other trauma-related factors such as a larger number of laparotomies. When evaluating the results in this context, there was ultimately no difference in outcomes when evaluating the two methods, and the outcomes were comparable.
Regarding complications, although some studies showed no difference, other authors have reported worse outcomes with WC.3 4 16 Several prior studies note that WC has largely been abandoned due to the high risks of complications. These studies raise concern for evisceration, intra-abdominal hypertension, infection, and recurrent abdominal compartment syndrome, with rates reported from 13% to 36% with the use of WC.3 4 16 Although limited in sample size, Kruger et al20 report high complication rates in their cohort of patients undergoing emergent laparotomy and skin-only closure in South Africa. Of their 25 patients undergoing skin-only closure, 70% developed a postoperative complication, with 28% developing an SSI. The results from our current study vary significantly from these findings, although differences in country, clinical setting and practice, and injury mechanism may explain some of this variation. The current study findings of no adverse increase in complications with WC are supported by another recent study from Hu et al6 that showed no significant difference in complications when comparing WC with ABTHERA. Similarly, in our study, WC had a similar overall complication rate than ABTHERA when controlled for the duration of TAC application.
Due to the 12-hour shift-based model used at our institution, the surgeon performing the index operation was not necessarily the surgeon performing subsequent operations; thus, 26 patients received both closure methods during their stay. Regarding the patients who had both methods, most (65%) had WC first then ABTHERA. Surgeon preference largely drove the decision whether to use WC or ABTHERA. As such, certain surgeons, including the senior author (SD) primarily used WC, whereas others primarily used ABTHERA. Our findings indicate that the switch to ABTHERA happened later, an average of 3.3 days postoperatively, compared with the switch to WC, which occurred an average of 0.8 days postoperatively. Given the later transition from WC to ABTHERA, it is possible that the surgeon started with WC and transitioned to ABTHERA when they could not primary close, although this was not generally explicitly stated in the operative note. This introduces possible bias, which should be acknowledged when evaluating the results of the patients receiving both methods.
Although we did not conduct a formal cost analysis, the price difference between WC and ABTHERA warrants comment. Although prices vary at each hospital in the USA based on negotiated contracts, at the institution where this study was conducted, the nylon suture (usually size 0–2) on a cutting needle used for WC closure ranges from $1.71 to $3.91 a suture, and one to two sutures are used for each patient. In comparison, each ABTHERA dressing kit is $478.40, a cost that is repeated with each dressing change. Thus, there is a substantial cost savings to the patient and healthcare system associated with WC versus ABTHERA TAC placement.
Healthcare costs are a major concern throughout the world, especially in low-income to middle-income countries; therefore, the economic component is an important practical consideration when selecting the appropriate TAC method. Each year, 5.8 million people worldwide die from traumatic injuries, with 90% of deaths occurring in low-income to middle-income countries.21 Barriers driving these abysmal statistics include lack of access, availability, and affordability of surgical care, as well as limited resources necessary to provide appropriate care.22 23 Thus, low-cost surgical management strategies can make a major impact in limited resource settings. The implications of our findings of similar outcomes and complications of WC to ABTHERA in trauma patients requiring a period of OA management may benefit surgeons in resource-limited settings by providing the low-cost and readily available option of simple suture closure. As stewards of surgical and trauma care, it is important that surgeons participate in systemic decisions to ensure we use the limited resources at hand to benefit the greatest number of patients.
Limitations of this study include the design as a retrospective single-center study and the resulting small sample size, although this is still one of the largest to date evaluating WC patients. Ideally, the preliminary data generated by this study will form the basis of a prospective, multicenter collaborative trial that can provide more robust information on this critically injured patient population. Second, this was a convenience sample, with the decision for WC versus ABTHERA based on which surgeon was on call when the patient arrived, rather than a randomized controlled study, which would clearly have been preferable. Despite this, the two groups were well matched in trauma-specific clinical criteria at baseline, so it is doubtful this introduced much meaningful bias into the results. Since the decision was based on attending surgeon habitual preference, it is possible the difference in outcomes is due to the difference in clinical aptitude and practice between surgeons; however, as this study was conducted at an institution using a full shift-based ACS model, the surgeon doing the operation was not necessarily the surgeon providing all the subsequent ICU care and decision-making and may or may not have been the surgeon performing the next operation. Given that multiple surgeons were involved in each patient’s care, we would expect any individual surgeon effect to be significantly mitigated in the final results. Third, there were differences in patient groups who received a particular TAC, which precludes interpreting these findings as a head-to-head comparison. For instance, since the ability to perform WC is predicated on the ability to approximate skin, that alone excludes patients with massive visceral distention that may have prevented skin approximation. Similarly, patients who underwent decompressive laparotomy for abdominal compartment syndrome would not receive WC, whereas patients who were not expected to survive, and received TAC simply to be transferred out of the OR prior to inevitable demise, disproportionately received WC. Finally, since there were a few patients who required a complex, staged abdominal wall reconstruction using fascial traction techniques after a period of time on ABTHERA, this may have contributed to the longer time to fascial closure present in this group. The indications for TAC in the first OA are also subject to bias since they were extracted from the surgical operative note; however, due to the retrospective nature of the study, objective metrics were not available for this data point. Despite the limitations acknowledged, as a result of the findings of this study, the trauma team at our institution has switched almost entirely to WC of the OA where feasible in the trauma population, reserving ABTHERA only for cases where abdominal compartment syndrome has been diagnosed.
Given the multiple confounders inherent in any study performed in this critically ill and complex population with multiple injuries, it would be unreasonable to make sweeping generalizations regarding which is the better method based on retrospective data alone. Instead, we suggest these findings justify viewing WC as a viable TAC option, with similar outcomes and lower cost than commercially available alternatives, for patients in whom this method is feasible. Among the TAC options available for OA in critically ill trauma patients, WC is an effective and cost-efficient option. This should be considered in appropriate patients when determining the optimal technique for temporary closure of an OA.
Data availability statement
Data are available upon reasonable request. Data are available upon request.
Ethics statements
Patient consent for publication
Acknowledgments
The study group would like to thank the Clinical Research Institute at Texas Tech University Health Sciences Center for their assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at Presented at Southwestern Surgical Congress April 2022, Wigwam, Arizona, USA. The content presented in this article has not been previously published nor is it currently under review for publication.
Contributors RC contributed to literature search, data collection, writing, and critical revision. CSD contributed to writing, data analysis, data interpretation, and critical revision. EM and BM contributed to data collection and critical revision. SD contributed to conceptualization, study design, and critical revision and is responsible for overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.