Article Text

Statistics from Altmetric.com
Case presentation
The patient is a 71-year-old man with a history of normal pressure hydrocephalus status post ventriculoperitoneal (VP) shunt placement and prostate cancer status robot-assisted radical prostatectomy (RARP) and radiation therapy. The patient was re-evaluated by the neurosurgery service for a shunt malfunction and subsequently underwent a proximal shunt revision. On postoperative routine X-ray of the shunt, the peritoneal portion was found incarcerated within a previously unrecognized right inguinal hernia and suspected to be the actual cause of the malfunction. On reflection, the patient did notice a right inguinal bulge after his shunt placement but did not think anything of it at the time. CT scan of the abdomen and pelvis confirmed the catheter resided in a right inguinal hernia, also containing fluid (figure 1).
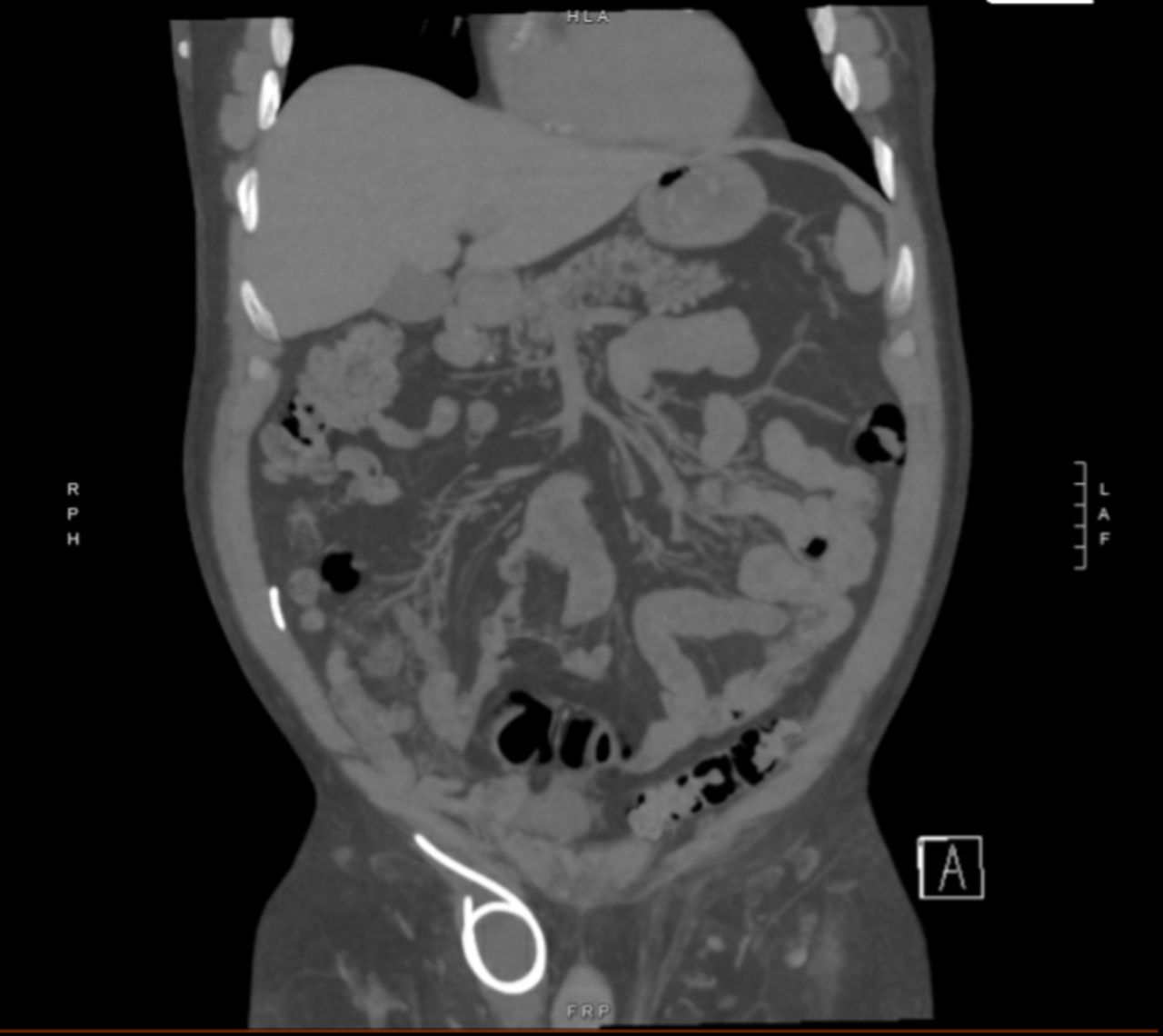
Coronal section of CT scan demonstrating the shunt catheter present in the right groin.
What would you do?
Observation and serial monitoring for spontaneous reduction of the shunt.
Return to the operating room for laparoscopic shunt revision alone.
Return to the operating room for laparoscopic shunt revision and open hernia repair.
Return to the operating room for laparoscopic shunt revision and laparoscopic extraperitoneal hernia repair (total extraperitoneal repair).
What we did and why
C. Return to the operating room for laparoscopic shunt revision and open hernia repair.
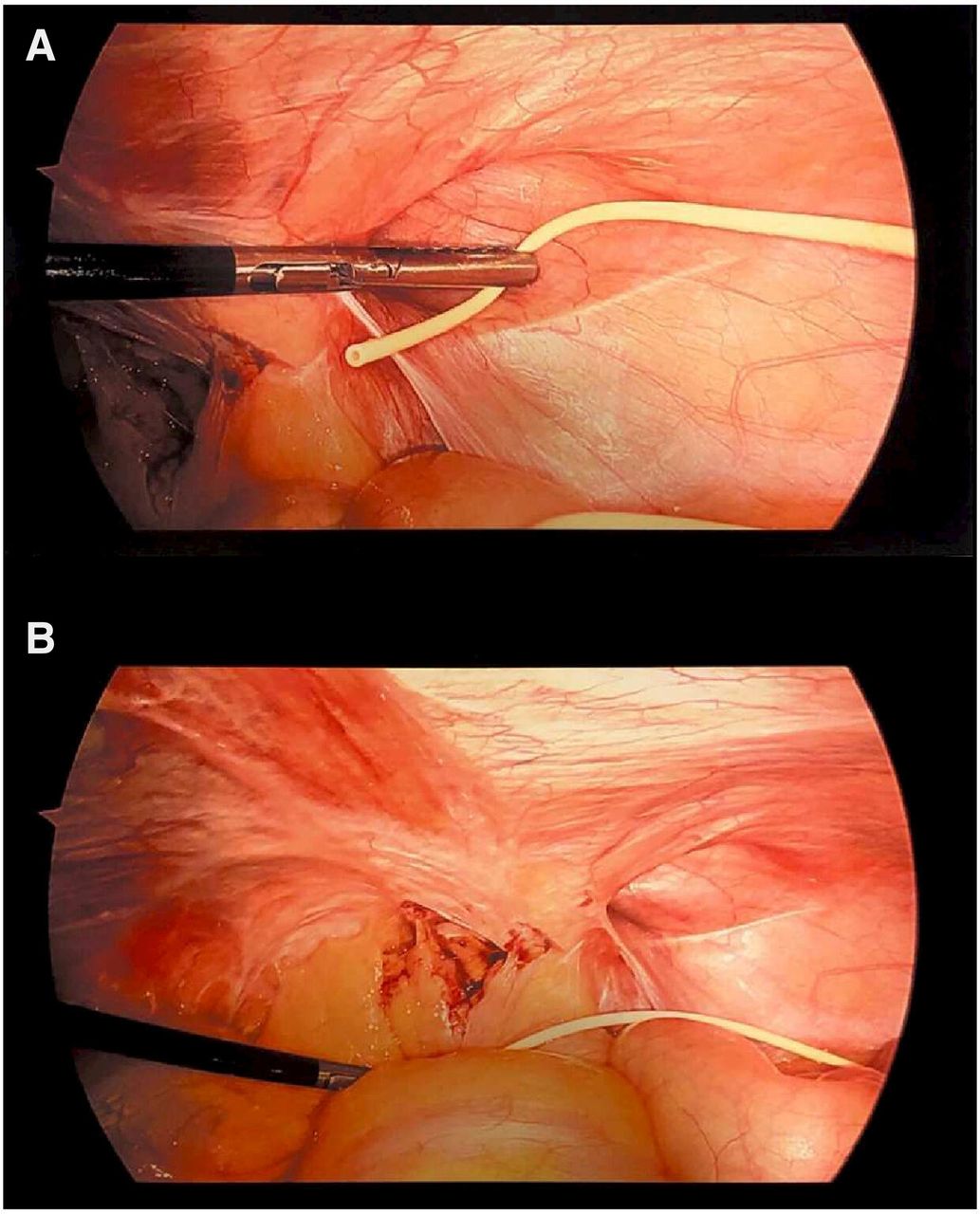
We elected to proceed with urgent diagnostic laparoscopy with distal shunt revision and open hernia repair to prevent further shunt malfunction. The patient was brought to the operating room and placed in supine position, where general anesthesia was induced. We began with a diagnostic laparoscopy with the intention to reduce the catheter, obtaining abdominal access with the Hasson technique. After insufflation, we noted that the catheter had self-reduced and was situated next to the hernia in the abdomen (figure 2). We placed the catheter in the pelvis and turned our attention to the hernia via an open approach. We identified a right indirect inguinal hernia, and separated and reduced the hernia sac from the cord structures. We performed a Lichtenstein open repair of the hernia using the Covidien Mesh Hernia Plug and Patch. The patient recovered appropriately and was discharged the following day.

{kind=link}
{kind=link}
(A) Laparoscopic examination of the right internal inguinal ring with the ventriculoperitoneal shunt tip situated beneath. (B) Laparoscopic examination of the right internal inguinal ring and ventriculoperitoneal shunt tip prior to repositioning of the shunt in the pelvis.
To our knowledge, there are only two cases of VP shunt migration into the scrotum in adults. In one case, this was managed with laparoscopic distal catheter trimming.1 In another case, scrotal perforation from the shunt occurred and the shunt was replaced entirely.2 Neither case described simultaneous hernia repair at the time of shunt revision. We discussed trimming the shunt, but as the inguinal hernia was symptomatic we thought that it was appropriate to proceed with hernia repair. In addition, electing for no repair or delayed repair would have posed an increased risk of repeat occurrence of shunt migration. Our selection of an open approach to repair was based on the consideration that our patient had a history of RARP and thus a previous violation of the preperitoneal space would make a laparoscopic total extraperitoneal repair more difficult, if even feasible at all. Additionally, there was some concern of having mesh in contact with cerebrospinal fluid (CSF) fluid with a preperitoneal repair (transabdominal preperitoneal (TAPP)), and thus we thought that an open repair would be the safest option.
In general, VP shunt incarceration in inguinal hernias has been studied in the pediatric population but has rarely been reported in adults.3 Among the pediatric population with newly identified inguinal hernias, the incidence of incarceration of shunt catheters has been estimated to be as high as 20%.4 This is suggested to be related to the accumulation of volume in the peritoneal cavity, which may pose risk to the development or enlargement of hernias. The fact that this complication has been largely described in the pediatric population may be due to the greater proportion of congenital hernias from a patent processus vaginalis as compared with adults, where most inguinal hernias are acquired from fibromuscular weakening of the abdominal wall.
In our experience, diagnostic laparoscopy with concurrent open inguinal hernia repair may be safely performed in a patient with a history of lower abdominal surgery and VP shunt. Although VP shunt incarceration in an inguinal hernia remains a rare complication, it is important to recognize this as a potential cause of a VP shunt malfunction and consider repair approach based on individual patient profile.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was not required by our institutional review board given that this case report does not fall under the classification of research as determined by our institution.
Footnotes
Contributors Conceptualization: VL, KY, and JT. Clinical management: KY and JT. Writing - original draft: VL and JT. Writing - review and editing: VL and JT. Figure preparation: VL and JT. Supervision: JT.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.