Article Text

Abstract
Background The prevalence of diverticulitis has steadily increased during the past century. One possible complication of large bowel diverticulitis (LBD) is the concurrent development of a small bowel obstruction (SBO). The literature regarding these joint diagnoses is primarily limited to small case series from the 1950s. Consequently, no official recommendations or recent literature exists to guide decision making.
Methods This is a retrospective case–control study with 5:1 matching by demographics, comorbidities, and Hinchey classification of patients presenting with concomitant LBD and SBO and patients with LBD alone. The primary outcome assessed was the need for same admission surgical intervention.
Results Patients with concurrent LBD and SBO were more likely to require surgical intervention (OR 4.2, p<0.001) and more likely to receive an open operation than patients with only LBD (p<0.001). The length of stay (LOS) was longer for LBD with SBO (mean LOS +3.2 days, p=0.003).
Discussion Patients with concurrent LBD and SBO are more likely to fail non-operative management. Given this, along with their longer LOS and higher rate of open surgery, earlier surgical intervention may improve outcomes and reduce hospital LOS.
Level of evidence 4.
- diverticulitis
- small bowel obstruction
- general surgery
- colostomy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Sigmoid diverticulitis (large bowel diverticulitis (LBD)) and small bowel obstruction (SBO) are two of the most common indications for surgical admission in the USA. The prevalence of LBD and SBO is increasing, with each accounting for approximately 300 000 hospitalizations per year in the USA.1 As an isolated entity, the majority of diverticular disease can be managed in the outpatient setting; however, it carries potential for severe illness and multiple complications. One complication that has not been well described is SBO.
Limited data exist regarding patients with SBO complicating an episode of LBD. Unlike the complication of a large bowel obstruction due to localized inflammation at the site of diverticulitis, SBO is presumed to be related to fibrinous exudate or bowel wall involvement with an abscess. In 1958, Bodon and Lapuz2 published a series of cases of SBO in the setting of acute diverticulitis. They identified a group of patients that progressed with increased abdominal distention and dilated loops of small bowel on imaging. Two out of the three patients included required surgical resection of the sigmoid colon without surgical intervention on the small bowel, whereas the third case resolved without operative intervention.2 In a subsequent case series, Kim et al3 identified 16 patients with CT imaging diagnostic of SBO and acute diverticulitis. All of the patients in this series required surgical intervention to address the diverticulitis without small bowel resection.3
As management for LBD continues to trend toward non-operative therapy with antibiotics and drainage procedures as the mainstay of treatment, it is important to identify patients who will fail non-operative management and in whom early surgical intervention may be beneficial. Current recommendations of the American Society of Colon and Rectal Surgeons and the World Society of Emergency Surgery include a strong recommendation for emergent surgery in patients who develop diffuse peritonitis.1 4 An additional indication for operative intervention includes failure to improve with non-surgical management.5 The exact indications for surgical intervention and the definition of “failure to improve” are poorly defined, with large variability. Furthermore, the surgery performed is often dependent on the surgeon caring for the patient. Despite sigmoid resection with primary anastomosis being shown as a safe alternative to Hartmann’s procedure in the majority of patients, it has repeatedly been shown to be a less utilized procedure.6 Overall, in the USA, up to 57% of patients treated surgically for acute diverticulitis will receive a colostomy, which can result in numerous complications ranging from electrolyte abnormalities to the development of hernias. Additionally, many individuals given a colostomy in an acute setting will never have the ostomy reversed.6
Similarly, most isolated SBOs are managed conservatively, with approximately 22% requiring surgical intervention.7 Since most obstructions resolved without surgery and rarely does a delay in surgery cause a difference in long-term outcomes, a non-operative approach is often first attempted. A patient with an underlying diagnosis of sigmoid diverticulitis who develops concurrent SBO raises an interesting clinical decision. Based on the limited available literature, we hypothesized that patients with concurrent LBD and SBO would be more likely to require surgical intervention and have longer hospital length of stay (LOS) compared with patients with only LBD.
Methods
Electronic health records at a single, large, independent academic medical center were reviewed. All patients over the age of 18 with a diagnosis of LBD who presented between July 2011 and June 2016 were included. Patients were first identified by International Classification of Diseases Ninth Revision (ICD-9) code for LBD and were then subdivided by ICD-9 code for SBO. Patients were excluded from analysis if documentation indicated they required urgent operative intervention on initial evaluation or if they were immediately placed on comfort/hospice care. Data were collected with the aim to match patients with small bowel obstruction to no obstruction based on age, race, sex, presence of prior abdominal procedures, and diabetes. After elimination of patients with incomplete medical records, a 5:1 matching was performed based on age, race, sex, presence of prior abdominal procedures, and diabetes status.
Outcomes of interest include LOS, time to operation, procedure performed, creation of an ostomy, mortality, postoperative infection, and discharge disposition. Procedures that began as an exploratory laparotomy and those that began as a minimally invasive surgery but required conversion to an open procedure were considered “open.” Unadjusted analysis was performed, and subsequently an adjusted analysis was performed which accounted for Hinchey classification, immunosuppression, congestive heart failure, coronary artery disease, chronic lung disease, obesity, renal failure, hypertension, and tachycardia. The imaging for all included patients was reviewed by a radiologist and two surgical residents. Hinchey classification was determined by radiographic documentation, and both the Hinchey classification and SBO diagnosis were verified by review of imaging by two surgical residents. An SBO was confirmed if both dilated small bowel and a transition point were identified. Logistic regression was performed for binary outcomes and linear regression for LOS. The researchers were blinded to all patient identifiers and admitting/operative surgeon information to limit any possible bias. A p of <0.05 was considered significant.
Results
A total of 3592 patients with either LBD or LBD+SBO were admitted to our institution between July 2011 and June 2016. We identified 3528 cases with LBD without SBO and 64 cases with concurrent diagnoses of LBD and SBO (LBD+SBO). After excluding 180 patients due to exclusion criteria, a 5:1 match was created which included 170 patients with LBD and 34 patients with LBD+SBO. The 30 patients excluded from the LBD+SBO group were all secondary to incomplete documentation; most notably these patients were transferred from another facility and imaging findings could not be verified regarding SBO status or Hinchey classification. Data on the two groups and their comorbidities can be seen in table 1.
Demographic and comorbidity comparison between the LBD group and the LBD+SBO group
Patients with LBD+SBO were more likely to require surgical intervention for their condition (OR 4.2, p<0.001) and were more likely to require an open operation (OR 5.3, p<0.001). All patients in the LBD+SBO group who required surgery were verified intraoperatively to have an SBO. These patients commonly required enterolysis and a small number also required small bowel resections. This was particularly seen in cases where the small bowel was adherent to the pelvis or was directly involved with the LBD site. Patients with LBD+SBO required an ostomy 41% of the time compared with 12% in the isolated LBD group; however, this was not statistically significant (OR=2.3, p=0.18) (table 2). Patients with Hinchey 3 or 4 diverticulitis trended toward requiring an open procedure more frequently (89% vs. 79%, p=0.46) and had a higher rate of ostomy formation (89% vs. 44%, p=0.001). Similarly, patients who had previous abdominal surgery trended toward higher rates of open operation (100% vs. 78%, p=0.33) but similar rates of ostomy formation (16% vs. 17%, p=1.0). Evaluation of these populations for further subgroup analysis was limited by the small sample size.
Univariate analysis assessing the requirement for a particular intervention between patients with LBD and with concurrent LBD and SBO
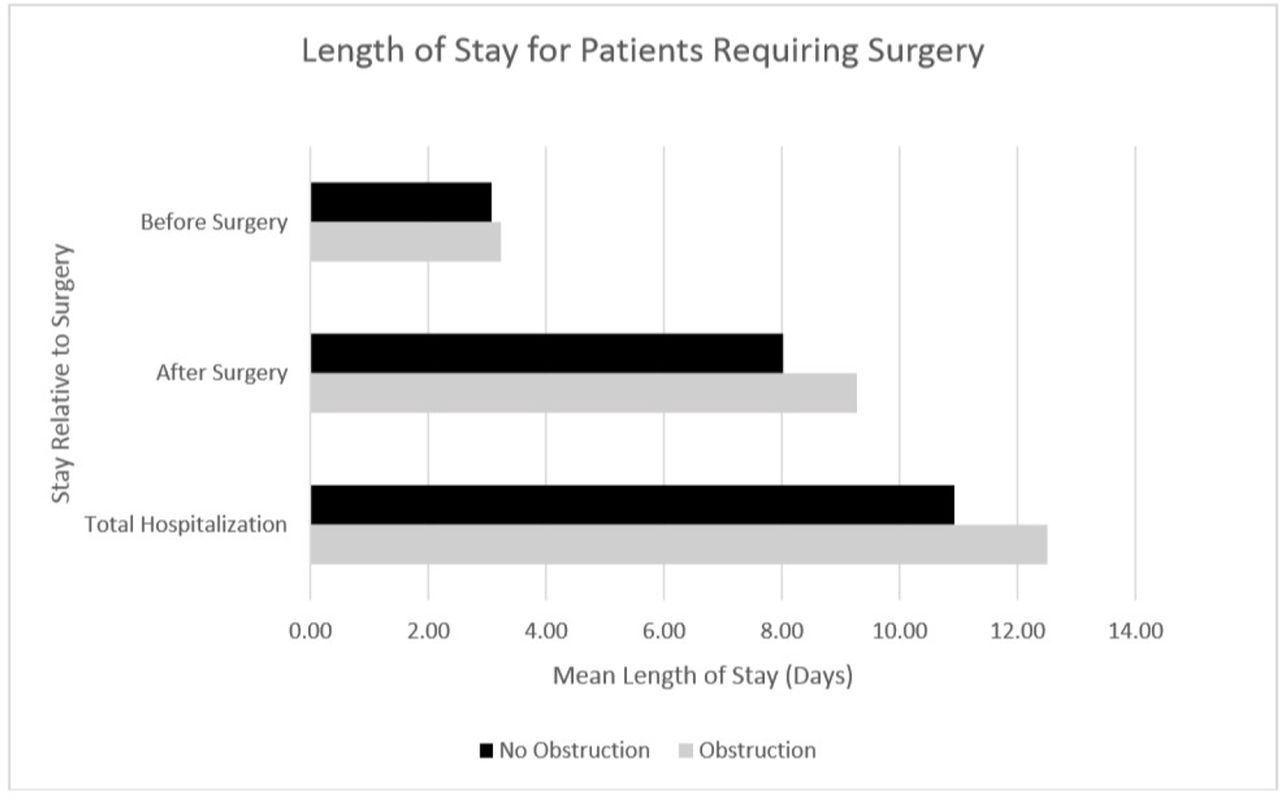
Patients with LBD+SBO had a mean LOS that was 3 days longer than patients with LBD only (p=0.003). The mean LOS for patients who required surgery, regardless of presence of SBO, was 6 days longer than those who did not require surgery (p<0.001). Patients with LBD+SBO who required surgery had similar times to surgery and after surgery as compared with patients with isolated LBD (figure 1).
{kind=link}
Median length of stay of patients who required surgical intervention, relative to starting surgery. “Before surgery” indicates time from admission to entering the operating room. “After surgery” indicates time from completion of surgery to discharge.
There was no difference between the LBD and LBD+SBO groups with respect to postoperative infection rate, discharge disposition, or mortality. The overall postoperative infection rate was 6.4% (OR 1.8, p=0.54). When comparing discharge disposition between either to home or to any facility, there was no significant difference between the LBD and LBD+SBO groups (OR 1.2, p=0.72). The overall mortality rate was low with only five mortalities, with four of these cases occurring in the isolated LBD group (2.4%) and one in the LBD+SBO group (2.9%). There was no difference in mortality between the two groups (p=0.997) (table 3).
Univariate analysis assessing rates of postoperative infection and overall mortality between patients with LBD and with concurrent LBD and SBO
Discussion
LBD remains one of the most common inpatient gastrointestinal diagnoses in the USA. The estimated costs are more than $2 billion annually.8 Modern management of diverticulitis has trended toward non-operative management of most cases that do not meet the criteria for emergent intervention.1 Non-operative management of acute complicated diverticulitis has been shown to be highly successful in up to 91% of patients in recent analysis, whereas additional studies have operative rates closer to 30% for acute complicated diverticulitis.9 10 We have identified a subset of patients with LBD who have concurrent SBO who have a much higher failure rate for non-operative therapy than patients with isolated LBD. Our operative rate of 21% for isolated LBD falls within the previously published rates for surgical intervention; however, patients with concurrent SBO required intervention 53% of the time. Importantly, this higher rate of failure often was due to failure to progress, secondary to the combined LBD and SBO pathologies rather than acute distress. When they did require surgery, this group was more likely to require an open procedure and an ostomy. The decision for ostomy creation was at the discretion of the surgeon and the specific rationale was not always clarified. That said, given the higher rate of both open procedures and ostomy creation, it is likely that the surgeons thought the SBO component made a colonic anastomosis a prohibitively high risk.
Previous studies have started to identify patient subgroups that should prompt more aggressive surgical intervention, including multiloculated abscess, fistula formation, or perforation; however, in the last 20 years, no other studies have examined the subgroup of patients with concurrent SBO.11 We suggest that, although a rare occurrence, with a rate of 1.8% in our study, these patients have a much higher failure rate for non-operative therapy and may benefit from earlier operative intervention. Earlier intervention, prior to progressive small bowel dilatation, may allow higher rates of laparoscopic intervention, as well as allow higher rates of primary anastomosis without ostomy creation.
This study is primarily limited by its retrospective design. Nearly half of the LBD+SBO group were excluded from analysis due to incomplete medical records. Primarily the missing information was related to demographic information, imaging information, and information regarding comorbidities, which prevented inclusion into the matching. The most frequent reason for missing imaging was related to patients presenting through outpatient imaging clinics which were not available for retrospective review. The retrospective design also limited our ability to fully interpret possible additional confounders, including what specific factors prompted surgery or if a patient had declined a surgical treatment option. We do feel that the data presented in this study are generalizable as it incorporated a large patient population being managed by a wide range of surgical specialists, including colorectal surgeons, surgical oncologists, acute care surgeons, and general surgeons. Importantly, care was driven by surgeon preference. During this study period, there was no standardized enhanced recovery after colorectal surgery pathway or diverticulitis management guideline at the institution and patients were excluded from the institutional adhesive SBO guideline given the LBD pathology. Further subgroup analysis of how care differed between surgical specialists may help illustrate practice differences; however, it is beyond the scope of this study as we sought to better understand patient prognosis and disease progression.
Conclusion
Patients with LBD and concurrent SBO have a much higher failure rate for non-operative therapy than patients with isolated large bowel obstruction. Identification of patients who may fail non-operative therapy is important to help guide clinical decision making. Earlier intervention may improve clinical outcomes, such as increasing the rates of laparoscopic surgery and decreasing the rates of ostomy creation.
Ethics statements
Patient consent for publication
Ethics approval
This project was evaluated and approved for patient safety and ethics by the Christiana Care Health System Institutional Review Board (approval number: 603529).
Footnotes
Presented at The data in this manuscript have previously been presented at the American Society of Colon and Rectal Surgeons Annual Scientific Meeting (Nashville, Tennessee, May 19-23, 2018).
Contributors Study conception and design: JG, MSF, MR, RC. Data collection: JG, MSF, MR, RC. Analysis and interpretation of results: JG, MSF, MR, RC. Article preparation: JG, MSF, MR, RC. All authors reviewed the results and approved the final version of the article.
Funding This study was funded by the National Institute of General Medical Sciences of the National Institutes of Health (grant number: U54-GM104941).
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.