Article Text

Abstract
Background Venous thromboembolism (VTE) after an inferior vena cava (IVC) injury is a devastating complication. Current practice involves variable use of anticoagulation and antiplatelet (AC/AP) agents. We hypothesized that AC/AP can reduce the incidence of VTE and that delayed institution of AC/AP is associated with increased VTE events.
Methods We retrospectively reviewed IVC injuries cared for at a large urban adult academic level 1 trauma center between January 1, 2008 and December 31, 2020, surviving 72 hours. Patient demographics, injury mechanism, surgical repair, type and timing of AC, and type and timing of VTE events were characterized. Postoperative AC status during hospital course before an acute VTE event was delineated by grouping patients into four categories: full, prophylactic, prophylactic with concomitant AP, and none. The primary outcome was the incidence of an acute VTE event. IVC ligation was excluded from analysis.
Results Of the 76 patients sustaining an IVC injury, 26 were included. The incidence of a new deep vein thrombosis distal to the IVC injury and a new pulmonary embolism was 31% and 15%, respectively. The median onset of VTE was 5 days (IQR 1–11). Four received full AC, 10 received prophylactic AC with concomitant AP, 8 received prophylactic AC, and 4 received no AC/AP. New VTE events occurred in 0.0% of full, in 30.0% of prophylactic with concomitant AP, in 50.0% of prophylactic, and in 50.0% without AC/AP. There was no difference in baseline demographics, injury mechanisms, surgical interventions, and bleeding complications.
Discussion This is the first study to suggest that delay and degree of antithrombotic initiation in an IVC-injured patient may be associated with an increase in VTE events. Consideration of therapy initiation should be performed on hemostatic stabilization. Future studies are necessary to characterize the optimal dosing and temporal timing of these therapies.
Level of evidence Therapeutic, level 3.
- adult
- venous thromboembolism
- venous thrombosis
- vascular system injuries
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Traumatic injury lends an individual susceptible to venous thromboembolism (VTE) events.
Within injured patients, several cohorts exist that have a higher incidence of VTE, including patients with an injured inferior vena cava.
WHAT THIS STUDY ADDS
This study provides stratification to thromboprophylaxis regimens and suggests that more aggressive prophylaxis can mitigate VTE events.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
On hemostatic stabilization, a clinician should consider initiating appropriately aggressive antithrombotic medications.
Background
Inferior vena cava (IVC) injuries, inclusive of various types, locations, and severities, account for up to 40% of major abdominal vascular injuries and carry a mortality rate of 20% to 66%.1–10 Following injury, surgical exploration and repair can be arduous and inclusive of high-volume bleeding and major risk of death. Patients surviving IVC injury are at high risk of catastrophic complications, including major life-threatening bleeding, IVC thrombosis, deep vein thrombosis (DVT), and pulmonary embolus (PE).4 8–11 The incidence of venous thromboembolism (VTE) has been reported to be 1.1% to 18.9% in DVT and 0.4% to 4.6% in PE.8 9 11
Best practices for antithrombotic prophylaxis in patients with traumatic vascular injury remain unclear, as demonstrated by the American Association for the Surgery of Trauma in the multicenter PROOVIT (PROspective Observational Vascular Injury Trial), which found no consistent approach to anticoagulation across 542 patients with various vascular injuries.12 Surgical repair of the IVC further disrupts the endothelium and may also introduce luminal stenosis, both of which further increase the risk of VTE. In addition, a focal hematoma can compress the vessel, disrupting laminar flow.
This risk, however, must be balanced by acute bleeding concerns after an extensive retroperitoneal dissection needed for surgical repair,13 which can lend a risk of excess bleeding in addition to other concomitant injuries that may continue to bleed (ie, liver laceration, splenic laceration). Additionally, the plausibility of incomplete hemostasis, missed injuries, or iatrogenic injuries must be considered before instituting these modalities. Lastly, if the patient had other injuries that contaminated the repair including enteric contents, fecal contents, or pancreatic enzymes, then there is always the possibility of dehiscing the IVC suture line. This then renders a high-flow, low-pressure catastrophic bleed.
Antithrombotic agents are widely used postoperatively and even beyond hospital discharge to mitigate VTE events, but for patients with IVC injuries specifically no studies have conclusively demonstrated an ideal course for treatment.12 Herein, this study sought to evaluate the relationship between various antithrombotic regimens with the incidence of acute VTE in patients with an IVC injury. We conducted a retrospective clinical study in which our hypothesis was that varied anticoagulant and antiplatelet dose regimens exist, and these regimens will result in a varied incidence of acute VTE events after IVC injury. Such study is necessary as potentially preventable deaths could then be mitigated.
Methods
Patients and data collection
We performed a retrospective observational study at our large, urban, academic, medical center and level 1 trauma center between January 1, 2008 and December 31, 2020. Data were curated from our institutional trauma registry and electronic medical record (EMR). The registry was queried for all patients who sustained a traumatic IVC injury requiring hospital admission. On EMR review, patients who were ultimately found not to have sustained an IVC injury or if they died within the index 72 hours were excluded from analysis. An investigation of cause of death was performed on patients who survived beyond their index operation; however, succumbed to death within the first 72 hours. Furthermore, due to the inherent differences in underline presenting physiology, a patient was excluded from the VTE analysis if they underwent an IVC ligation (online supplemental figure 1).
We classified patients into four cohorts: full-dose anticoagulation, prophylactic dose anticoagulation, prophylactic dose anticoagulation with concomitant antiplatelet agent, and no anticoagulant or antiplatelet agent. During the study period, standard-of-care prophylaxis was based on empiric dosing and not titrated to any measure. Patients were assigned to their cohort depending on their current treatment before an acute VTE event or hospital discharge, whichever occurred first. Therefore, if a patient received full-dose anticoagulation, but they were transitioned to prophylactic anticoagulation before sustaining an acute VTE, then the patient was analyzed in the prophylactic dose regimen. Pre-existing home medications were characterized. Our analysis included any available EMR data up to 6 months postacute hospitalization discharge.
Our primary outcome was the incidence of an acute VTE event. An acute VTE included IVC thrombus (presumed at the site of injury), any DVT distal to the IVC injury (ie, ileac veins), or PE. Only a patient’s first acute VTE event was recorded in the analysis for time to VTE event. If a patient sustained both a DVT and a PE, this was also characterized.
Descriptive variables included patient demographics (age, gender, body mass index), injury mechanism and details (mechanism, Injury Severity Score, Abbreviated Injury Scale score of the abdomen, trauma exsanguination protocol activation), surgical methods (type of operation, IVC filter placement), type and timing of all antithrombotic agents (including discharge regimens), timing of VTE events, and outcomes (mortality, bleeding complications, new VTE events after hospital discharge).
Although this is an observational study, it should be noted that during the investigation period our DVT surveillance protocol underwent several modifications, which may have affected our recorded incidence of DVT detection. Briefly, in the first 4 years of the study period, screening was optional in the high-risk and very high-risk patients; however, it became mandatory for this cohort in 2012. Then, in 2017, screening again de-escalated. When performed, asymptomatic screening typically involved duplex ultrasound imaging of the lower extremities, usually performed within the first 5 days of admission and continued every 5 to 7 days up to either 3 weeks or until three negative duplexes (online supplemental table 1). In addition, imaging was also obtained when clinical suspicion arose, at the provider’s discretion. Article preparation was guided by STROBE (Strengthening The Reporting of OBservational Studies in Epidemiology; checklist provided in online supplemental materials).
Supplemental material
Supplemental material
Results
Of the 84 patients screened from the registry query, 76 sustained an IVC injury on EMR review. 26 met all the inclusion and exclusion criteria. On EMR review, 8 were excluded as they did not have an IVC injury, 23 died in the emergency department, 22 died in the operating room, and 4 died within the index 72 hours (online supplemental figure 1). In addition, one patient underwent an IVC ligation.
Four patients were partitioned into the therapeutic dose anticoagulation. Ten patients received concomitant prophylactic dose anticoagulation with an antiplatelet agent. Eight patients received prophylactic dose anticoagulation. Four patients did not receive any anticoagulation or antiplatelet agents. Of the fully anticoagulated patients, two received a concomitant antiplatelet agent during part of their hospital course.
Overall, 26 (100.0%) were male and the median age was 26 (IQR 16–51). Of the patients, 24 (92.3%) sustained a penetrating injury and 22 (84.6%) sustained a gunshot wound. The descriptors of their injury burden and operative details are listed in table 1, including 24 (92.3%) who went to the operating theater. These 26 patients were admitted by 18 different trauma attendings. Table 2 depicts patients’ injuries, including their cava injuries.
Baseline demographic comparison of the AC and AP cohorts
Description of patient injuries, including a description of the IVC injury
None of the patients were noted to be on an anticoagulant as a home medication; however, one patient in the prophylactic anticoagulation with a concomitant antiplatelet agent was noted to have aspirin and effient as home medications. Four (15.4%) of the patietns had data missing on their home medications.However, none of these four patients had a pre-existing condition warranting an antithrombotic agent.
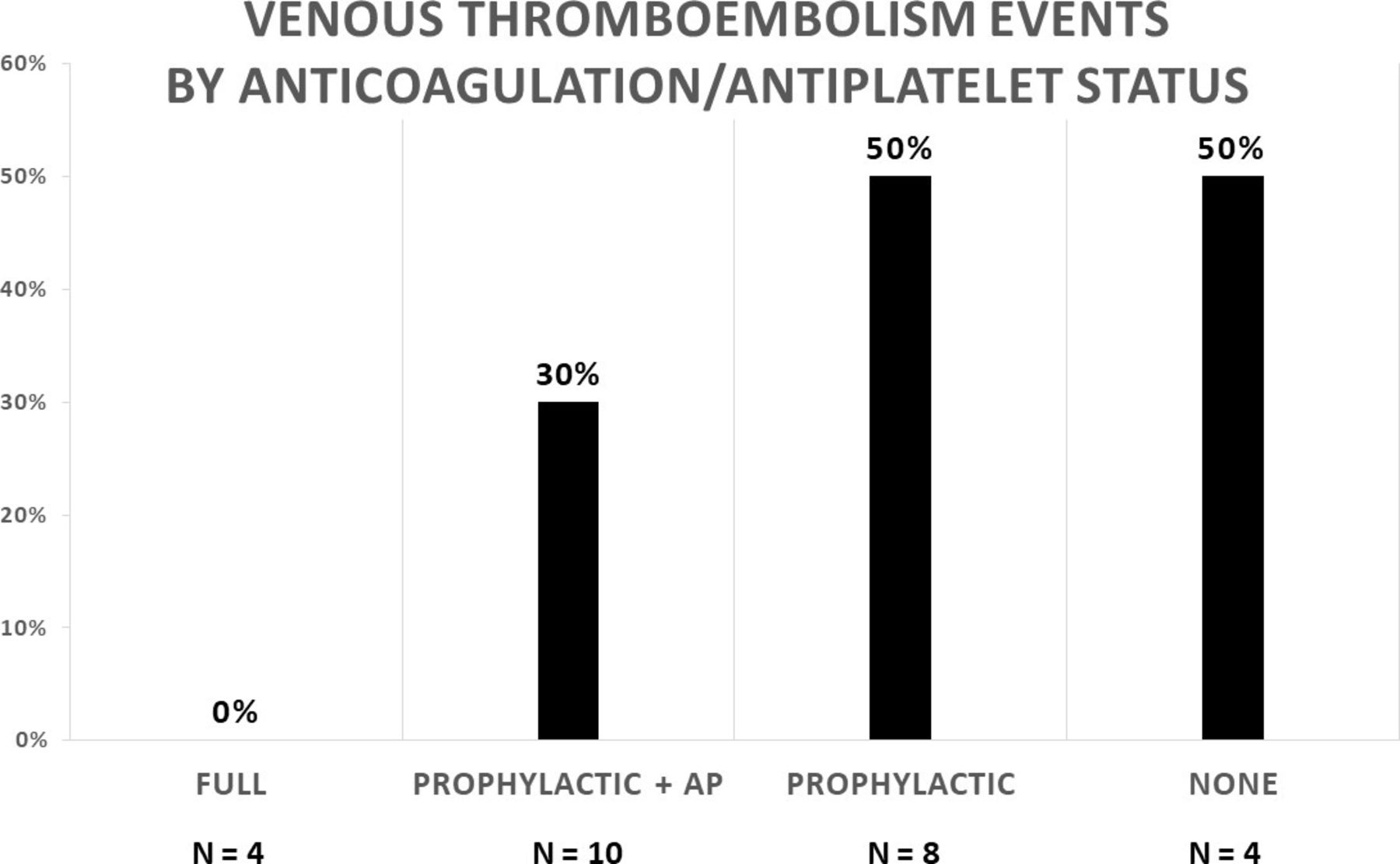
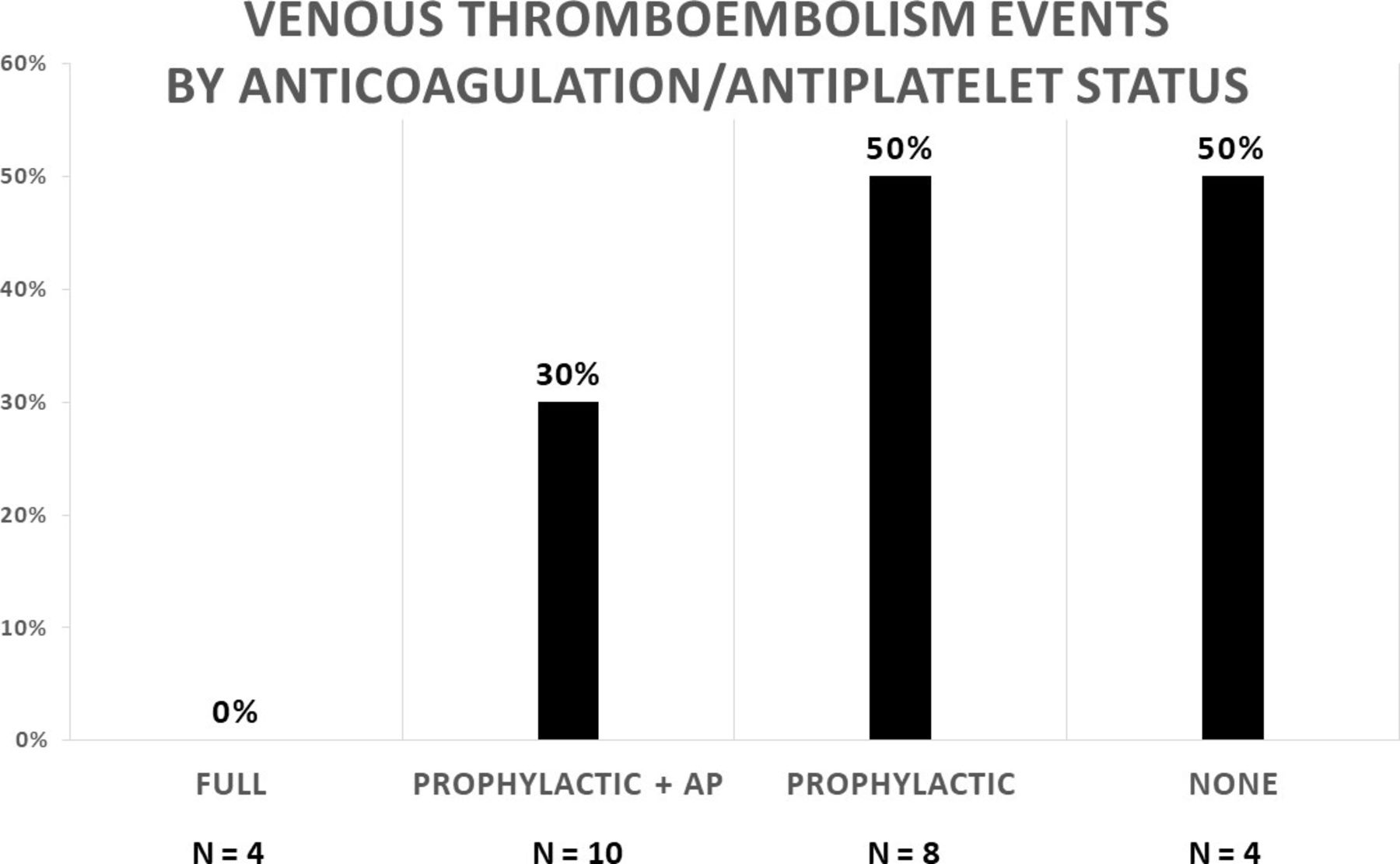
Nine (34.6%) acute VTE events were reported. Four PEs and eight DVTs occurred in nine different patients and the anatomic locations of the DVTs are described in table 3. New VTE events occurred in zero (0.0%) patient in the full-dose cohort, in three (30.0%) patients in the prophylactic dose with concomitant antiplatelet agent cohort, in four (50.0%) patients in the prophylactic cohort, and in two (50.0%) patients without antithrombotic agents (figure 1). Of note, three IVCs were thrombosed, two prophylactic patients and one patient without any antithrombotic agents. Additionally, one prophylactic patient whose IVC was stenosed sustained a right femoral DVT.
{kind=link}
Bar graph with anticoagulation and antiplatelet (AP) as the independent variable and the incidence of acute venous thromboembolism events as the dependent variable.
Location of deep vein thrombosis
Table 4 depicts the antithrombotic regimen throughout the hospital course, including changes to the daily antithrombotic medications along with hospital days of VTE events. Notably, one patient who was classified in the category without receiving antithrombotic agents had been on prophylactic dose anticoagulation from hospital days 3 to 8, then was transitioned to full-dose anticoagulation on day 8. On hospital day 10, the full-dose and prophylactic dose anticoagulation were discontinued due to a gastrointestinal bleed. The patient was then diagnosed with a pulmonary embolism on day 11 in addition to a DVT on day 19. They received an IVC filter on hospital day 11 and their full-dose anticoagulation resumed on hospital day 14. Of the four fully anticoagulated patients, none sustained an acute bleeding complication after full-dose anticoagulation initiation. Online supplemental table 2 provides a detailed account of the bleeding events.
Temporal timing of antithrombotics and venous thromboembolic events by patient
The median days to onset of an acute VTE event was 5 (IQR 1–11). The hospital days that the four cohorts sustained an acute VTE event with their respective median time to receiving anticoagulation and antiplatelet treatment modalities are included in table 5. Notably, the timing only depicts current antithrombotic initiation that the patient is on immediately before a VTE event. All patients who sustained an acute VTE event had undergone primary repair, except for one patient who did not undergo an operation. It should be noted that the incidence of DVT detection increased over time; conversely, the DVT screening process became less aggressive over time.
Hospital day of acute thrombotic event and of anticoagulant/antiplatelet initiation
Online supplemental table 3 depicts patients’ discharge regimens after hospitalization. Most of the patients maintained their hospital regimen. Of note, one patient who was in the prophylactic anticoagulation category sustained a new VTE after discharge. Furthermore, on posthospitalization follow-up, there were expected VTE propagations of previously diagnosed DVTs. Two out of the three IVC that were thrombosed had further propagation distally on outpatient follow-up. Finally, one patient (3.8%) did not complete posthospitalization follow-up.
Of the four patients who died within the index 72 hours, one died immediately after their operation and the remainder had a re-exploratory laparotomy confirming coagulopathy as the cause of their death.
Discussion
Traumatically injured patients often have risk factors that lend them to be hypercoagulable, rendering them susceptible to VTE events.14 15 In this retrospective study of IVC-injured patients, we sought to determine the association between anticoagulation/antiplatelet status and the incidence of acute VTE events. Our results show this group to be very high risk, with a 50.0% acute VTE event rate in patients with prophylactic dose anticoagulation and in patients who were not receiving an antithrombotic agent. On the other hand, those receiving full-dose anticoagulation had a 0.0% acute VTE event rate. These novel and striking findings should prompt consideration of more aggressive anticoagulation/antiplatelet treatment therapies in this high-risk population.
The increased VTE event rate in patients with IVC injuries is thought to occur due to disturbance in the laminar flow through endothelial layer disruption and/or the disruption caused by an outflow obstruction when the repair becomes stenosed.16–19 To capture this pathology, we excluded all deaths within the first 72 hours. Of the 49 excluded patients, 48 died within the first 24 hours and the 49th patient died within the first 48 hours. Excluding these patients ensured that we were more likely to include patients who sustained an acute VTE event as the result of disruption of the laminar flow and less likely to include patients who had a non-survivable injury without enough time to contract an acute VTE.
Our 34.6% incidence of acute VTE events is compatible with the existing body of literature.14 20–28 In a large prospective study of 716 patients, it was found that traumatically injured patients have a high incidence of VTE events, with up to 57.6% incidence in those without prophylactic anticoagulation.14 Our cohort of four patients who did not have prophylactic anticoagulation had an incidence of DVT distal to the IVC injury of 50.0%. Prior literature has suggested that there may be a synergistic effect when antiplatelet agents are combined with pharmacological prophylactically dosed anticoagulants and our findings noted an improvement in the VTE event from 50% to 30% when an antiplatelet agent was added to the prophylactic regimen.29 These findings are strikingly different from those who received full-dose anticoagulation, as our incidence of VTE events in this cohort was 0.0%. The literature on the incidence of acute VTE events has widely variable data, with an incidence as high as 57.6% in the general trauma population and an incidence as low as 1.2% in the traumatic IVC injury population.8 9 14 30 Our fully anticoagulated patients had an event rate lower than what was previously described in the literature; however, there were only four patients partitioned into this cohort.
The strength of our study was the manual extraction of data allowing for detailed determination of the type, dosage, and timing of anticoagulation/antiplatelet initiation and the timing of any acute VTE events. In addition, patients were followed 6 months after hospital discharge for any further VTE events. Regional and national databases may list injuries and complications; however, they do not have the granularity of the treatment regimen provided. There are, however, some limitations to consider. This was a single-center study and the analysis was therefore limited. Operative interventions, VTE prophylaxis, and screening processes may not be the same at all other institutions.
In addition, with a final cohort of 26 patients, our study was underpowered to detect a statistical significance between the various cohorts. This further limited our ability to apply more rigorous excluding parameters, to perform a multivariable analysis or to stratify patients based on a number of confounding variables, as it is plausible that a selection bias exists in our fully anticoagulated patients. Furthermore, the classification scheme is not without inherent limitations. Given that group assignments were made based on the immediate last therapy, length of therapy and missed doses were not accounted for. Such a patient may have undergone a lengthy hospital course without receiving antithrombotic agents or sustaining an acute VTE event and then be placed on full-dose anticoagulation in the days preceding discharge. Consequently, this patient would be classified as receiving full-dose anticoagulation.
Our study also had a high prevalence of penetrating mechanisms with a patient population that was entirely male. Of note, in general female trauma patients31–33 and patients with a blunt mechanism34–36 are more likely to be of the hypercoagulable phenotype than of the hyperfibrinolytic phenotype. IVC filter placement can also mitigate some risk; however, placement is not without risk.37–43 As such, this is a controversial topic that needs further investigation in this population as treatment options vary widely in the literature.44–49 The granularity of our data presented a unique opportunity to demonstrate that patients receiving lower doses of anticoagulation/antiplatelet medications had an overall higher incidence of VTE events, all while not having any major bleeding complications in the fully anticoagulated cohort. This outcome is applicable with the understanding that the level of evidence is insufficient.
Although there is a growing body of literature regarding coagulopathy in traumatically injured patients, there remains a paucity of data regarding trauma subpopulations that may benefit from higher doses of VTE prophylaxis, including IVC-injured patients. We think that future prospective multicenter clinical trials should capture coagulation phenotypes and anticoagulation/antiplatelet initiation practices. These details would serve to inform clinical practice guidelines as future directives decide on how to best handle traumatic IVC-injured patients. Our findings can then facilitate a more robust power analysis for a future multicenter trial.
Conclusion
In this retrospective, single-center, observational study of a large, urban, academic, level 1 trauma center, we found that IVC-injured patients have a high incidence of acute VTE events. There appears to be a lower incidence of acute VTE events in patients who were prophylactically fully anticoagulated compared with patients who had other regimens of antithrombotic agents. Consideration of appropriate anticoagulation/antiplatelet initiation should ensue after hemostatic stabilization. A future prospective multicenter trial should capture the temporal characteristics of anticoagulation/antiplatelet treatment modalities to further inform clinical practice.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study was reviewed and approved by the University of Pennsylvania Institutional Review Board (protocol number: 843994). The investigators adhered to the policies regarding the protection of human subjects as prescribed by the Code of Federal Regulations Title 45, Volume 1, Part 46; Title 32, Chapter 1, Part 219; and Title 21, Chapter 1, Part 50 (Protection of Human Subjects).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AMH, DRS, JSP, PMR, and NM designed the study. AMH, BCB, and MJS searched the literature. AMH, SM, and BCB aquired the data. AMH analyzed the data. AMH, DRS, SM, JSP, PMR, MJS, and NM participated in data interpretation. AMH and BCB drafted the article, which all authors critically revised for important intellectual content and approved the final version to be published. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. AMH accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.