Article Text

Statistics from Altmetric.com
Case presentation
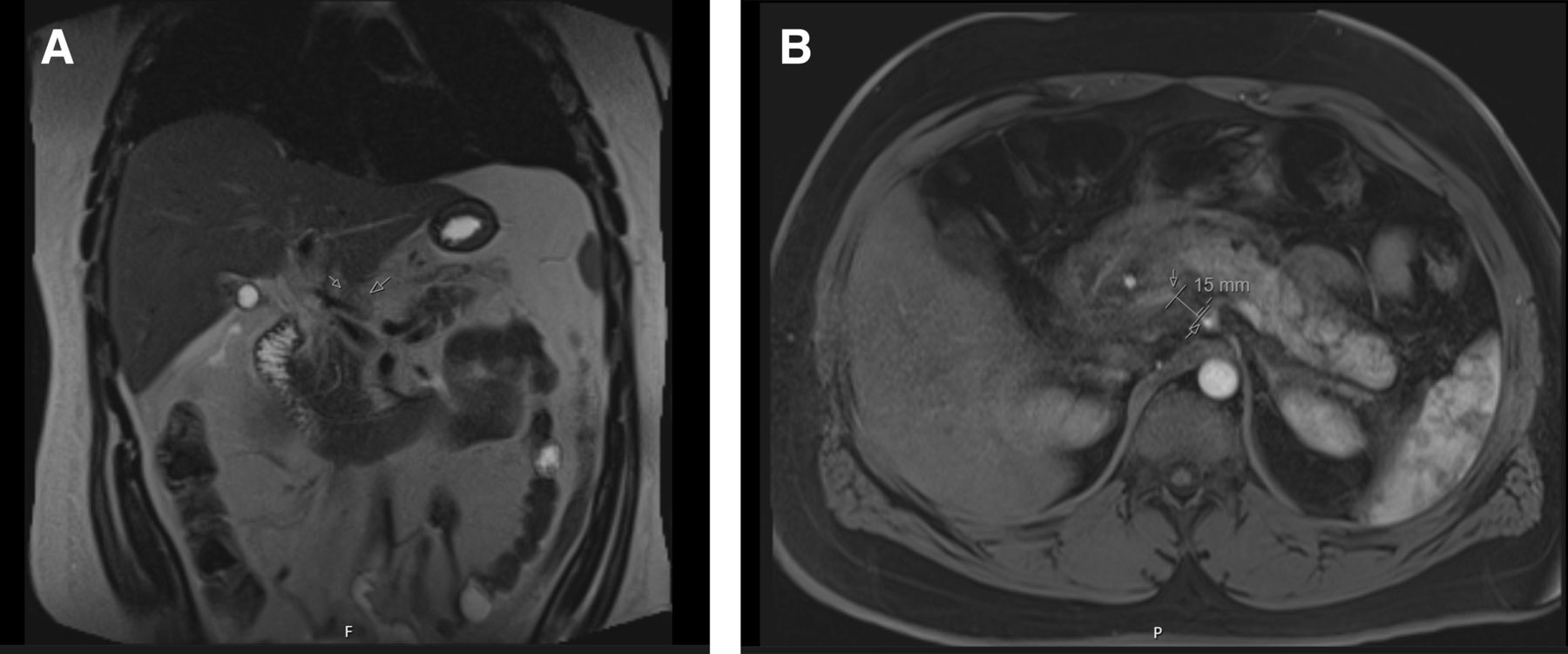
A 34-year-old pedestrian was struck by a vehicle and presented with epigastric tenderness. He underwent an abdominal CT scan which showed a moderate-sized peripancreatic hematoma and a focal interruption of the proximal common hepatic artery without extravasation. He was transferred to our center and arrived in stable condition. Magnetic resonance angiography (MRA) and cholangiopancreatography (MRCP) was obtained and it redemonstrated segmental occlusion of the proximal common hepatic artery with collateral flow from the gastroduodenal artery. There was no evidence of a pancreatic injury (figure 1A,B). One week later, a surveillance abdominal computerized tomography angiography (CTA) demonstrated interval development of a 3.2×2.2 cm common hepatic artery pseudoaneurysm just distal to its takeoff from the celiac artery (figure 2). Immediately after CT, he became unresponsive with a systolic blood pressure of 60 mm Hg.

(A,B) Coronal and axial slices of the MRA of the common hepatic artery one day after injury.

{kind=link}
{kind=link}
Axial slice of the CTA abdomen of the ruptured hepatic artery pseudoaneurysm.
What would you do next?
Take to the operating room (OR) immediately for definitive vascular control
Take to interventional radiology (IR) for angioembolization of the pseudoaneurysm
Place Resuscitative endovascular balloon occlusion of the aorta (REBOA) as a bridge to the OR
Place REBOA as a bridge to IR
Take to a hybrid OR for angioembolization followed by abdominal washout
What we did and why
A REBOA was placed in the intensive care unit and he was emergently taken to the OR for an exploratory laparotomy. A large, peripancreatic hematoma precluded dissection of the common hepatic artery origin. Furthermore, the celiac axis was known to originate from behind the pancreas on his preoperative imaging. Once the area was packed, the REBOA was deflated and the site appeared hemostatic. Interventional radiology then attempted catheter angioembolization of the lesion; however, the absence of a sufficient landing zone within the proximal hepatic artery precluded safe angiographic control. After resuscitation, we returned to the operating room for ligation of the celiac axis. The patient was since been discharged and is recovering well.
Discussion
Blunt injuries to the porta hepatis remain rare. Hepatic artery injuries account for 21% to 44% of all splanchnic artery aneurysms and the majority are intrahepatic when they occur after traumatic injury.1 2 Presentation is typically delayed weeks to months and gold standard for diagnosis remains imaging with arteriography. A high degree of suspicion is required as these may not be readily apparent on the first imaging studies. Rupture may occur into the peritoneum, biliary tract, or gastrointestinal tract.3 4 Mortality rates are highest in those with intraperitoneal rupture with one study reporting a 33% mortality rate.2 The most common interventions include embolization, hepatic artery ligation, no intervention, and hepatic resection in cases of intrahepatic pseudoaneurysm.
Gaining proximal control of the common hepatic artery is often difficult as it often exists deep to multiple important structures. Ligation of the celiac is a known option for controlling significant hemorrhage from any of its many branches, though our literature search did not reveal prior examples of this maneuver to control a bleeding extrahepatic pseudoaneurysm. Certainly, this would not have been feasible had our patient not had good collateral flow from the gastroduodenal artery. Pseudoaneurysms of the proper hepatic artery may prove a more challenging entity in that ligation and embolization may completely take out the hepatic arterial vasculature, despite the proper hepatic artery being in a more anatomically amenable position.
This case highlights the urgency needed in diagnosing and treating these pseudoaneurysms. In this case, placement of REBOA was crucial to temporize the arterial hemorrhage and this demonstrates an example of how this device may be used outside the trauma bay. Treatment of these pseudoaneurysms remains difficult and multiple strategies should be considered including operation, endovascular techniques, or a combination of both. Hybrid operating rooms may be especially useful in these scenarios, though these remain a scarce resource. In our case, our trauma center does not currently use a hybrid OR, otherwise this would have likely been the best place for our patient as he eventually required both angiographic and open surgical procedures. No one method has proven superior for treatment and patient history, hemodynamic stability, associated injuries, hospital resources, and operator abilities should all be considered when making treatment decisions.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Contributors GMN and JY contributed to the drafting of the article. GMN, BS, JC, and JY contributed to editing the final draft of the article. All individuals who met the authorship criteria are listed as authors, and all authors attest that they participated in the study to take public responsibility for its content. All authors certify that they have participated in the study sufficiently to take public responsibility for its content, including participation in the conception, writing, and revision of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.