Article Text

Statistics from Altmetric.com
Case summary
A 45-year-old woman with remote history of Roux-en-Y gastric bypass presented with acute-on-chronic epigastric abdominal pain and new-onset hematemesis. Her nasogastric tube output was coffee ground and there was a palpable left-sided mass with focal tenderness. Her CT scan revealed an intussusception with a small bowel obstruction at the jejunal common channel, with proximal bowel dilation and distal bowel decompression. We performed a multistep surgical procedure. First, we performed a damage-control laparotomy, during which about 25 cm of the intussuscepted bowel was reduced, and an esophagogastroduodenoscopy was performed. We then performed an abdominal re-exploration, during which we identified the lead point to be about 20 cm distal to the common channel anastomosis and resected this segment of the bowel with adequate margins on either end. Given the distance of the involved bowel from the anastomosis, we were able to avoid resection and/or revision of the Roux-en-Y. The patient recovered from surgery without complication and was discharged home on postoperative day 7. She presented to our clinic 3 weeks later and noted to be healing well from surgery, with reported resolution of previous abdominal symptoms.
What would you do?
A 45-year-old woman with remote history of Roux-en-Y gastric bypass presented with acute worsening of chronic epigastric abdominal pain with new-onset hematemesis. She reported an absence of bowel movement or flatus in the past 24 hours.
She reported 3 years of intermittent epigastric pain triggered by certain foods and stress, with chronic constipation. A lack of insurance coverage deterred her from seeking care sooner. She had a marginal ulcer 10 years previously, for which she regularly took a proton pump inhibitor (PPI). She confirmed non-steroidal anti-inflammatory (NSAID) drug use but denied smoking. There were no other pertinent findings on review of systems.
On physical examination, her heart rate was 90 beats per minute and blood pressure was 177/78 mm Hg. Her nasogastric tube output was coffee ground. Her abdomen was soft and non-distended, with a palpable left-sided mass and focal tenderness, without peritonitis. Labs revealed a hemoglobin of 11 g/L and white cell count of 10.8 x 109/L, with a left shift.
CT scan revealed an intussusception with a small bowel obstruction at the jejunal common channel, with proximal bowel dilation and distal bowel decompression. This was unexpected as a bowel obstruction after Roux-en-Y caused by intussusception is rare and there are variable conclusions regarding management. Bowel obstruction after a Roux-en-Y gastric bypass is more likely to be caused by mesocolonic constrictions, narrowing of the jejunojejunostomy, anastomosis, internal herniations, adhesions, and obstructive clots at the gastrojejunostomy.
The patient was admitted to our surgical service. Treatment options included operative and non-operative management. Non-operative management options included an endoscopy for further evaluation and supportive care. Operative management options included possible reconstruction of the Roux-en-Y depending on the location of the lead point and/or the involved bowel segments.
What we did and why
We performed an urgent overnight damage-control laparotomy with intraoperative esophagogastroduodenoscopy (EGD) due to concern for complete bowel obstruction. The laparotomy identified a small bowel obstruction of the jejunum at the common channel of the Roux-en-Y; about 25 cm of the common channel was intussuscepted retrograde into the Roux limb (figure 1). Gentle, manual traction reduced this obstruction. The affected bowel from all three limbs of the bypass appeared thickened and edematous, although viable, making it difficult to assess a true lead point. The procedure did not identify any other abnormalities.
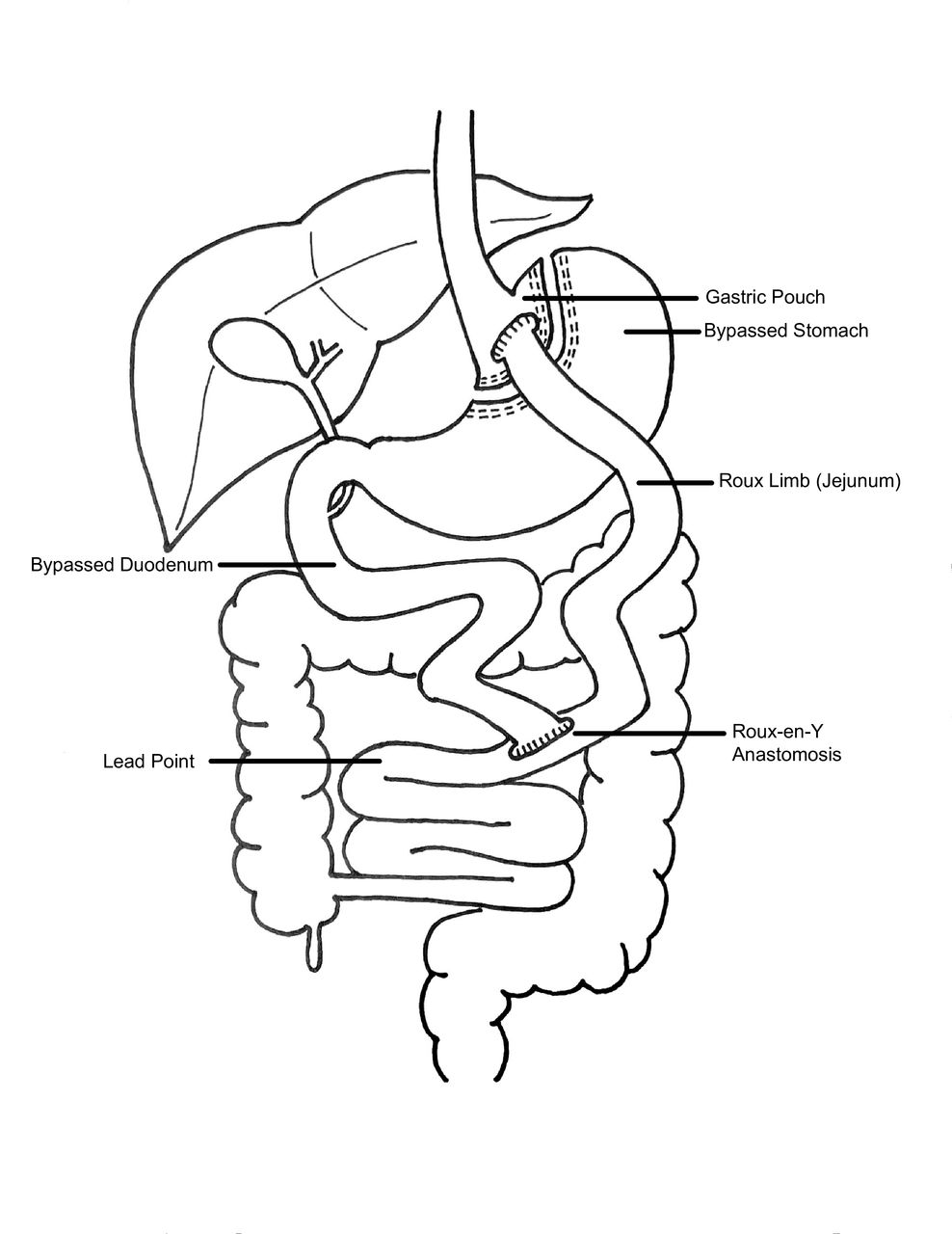
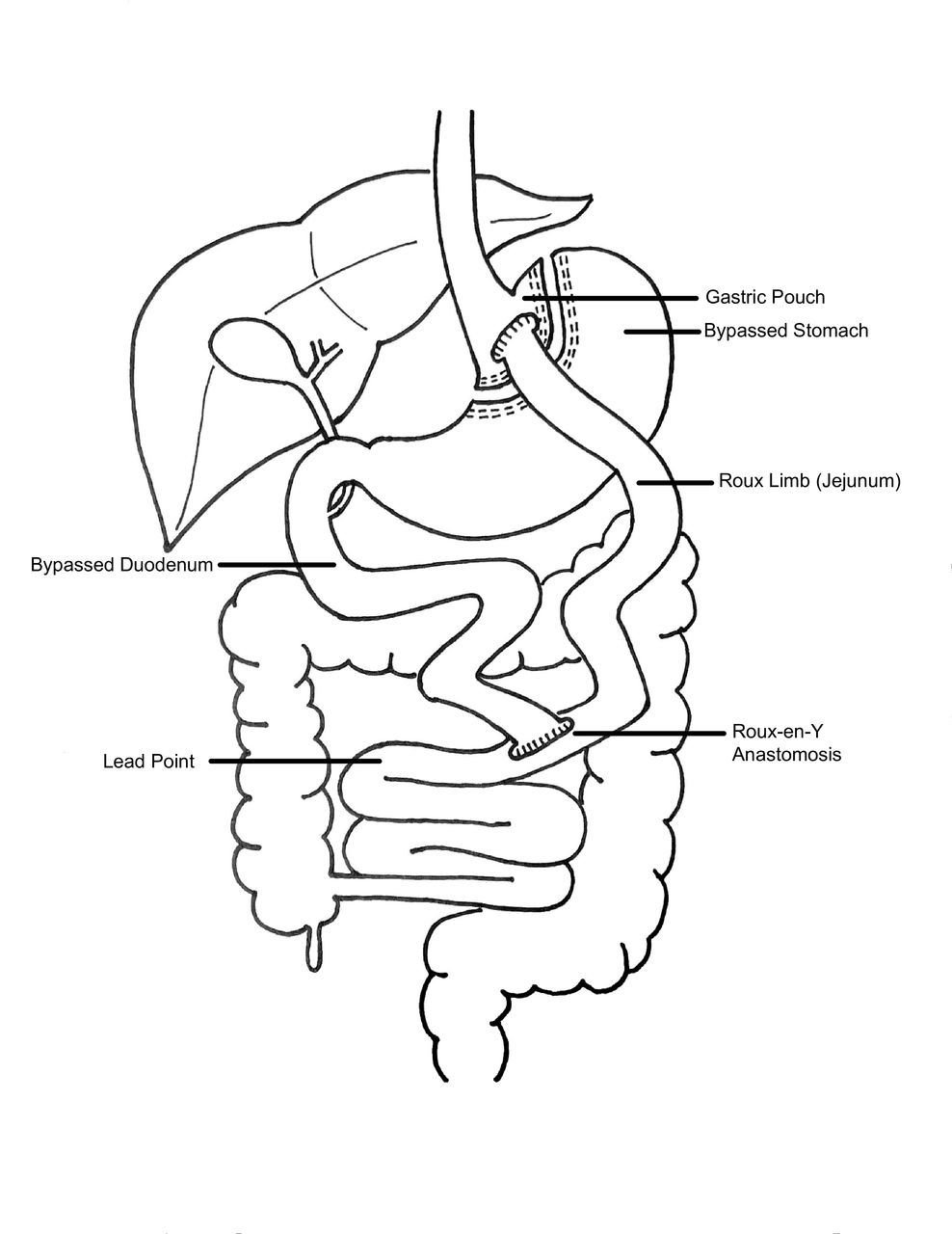{kind=link}
Anatomy of Roux-en-Y gastric bypass with approximate location of intussuseption lead point.
Subsequent EGD revealed friable mucosa at the gastrojejunal anastomosis, with sequelae of ulcer disease, non-bleeding. The jejunum was found to be patent and without ulcer disease.
We wanted to take time to plan appropriately for potential need to surgically revise the Roux-en-Y so we elected to place a temporary abdominal dressing and perform a second-look laparotomy in an elective fashion to allow for better time and resource capabilities. The patient benefitted from this damage-control stepwise operation because it allowed time for the bowel edema to subside and for appropriate surgical planning to occur. Further, this method provided the patient with daytime, non-urgent operating room capabilities. The following day, we performed an abdominal re-exploration, during which we identified an abnormally thickened bowel about 20 cm distal to the common channel anastomosis, with adjacent lymphadenopathy in the mesentery. This appeared to be the lead point. We resected this segment of the bowel with adequate margins on either end, in case of malignancy. Anastomosis was performed in a side-to-side, functional, end-to-end fashion using a 55 cm blue load gastrointestinal anastomosis stapler 6 to 7 cm distal to the common channel connection. The patient’s abdomen was subsequently closed. Given the distance of the involved bowel from the anastomosis, we were able to avoid resection and revision of the Roux-en-Y.
The patient’s Helicobacter pylori IgG was negative. Pathological review of the specimen revealed acute and chronic ulceration within the resected jejunum, but was otherwise benign. The patient recovered from surgery and was discharged home on postoperative day 7. She presented to our clinic 3 weeks later and noted to be healing well from surgery, with reported resolution of previous abdominal symptoms. She resumed her PPI without complications and had appropriate gastroenterology follow-up for her ulcer disease.
Ethics statements
Patient consent for publication
Footnotes
Contributors MM was the primary surgeon for the patient’s surgical care. All authors equally contributed to submission of draft, edits, and finalization.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.