Article Text

Statistics from Altmetric.com
Case presentation
A 14-year-old boy who jumped from the 12th floor was brought to our emergency department and directly admitted to the hybrid emergency room system (HERS). The HERS is a trauma resuscitation room equipped with a CT scanner, fluoroscopy unit, and operating room setup (figure 1).

The HERS at Teikyo University. A CT scanner and fluoroscopy instrument are installed in the trauma resuscitation room, which functions as an operating room and an angio-suite. HERS, hybrid emergency room system.
His vital signs at admission were as follows: Glasgow Coma Scale score, 6 (E1V1M4); heart rate, 132 bpm; blood pressure, unmeasurable; respiratory rate, 18 breaths per minute; SpO2, 89% ; and body temperature, 34.6°C.
The extended focused assessment with sonography for trauma (eFAST) was negative. The arterial blood gas analysis showed a pH of 7.0 and lactic acid level of 14.1 mmol/L. Laboratory tests revealed fibrinogen level 139 mg/dL.
The patient was intubated. Blood transfusion was initiated. The resuscitative balloon occlusion of the aorta (REBOA) was inserted in Zone I under fluoroscopy. The patient’s systolic blood pressure improved to 75 mm Hg. Whole-body CT (WBCT) with an intravenous contrast agent was performed.
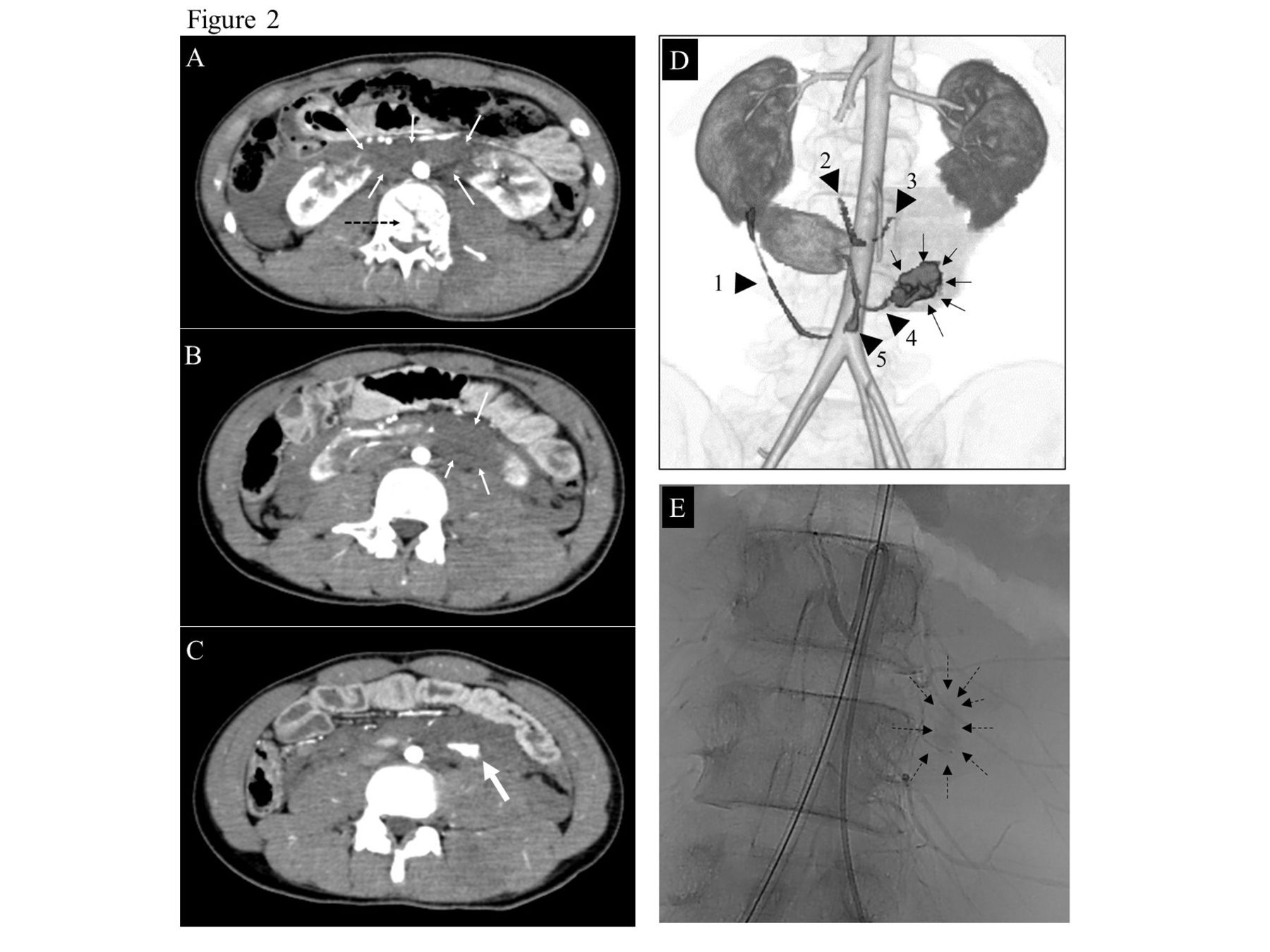
WBCT showed a horseshoe kidney (HSK) injury. Active extravasation of the contrast agent from the lower pole of the left wing of the HSK surrounded by retroperitoneal hematoma was observed (figure 2A–C). Five aberrant arteries from the aorta were feeding the HSK and the extravasation occurred from one of those (figure 2D).
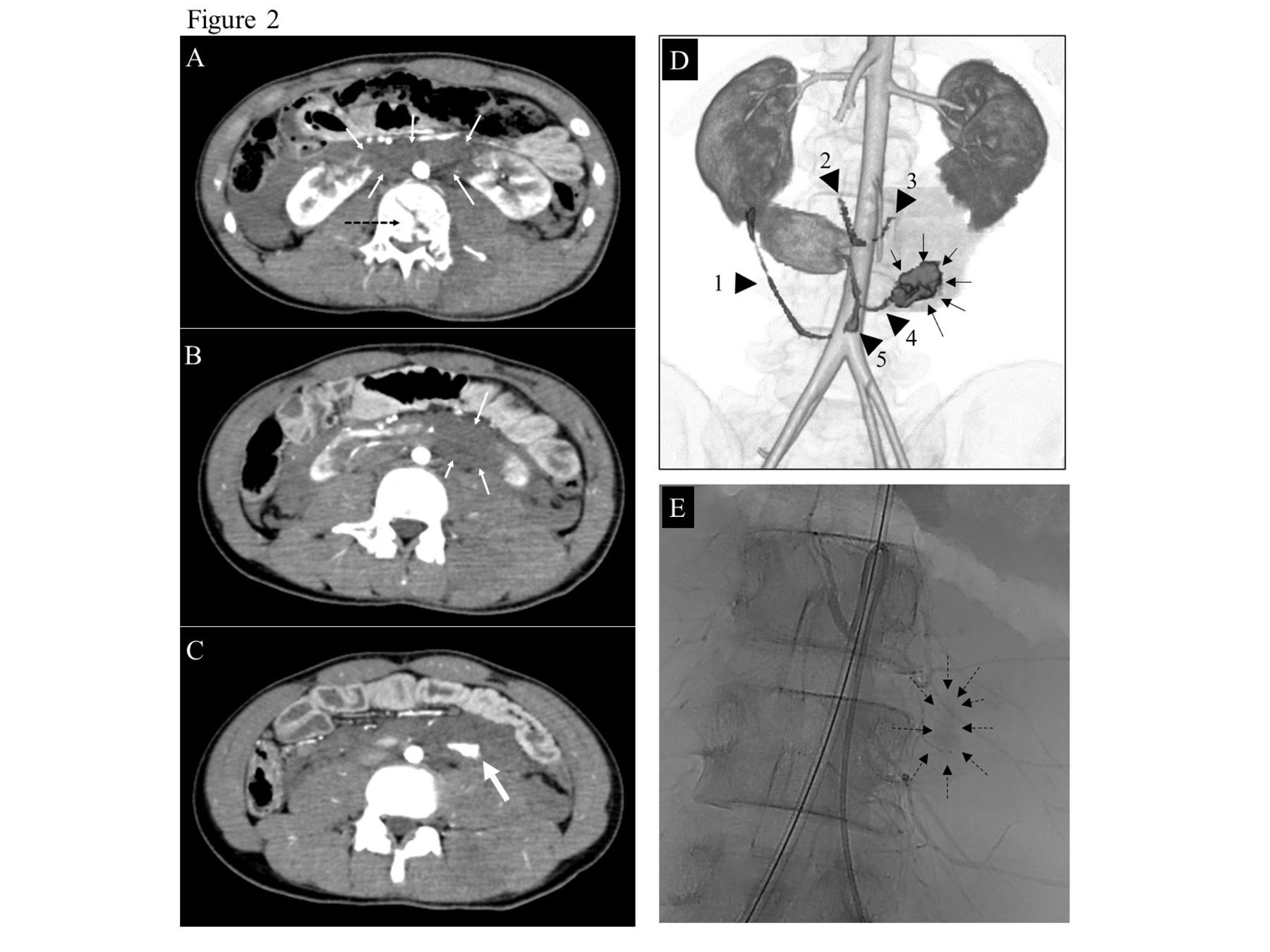
(A–C) Whole-body CT with intravenous contrast agent revealed the HSK injury. The left wing of the HSK and isthmus were not enhanced with the contrast media, which indicated parenchymal ischemia due to the contusion (thin arrows). Extravasation of the contrast agent from the lower pole of the left wing of the HSK surrounded by retroperitoneal hematoma (thick arrow) was evident. The vertebra body behind the isthmus was fractured (dashed arrow). (D) Three-dimensional reconstruction of the CT showed the extravasation of contrast media (thin arrows) that was evident from one of the five aberrant vessels directly arising from the aorta (arrow heads with numbers). (E) Angiography revealed the disruption of a vessel feeding the lower pole of the left wing of the HSK close to the take-off point of the aorta (dashed arrows). HSK, horseshoe kidney.
Additional injuries were seen in right cerebral intraparenchymal hematoma, right pneumothorax, multiple rib fractures, multiple thoracolumbar fractures, pelvic fracture with lumbar spinal cord injury, and left femur fracture (Injury Severity Score 41, Revised Trauma Score 3.57, Trauma Revised Injury Score Probability of Survival 0.27).
What would you do?
Transcatheter arterial embolization (TAE)
Laparotomy and damage control operation
Laparotomy and left heminephrectomy
Inflation of the balloon of the REBOA, simultaneous angiography and damage control operation
What we did and why
After deflation of the balloon of the REBOA, angiography was performed, which revealed that the active extravasation of the contrast agent was very close to the aorta and not amenable to embolization (figure 2E). The balloon of the REBOA was inflated immediately. A midline laparotomy was performed. Although there was a small amount of intraperitoneal hemorrhage, there was a large expanding hematoma in the left retroperitoneum. The left retroperitoneum was opened using the modified Mattox maneuver. Large amount of hematoma was evacuated. A hemorrhage from an artery avulsed from the aorta at the lower pole of the left wing of the HSK was identified and it was ligated. We found that the isthmus was contused with bleeding from the parenchyma (figure 3). It was packed with gauze. After confirming that there was no bleeding from any other site, a temporary abdominal closure was performed. The patient was transferred to the intensive care unit for further resuscitation. The abdomen was closed on postoperative day 3. Because of the spinal cord injury, the patient developed hemiparalysis and was transferred to the rehabilitation hospital after 3 months of hospitalization.

{kind=link}
{kind=link}
{kind=link}
The bleeding artery that was feeding the lower pole of the left wing of the HSK was ligated. There was a contusion of the isthmus, but no disruption. HSK, horseshoe kidney.
Discussion
This patient presented to the hospital with shock due to a massive hemorrhage in the retroperitoneum caused by an HSK injury. It was challenging to diagnose the cause of the shock initially because the eFAST result was negative. The HERS was very useful in this case because we were able to immediately insert the REBOA using fluoroscopy, restore the circulation, and then perform WBCT promptly to diagnose HSK injury. Furthermore, the subsequent angiography and damage control operation could be completed in one room without moving the patient.
HSK is an abnormality that occurs during development and is reported to occur in 1 in 500 patients. This anomalous kidney is likely to be injured by the vertebral body because of the isthmus being anterior to the vertebral body. The most common presentation of this injury is gross hematuria and retroperitoneal bleeding, which leads to hemorrhagic shock. Several vascular variations have been reported, with 40% of cases originating from the common iliac artery, and several cases originating each from the median sacral artery, lumbar artery, internal iliac artery, external iliac artery, and diaphragmatic artery. Arterial supply is often dependent on the arteries to the superior side and the isthmus. Conversely, caudal vessels are less likely to cause ischemia, even after ligation.
If there is significant damage to the parenchyma and the collection system of the HSK, heminephrectomy is necessary. Several reports have shown successful management of HSK injury by TAE, similar to TAE for normal kidney injury.
In conclusion, HSK injury is rare and requires special attention to variants of the feeding vessels. Preoperative radiological imaging is useful for understanding the distribution of blood supply to the HSK. The HERS allows for the use of endovascular procedures as an adjunct to damage control operation. This capability was useful in the management of an HSK injury.
Level of evidence: V
Ethics statements
Patient consent for publication
Ethics approval
This report is approved by the institutional review board of Teikyo University (TUIC-101-19-264). Participants gave informed consent to participate in the study before taking part.
Footnotes
Contributors Conception and design: KI. Acquisition of data: TK, KI. Analysis and interpretation of data: N/A. Drafting of the article: TK. Critical revision of the article: KI, TT, TN, NM. Statistical expertise: N/A. Supervision: NM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.