Article Text

Statistics from Altmetric.com
History
An 18-year-old man presented to the trauma center with a stab wound to the left upper quadrant. His systolic blood pressure during transit was 30 mm Hg palpable.
Examination and first operation
The patient was unresponsive. His systolic blood pressure was still 30 mm Hg palpable, heart rate was 140 beats/minute, and respiratory rate 30 breaths/minute with audible breath sounds bilaterally. Large bore intravenous catheters were inserted as an endotracheal tube was placed, and the patient was moved to the operating room. As a REBOA (resuscitative endovascular occlusion of the aorta) device was not available, a left anterolateral thoracotomy and cross-clamping of the descending thoracic aorta were performed. His heart was empty on palpation, and vigorous resuscitation with crystalloid solutions, packed red blood cells, and pressor medications slowly elevated the systolic blood pressure to 75 mm Hg.
A midline laparotomy was performed, and a massive midline inframesocolic hematoma was noted as were multiple perforations of the jejunum and two perforations of the transverse colon. Dissection through the hematoma exposed a transection of the inferior mesenteric artery and vein, a 95% transection of the infrarenal abdominal aorta, and bleeding from a laceration of the mesentery of the small bowel. The ends of the inferior mesenteric artery and vein were ligated. The abdominal aorta was then reanastomosed using a continuous 3-0 polypropylene suture and buttressed with polytetrafluoroethylene (Teflon) pledgets, the jejunal and colonic perforations were repaired in two layers, and a large mesenteric vein was ligated. A prolonged period of infusion of packed red blood cells, blood products, crystalloid solutions, and epinephrine and dopamine was necessary before the cross-clamp on the descending thoracic aorta could be removed. The abdominal incision was closed using en bloc #2 polypropylene retention sutures. Postoperatively, the patient developed hyperbilirubinemia to 20 mg/dL total, an ileus, and then diarrhea with up to 17 bowel movements per day. In addition, he developed a daily spiking fever to 103°F off antibiotics along with positive blood cultures for Bacteroides fragilis. On the 16th postoperative day, an ultrasound examination of the abdomen showed a pelvic abscess which was drained by reopening the lower half of the midline incision. His spiking temperatures and diarrhea stopped and, after an appropriate course of antibiotics (ampicillin, clindamycin, amikacin), he was afebrile and discharged home on the 26th postoperative day.
Readmission and second operation
Nine days later, the patient returned to the emergency room with a 1-day history of abdominal pain and vomiting. His systolic blood pressure was 60 mm Hg, heart rate was 100 beats/minute, and his stool was guaiac positive. After transfusion of 2 units of packed red blood cells, imaging of the abdomen was positive for free fluid in the left flank and fluid collections in both paracolic gutters. The patient then developed upper gastrointestinal bleeding through his nasogastric tube. Esophagogastroduodenoscopy was performed, but no active bleeding was visualized from the esophagus, stomach, or proximal duodenum; however, there was arterial blood in the distal duodenum. A presumptive diagnosis of an aortoduodenal fistula was made.
After the administration of the same antibiotics used during the first hospitalization, the patient was brought to the operating room. After the midline incision was reopened, 1500 mL of old hematoma was evacuated from the left retroperitoneum. Adhesiolysis was performed until the prior repair of the abdominal aorta was visualized (figure 1). At this point, the repair ruptured, and a large hole in the anterior abdominal aorta was occluded with a finger. An adjacent hole in the posterior duodenum was noted, as well, thus confirming the diagnosis of a secondary aortoduodenal fistula.
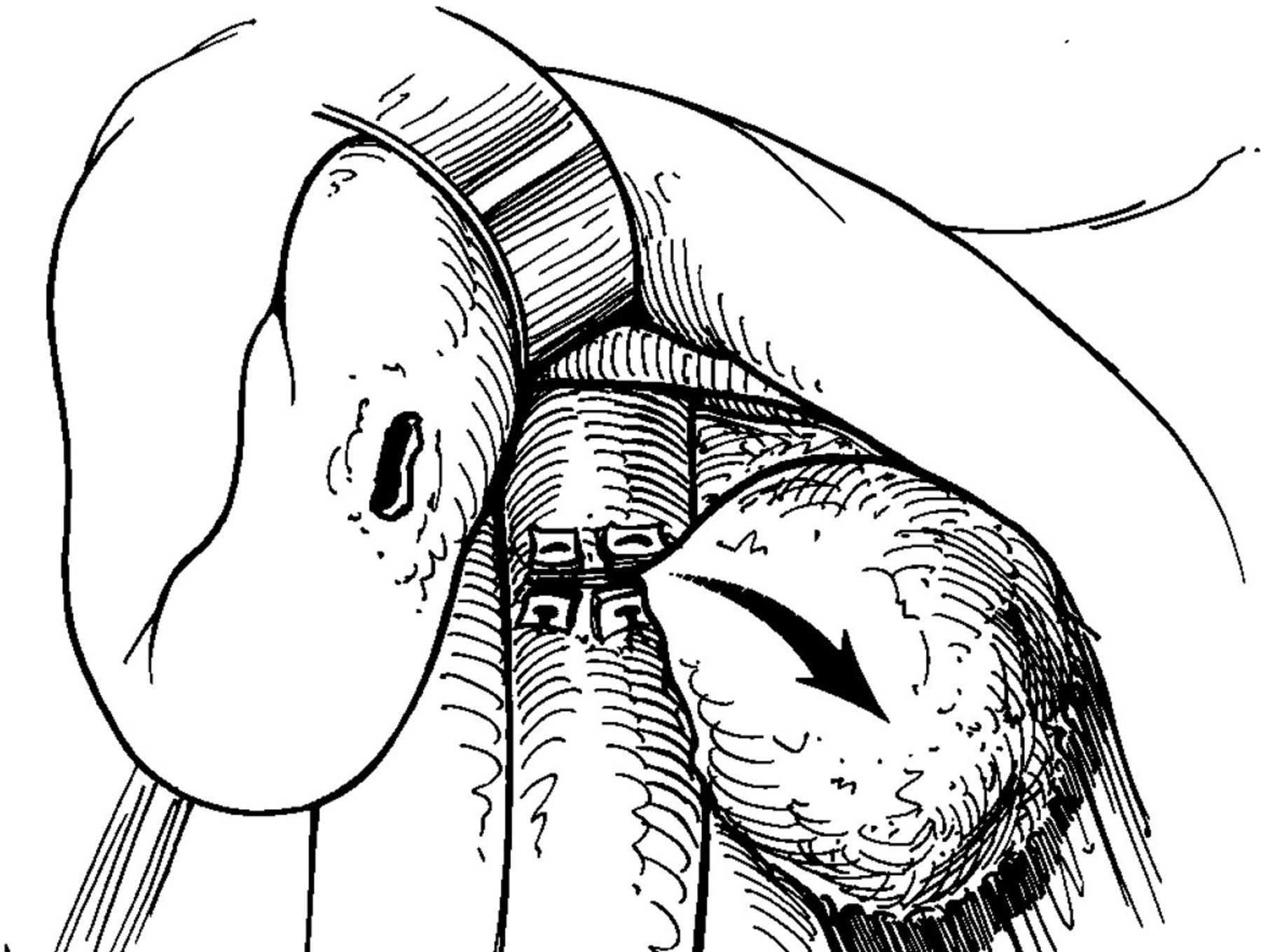
Secondary aortoduodenal fistula from prior primary pledgeted repair of stab wound of the infrarenal abdominal aorta.
Question
Management of the perforation in the abdominal aorta would best be performed by which of the following techniques?
Ligation of the abdominal aorta, insertion of an axillobifemoral graft.
Insertion of an endovascular stent graft to cover the perforation.
Resection of the infrarenal abdominal aorta, insertion of antibiotic impregnated graft.
Patch aortoplasty, cover with a viable omental pedicle, repair duodenum.
Second operation
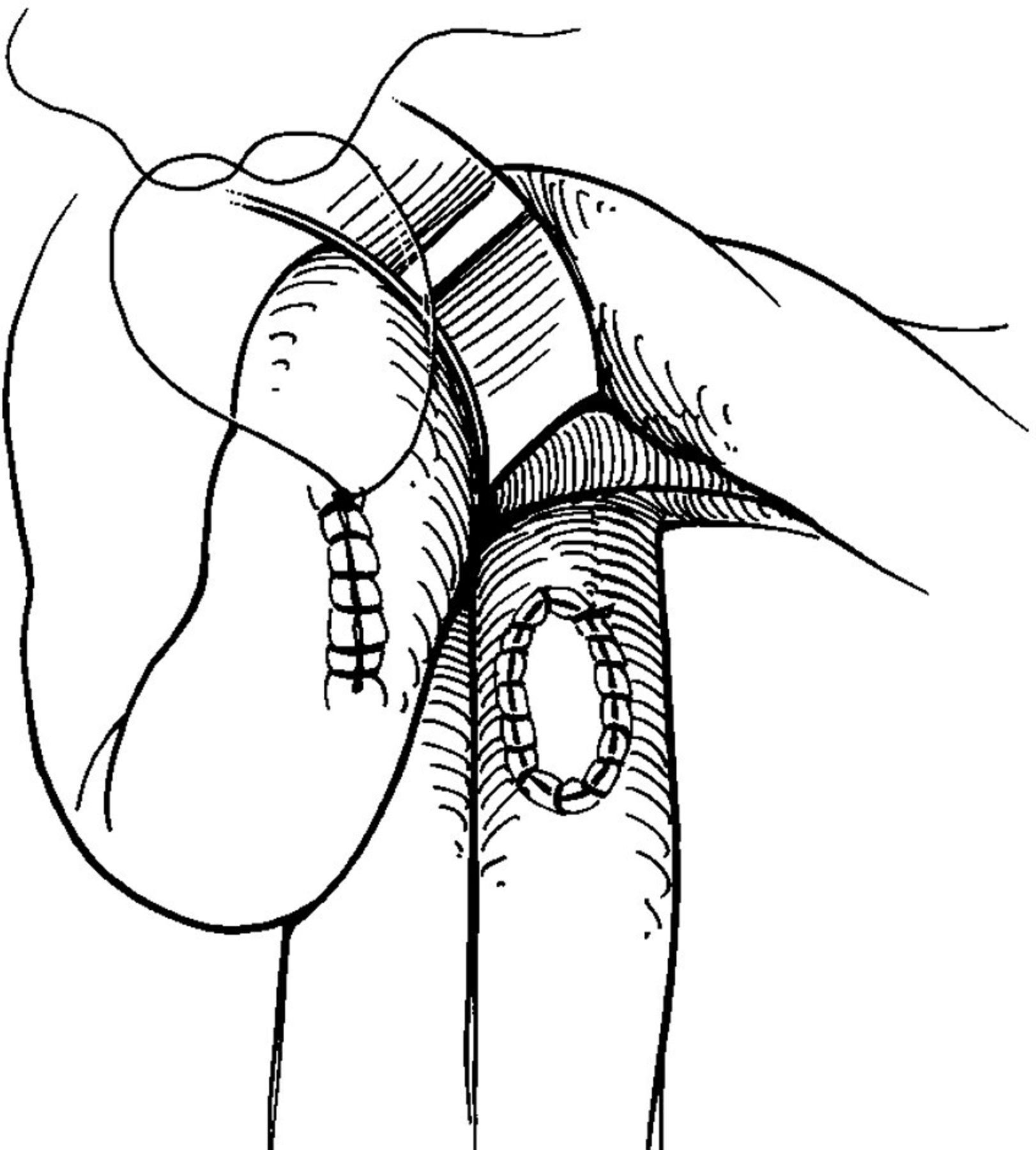
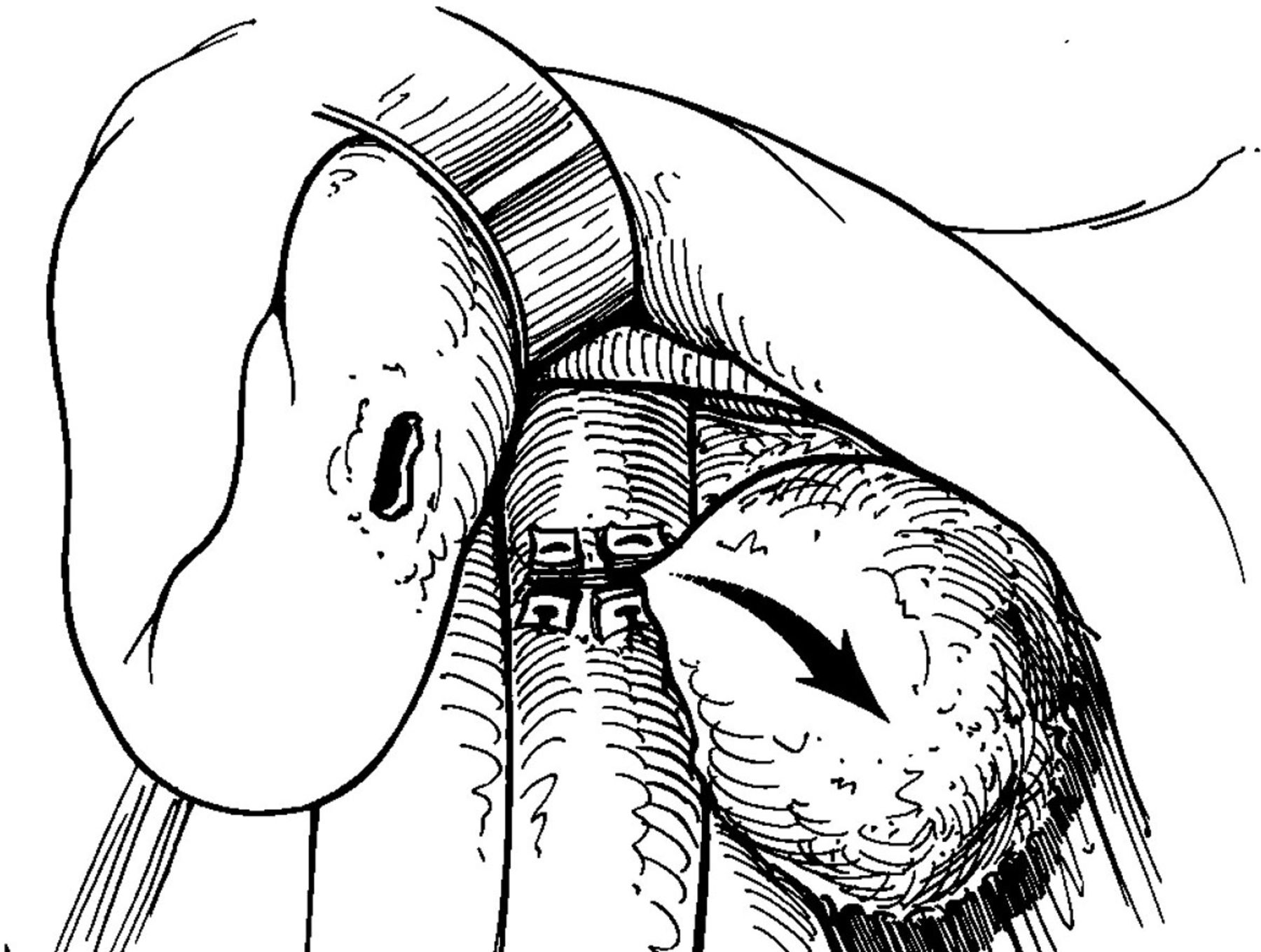
After tedious dissection through dense retroperitoneal scar, aortic cross-clamps were placed proximal and distal to the hole in the anterior infrarenal aorta (figure 2). The sutures and polytetrafluoroethylene (Teflon) pledgets from the original repair were sharply debrided leaving a 2 cm elliptical defect. A polytetrafluoroethylene patch was then sewn to the defect using 4-0 polypropylene sutures (figure 3). Before pulling the final sutures tight, the proximal aortic cross-clamp was removed to allow flushing and then reapplied. The distal aortic cross-clamp was removed to force air out from under the patch and allow for distal flushing. After the final knot was tied, the proximal aortic cross-clamp was gradually removed and bounding pulsations were noted in the distal abdominal aorta and both external iliac vessels.

Proximal aortic cross-clamp applied, and aortic and duodenal defects debrided. Distal aortic cross-clamp not pictured to allow for visualization of defect in aorta.
{kind=link}
{kind=link}
{kind=link}
Polytetrafluoroethylene patch repair of defect in infrarenal abdominal aorta and primary repair of duodenum before pyloric exclusion and gastrojejunostomy.
Management
The most appropriate management for the duodenal perforation in your hands would be:
Segmental resection of the duodenum, end-to-end anastomosis.
Roux-en-Y side-to-end duodenojejunostomy.
Jejunal serosal patch.
Primary repair followed by pyloric exclusion and gastrojejunostomy.
Second operation
After minimal debridement of the edges, the duodenal perforation was repaired in a standard two-layer fashion in a transverse direction (figure 3). A pyloric exclusion was then performed with two rows of 2-0 polypropylene suture through a dependent gastrotomy, and a handsewn antecolic gastrojejunostomy was performed at the site of the gastrotomy in a two-layer fashion, as well. After evacuating more thrombus from the left upper quadrant, the abdomen was vigorously irrigated with multiple liters of saline solution containing bacitracin antibiotic. A viable bulky omental pedicle was then mobilized and tacked in place with absorbable sutures between the aortic and duodenal repairs in the retroperitoneum. After debridement of some necrotic tissue in the midline incision, another en bloc interrupted closure was performed with #2 polypropylene sutures. At the completion of the procedure, bilateral pedal pulses were palpable. Blood replacement during the second operation was 6 units of packed red blood cells and 2 units of fresh frozen plasma.
On the 11th postoperative day, a left psoas abscess was diagnosed on a CT scan of the abdomen and pelvis. Needle aspiration of this was successful based on follow-up CT scans. He was placed on a 6-week course of parenteral antibiotics and then transitioned to lifelong daily oral amoxicillin At the time of discharge on the 51st postoperative day, he was afebrile off antibiotics, eating a general diet, and had normal pedal pulses. He did well for 18 months, but was readmitted with symptoms of biliary tract disease. There were no signs of infection in the aortic graft at that time.
Discussion
The incredibly rare connection developing between an abdominal aortic aneurysm or an untreated traumatic false aneurysm of the abdominal aorta and the retroperitoneal duodenum is known as a primary aortoduodenal fistula.1–4 When such a connection develops between a suture line or prosthetic graft in the abdominal aorta and the duodenum after emergent or elective surgery, this more common entity is known as a secondary aortoduodenal fistula (SADF).
The incidence of SADF after prior elective open insertion of a graft into the infrarenal abdominal aorta (ie, for repair of an abdominal aortic aneurysm or for bypass of occlusion or atherosclerotic narrowing of the aorta and/or common or external iliac arteries) is only approximately 1%.5 The incidence of SADF after primary aortic repair or insertion of a graft into the abdominal aorta after trauma is unknown. This reflects the tiny number of patients who survive after such a graft repair of an abdominal aorta in trauma. The major lesson to be learned from such a rare complication of a vascular repair on a trauma service is that it is mostly preventable.
Patients who have had an open or endovascular repair of an abdominal aortic aneurysm have the wall of the aneurysm interposed between the graft and the adjacent duodenum. In contrast, a patient with a penetrating injury to the abdominal aorta should have a viable omental pedicle mobilized into the retroperitoneum between the suture or graft repair of the vessel and the duodenum and tacked in place with sutures. Although SADFs after elective vascular surgery on the abdominal aorta are not always prevented by the insertion of the omental pedicle, the low incidence suggests that this buttress is mostly effective.
In patients with prior elective operations on the abdominal aorta, the time interval until a SADF develops varies widely, but has averaged 4–6 years in large reviews.5–7 In the trauma patient presented, the SADF developed and mandated a reoperation for upper gastrointestinal, retroperitoneal and intraperitoneal bleeding 36 days after the original repair of the abdominal aorta. This surely reflects incomplete control of the aortic laceration at the original laparotomy, an iatrogenic or missed injury to the duodenum, or both.
Much as the trauma patient described, a patient with a SADF presents classically with signs of infection (fever, chills, failure to thrive), abdominal pain, and gastrointestinal bleeding.5 A ‘sentinel’ upper gastrointestinal bleed is often the manifestation that alerts the surgical team that this unusual complication should be considered. The diagnostic workup involves upper gastrointestinal endoscopy and an abdominal CT with intravenous contrast. On occasion, suspicion of the complication of an SADF may prompt an emergency open exploration and exposure of the whole aortic suture line or graft in the absence of a definitive diagnostic workup.
As noted above, the patient described had patch repair of the defect in the abdominal aorta, primary repair of the duodenum, interposition of a viable omental pedicle between these repairs, and a pyloric exclusion and gastrojejunostomy. Patients with SADF after elective surgery on the abdominal aorta have been managed with a variety of operative procedures during the years. These have included the following: (1) excision of the aortic graft, oversewing of the abdominal aortic stump, axillobifemoral bypass, duodenal repair or resection/anastomosis; (2) excision of the aortic graft, insertion of an in situ antibiotic-impregnated new graft, duodenal repair; (3) injection of a sealant into the fistula, insertion of an endovascular stent graft as a temporizing maneuver in critically ill patients, later replacement of the stent graft and abdominal aorta; and (4) insertion of an endovascular stent graft, lifelong antibiotic therapy in a patient with severe medical comorbidities and a projected limited lifespan.4–13
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.