Article Text

Abstract
Background Older patients living in rural areas face unique challenges after trauma that may hinder optimal recovery. This study aims to qualitatively assess postdischarge challenges in this vulnerable population.
Methods We conducted remote interviews with older trauma survivors in Washington State previously hospitalized in 2019 and residing in rural areas as determined by rural–urban commuting area code. Participants were identified through our institution’s trauma registry and linked with postdischarge data. All eligible participants were contacted. Interview questions focused on needs relating to discharge transition, medical needs, housing, and daily living. Transcribed interviews underwent content analysis to derive a code hierarchy and themes.
Results We conducted 18 interviews out of 83 survivors queried. Compared with non-participants, interviewees had a higher rate of secondary insurance (61% vs 34%), and fewer had an emergency department visit within 1 year (22% vs 34%). Content analysis yielded four major themes: discharge transitions, loss of control, rural insights, and self-efficacy. Most patients felt prepared for discharge and had social support. Regardless of disposition type, most patients needed therapy sessions after discharge. Geography and transportation issues were among the biggest barriers. Most participants were never offered a telemedicine appointment but would have used it if offered. Subthemes of self-efficacy included financial security, leisure, personal outlook, physical and logistical resources, and participants’ support systems.
Discussion Older trauma patients from rural areas face unique challenges after discharge. Key strategies to improve patient experience might include more telemedicine appointments and increased awareness of resources in rural communities.
Level of evidence III.
- multiple trauma
- health care quality, access, and evaluation
- geriatrics
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known
Older adults, a quickly growing segment of the population, are vulnerable to trauma and face unique challenges during and after their care.
What this study adds
Older trauma patients living in rural areas face specific challenges in their discharge transition.
Through qualitative interviews, survivors report loss of control and rural insights in terms of access to care and suggest ways to improve self-efficacy.
How this study might affect research, practice or policy
These findings provide a template for trauma centers to develop postdischarge resources targeting older trauma patients living in rural areas.
Introduction
Older adults, a quickly growing segment of the population, are vulnerable to trauma1 and face unique challenges during and after their care. Older adults are more likely than younger individuals to be hospitalized due to a higher risk of disability and death after injury, and their higher likelihood of comorbid diseases and pre-existing disabilities that prolong the healing and recovery process. Moreover, the normal physiologic changes associated with aging negatively impact how organ systems function during the stress of an acute injury.1 The vulnerability older adults experience related to acute changes in health status, the stressors of hospitalization, and the challenges faced during the recovery period may lead to a decline in health status after hospitalization.2 Due to the unique challenges older adults present after experiencing a traumatic injury, their growing population, and the resulting financial and resource burden on the healthcare system, it is imperative we begin to understand the complex postdischarge needs of older adults.1
Older adults living in rural areas face even more challenges after discharge for traumatic injuries. Some of these factors may include socioeconomic needs magnified by illness and disability, and challenges with accessing rural healthcare and post-trauma or burn follow-up care. Compared with urban areas, rural areas tend to have a higher prevalence of older adults and poorer health, demonstrated by a higher prevalence of obesity, chronic diseases, depression, and decreased social functioning.3 Rural areas have fewer rehabilitation resources, including physiatrists, rehabilitation therapists, and mental health providers, when compared with urban areas.4 Although rural adults are at an elevated risk of traumatic injury when compared with adults in urban communities,5 there is limited research on the barriers that adults from rural areas face after hospitalization for traumatic or burn-related injuries. Most of the existing literature on rural trauma patients is quantitative and focuses on mortality and rehospitalization. We have chosen a qualitative research strategy to better understand the lived experiences of older adults from rural communities hospitalized with trauma.6 Indepth interviews may fill the gap in knowledge and enable strategies to maximize recovery from trauma for older adults living in rural communities.
The primary aim of this study is to assess and comprehend difficulties and barriers experienced by older adult trauma patients living in rural areas after hospitalization. This will help to inform quality improvement and improve the discharge planning process at state-designated level 1 trauma and regional burn center.
Methods
Study design and population
We conducted a cross-sectional, qualitative study. The research and survey were based at Harborview Medical Center (HMC). This institution serves as Washington State’s designated level 1 trauma center and also receives referrals from Idaho, Montana, and Alaska for trauma and complex surgical problems. It is also a regional burn center and altogether constitutes approximately 6000 injury admissions per year. HMC is a 413-bed safety-net hospital owned by King County and operated by the University of Washington (UW).
Interview development
The Knowledge to Action (KTA) framework informed this project and was used to guide a postdischarge needs assessment of older adults living in rural areas who were admitted to HMC after a burn or traumatic injury. The KTA framework is a dynamic process that includes knowledge creation and knowledge application with the overarching goal of improving health and healthcare.7 Furthermore, it allows the user to focus on the needs of the project and tailor interventions to meet agency-specific needs.7
We developed the patient interview guide using information synthesized in a literature review as well as questions taken from instruments and survey tools previously validated in the literature on postdischarge transitions.2 Survey questions were either multiple choice or open-ended and focused primarily on patient-reported needs related to housing, discharge, transition to home from the hospital, social support, and basic needs of daily living. Two authors (LN, TP) used an iterative process to develop and vet the questions. We ensured that the questions had an appropriate balance to query about transitional care challenges and living situation after injury. The interview guide was approved by both the UW faculty and agency contacts and the UW Institutional Review Board.
Data acquisition and interview protocol
First, we obtained patient and injury data from the hospital’s trauma registry for 2019 and then linked individual patient data to postdischarge data through the hospital’s quality improvement team. Patients who died within 1 year of admission were excluded. We then categorized the remaining patients by rural–urban commuting area (RUCA) index and restricted our sample to rural codes (RUCA 7, 8, and 10). From the final cohort of potential participants, we stratified age, sex, and injury mechanism and chose participants at random from each category to ensure a representative group (figure 1). Due to recruitment difficulty (many declined participation and others did not respond), we eventually contacted all eligible patients to obtain a sufficient sample size. We had aimed to enroll 20 patients as a final participant group of older adults who live in rural areas and are recovering from their traumatic injuries. To assess the representativeness of our sample, we obtained injury, patient, and clinical outcome characteristics for both participants and non-participants after merging our health system’s data with the state-wide death, trauma, and emergency use registries.

Flow diagram of participant selection. RUCA, rural–urban commuting area.
Indepth interviews were administered from December 2020 through January 2021. Participants were approached if they were discharged from HMC after burn or trauma in 2019, were at least 65 years of age, and were classified by zip code on file in the electronic medical record as living in a rural area as determined by the RUCA code. A research team member contacted each potential participant and provided a detailed overview of the study to include the need to record study interviews. Participants were offered interviews remotely by phone or Zoom videoconferencing (San Jose, CA). Patients were provided with categories of questions they would be asked if they consented. Participants were thanked but not compensated for their time.
Data analyses
Interviews were audio-recorded and then all questions were recorded, transcribed, coded, and analyzed using content analysis. Demographic data were analyzed using descriptive statistics. Recorded interview segments were transcribed verbatim and coded using Dedoose (Los Angeles, CA), an online software compliant with the Health Insurance Portability and Accountability Act (HIPAA). For the open-ended questions, two researchers (LN, TP) independently coded individual responses into similar ideas, concepts, or attitudes. The codes were then curated and condensed to derive key themes using an inductive strategy. Throughout this process, coders met weekly to discuss the process, development of the codebook, consistency in code application, and thematic code development.
Results
Participant characteristics
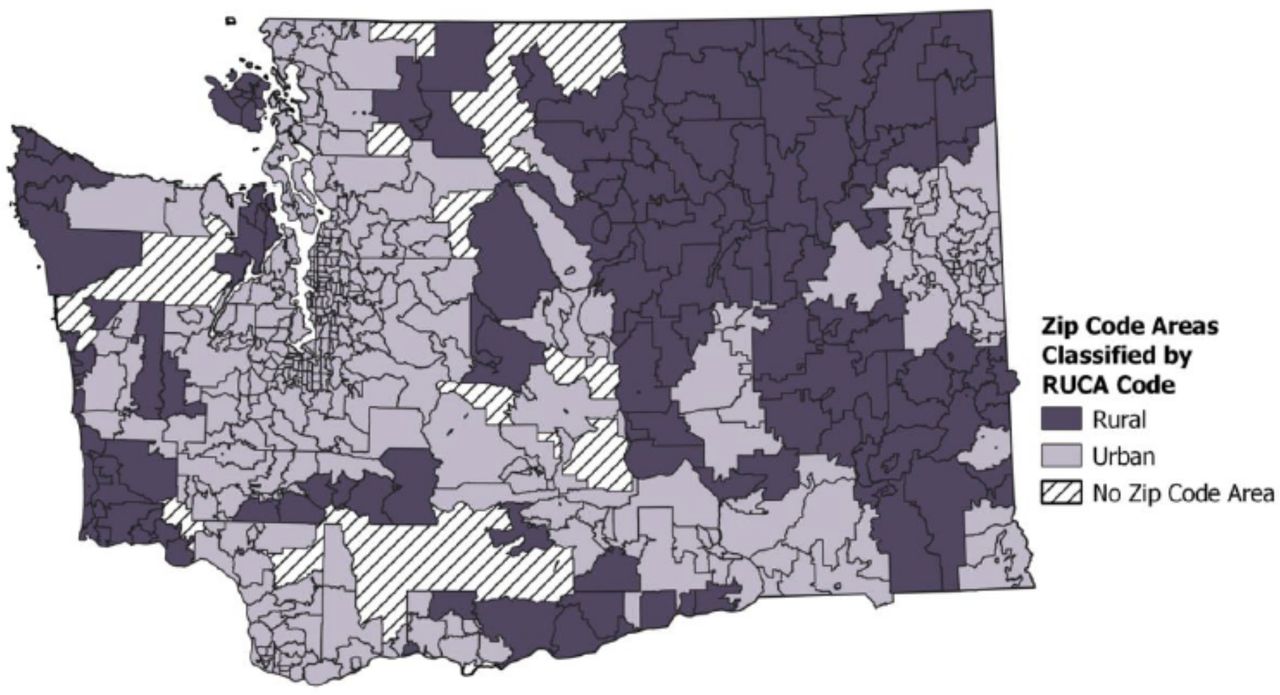
We ultimately contacted all 83 eligible survivors who fit the study inclusion criteria to be able to enroll 18 patients (21.7% participation rate) for interview. Our study sample consisted of 8 men and 10 women. Ten participants (56%) were 65 to 74 years old, seven (39%) were between ages 75 and 84, and one (5.5%) was aged 85 years. Sixteen patients identified themselves as white, one patient self-identified as white, Native American, and black, and one patient declined to answer. Ten participants (55.5%) lived in an area with RUCA code 7 or 8, and eight (44.5%) lived in an area with RUCA code 10 (figure 2). Sixteen participants (89%) used Medicare as primary insurance and 11 participants (61%) used commercial insurance for their secondary form of insurance. Four participants (22%) had an emergency department visit within a year after injury (table 1).
{kind=link}
{kind=link}
Washington zip code areas by RUCA code. RUCA, rural–urban commuting area.
Demographics of participating trauma patients
In contrast, 35 non-participants (54%) were aged 65 to 74 years, 18 (28%) were between ages 75 and 84, and 12 (18%) were aged 85 and older. Three individuals (4.6%) who declined participation were classified as Hispanic per the trauma registration. Fifty-seven (88%) non-participants used Medicare as their primary insurance, but only 22 (34%) non-participants had secondary commercial insurance. Twenty-two non-participants (34%) had an emergency department visit within 1 year (table 1).
Survey results
Participants reported variable experiences on returning home to their rural communities, but almost all reported having everything they needed to care for themselves at home. Four major themes were identified from qualitative analysis: discharge and care transition, loss of control, rural insights, and self-efficacy. Table 2 provides illustrative quotes for each of the four categories and subthemes. Discharge and care transition included the tools and education provided for patients at discharge, the equipment needed for recovery at home, the accessibility of telemedicine, and access to primary care providers, physical therapy (PT), and occupational therapy (OT). Assistance at home included a lift and housekeeping help. Home assistive devices included walkers, canes, shower chairs, or grab bars. Three patients needed restrictive devices on discharge (neck brace, arm sling), and one needed wound care supplies. Only two participants did not need any equipment or supplies after discharge. One key challenge for participants was accessing PT and OT after transitioning home. The majority of participants were recommended to continue PT or OT after discharge either at a skilled nursing facility, inpatient rehabilitation, or as an outpatient. In particular, PT is frequently used for recovery from falls, making it a common and important resource for older adults. However, two patients were unable to attend their recommended PT/OT, one because the patient was unable to pay for the therapy out of pocket or for the gas it would take to get there, and another because the patient was unable to travel the distance required. In terms of access to trauma center resources postdischarge, participants reported that telemedicine services were highly desirable. However, 13 participants reported never being offered a telemedicine appointment, and over half of the participants (10; 56%) reported feeling as though they would be able to successfully use telemedicine if it was offered. The majority of participants felt prepared to care for themselves on discharge. Two participants felt only somewhat prepared, whereas two did not feel that they were prepared at all. Many participants were supported by their families after discharge and the majority felt that they had quite a lot of emotional help and support from their family. Eleven participants lived with a spouse or significant other, and only four lived alone.
Illustrative participant quotes
Patients’ sense of loss of control centered primarily around their life changes resulting from their injury, their level of pain, and the COVID-19 pandemic. Many patients had to adjust to life with their injuries and were unable to do all the things they were able to do prior, such as driving a car. The COVID-19 pandemic caused multiple patients to discontinue their prescribed PT prematurely, potentially affecting their injury outcomes.
Participants were able to provide insights on the challenges living in rural communities, including difficulty finding a primary care provider, geography, and transportation issues. Five participants did not have access to a car or were unable to drive at all. Patients also highlighted the benefits of living in rural areas, such as the increased sense of community. Despite living in communities that had fewer resources than urban areas, there was an increase in shared resources, including programs that provided people with used medical devices such as walkers and commodes to be returned to the program after use.
Subthemes of self-efficacy include financial security, leisure, personal outlook on life, physical and logistical resources, and participants’ support systems. No patients reported needing to choose between paying for food or medication after discharge, although one noted that he previously had to make those choices.
Discussion
In this study we queried trauma and burn patients about their experience after injury, social support, and challenges specific to living in a rural area. We chose to implement indepth interviews as a research strategy in an effort to better understand the lived experiences of adult trauma patients during and after hospitalization.6 Although each patient’s experience was unique, almost all patients queried had the support and resources they needed for inhome care. Participants consistently highlighted the importance of assistive devices and therapy services in their recovery, as well as the positive impact of community resources such as loaner assistive equipment. The majority of participants reported a strong sense of community living in a rural area, a stable support system, and in general were able to meet their basic needs. However, a common experience for participants was the need for increased support with accessing PT and OT. Barriers to care varied but included expense, distance, and access to local and trauma center resources.
Resources in rural communities are reduced when compared with urban communities, and the majority of high-risk trauma patients living in rural areas are often not treated in major trauma centers.8 Rural areas have lower density of providers, including general surgeons, and other subspecialty providers.9 It is not uncommon for residents to not seek out necessary healthcare in their rural communities due to financial barriers, distrust that physicians had been adequately trained, or a lack of transportation.10 There are higher rates of mortality in rural areas, and the disparity between rural and urban age-adjusted mortality rates tripled between 1999 and 2019.11 A partial solution to address the disparity in healthcare in rural communities is the implementation of telehealth. Telehealth can provide broader resources to communities that would otherwise not have those options and allows providers to more effectively care for their patients.12 The majority of study participants were not offered telehealth appointments on discharge, but felt that they would be able to navigate telehealth if given the opportunity.
There are important limitations to these findings. Due to high rates of refusal or non-contact, we contacted all eligible survivors to arrive to a sample size of 18 participants. The participants who agreed to be interviewed may not be representative of the larger eligible cohort. Our methodology likely favored the subset of patients in better social, economic, and physical recovery. With respect to socioeconomic challenges, this cohort of participants faced fewer challenges than expected as they all had a current source of income and form of transportation, no one had to move their home location after discharge, and no participant had to choose between paying for medication or other needs. As an example, more participants had secondary insurance when compared with non-participants. This indicates that participants were more financially secure on average, as they were able to prepare for the potential of injury with insurance. More non-participants had an emergency department visit within 1 year of discharge, which may be related to access to PT, follow-up care, or stable housing. Our participants came from a single level 1 trauma center, so their challenges may not accurately represent or fully encapsulate the challenges faced by others in rural communities.
Additionally, the COVID-19 pandemic added challenges to both participants and researchers, making data collection more difficult. All interviews had to be conducted remotely. The high non-contact and refusal rate may highlight the difficulty in conducting research remotely with older survivors.
Conclusion
This project provides insights into the lived experience of older adults returning home to a rural area after hospitalization for traumatic injury. Discharge experience varied, but nearly all participants reported some difficulty when transitioning back into their rural communities. There is room for improvement in the discharge and care planning process for older adult patients from rural communities, who face a unique set of challenges. Trauma centers should increase their awareness of community resources in specific rural areas they serve. Actionable recommendations on discharge include the following: set up the option to be seen via telemedicine and ensure patients have the knowledge to use this option, arrange specific follow-up appointments with each patient’s primary care provider, and set up referrals to local PT/OT programs. By incorporating these recommendations, trauma centers may be able to facilitate patients’ access to the proper resources to successfully transition home and increase the likelihood of returning to baseline functional status.
Supplemental material
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the University of Washington Institutional Review Board (study number 00011654). Participants gave informed consent to participate in the study before taking part.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at The paper has been presented at the American College of Surgeons, Chelan, Washington in September 2021.
Contributors LN, MJR, EG, JS, and TP designed the study. LN recruited the patients and conducted the interviews. LN, TP, and ERD analyzed the data. ERD drafted the article and all authors participated in the critical revisions of the article. TP acted as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.