Article Text

Abstract
Objectives Recreational off-road vehicle crashes can produce severe injury and death among children, often from head trauma sustained while riding unhelmeted. Although required for competition, recreational riders commonly forego helmets. This study aimed to identify socioeconomic factors associated with unhelmeted injuries among children riding all-terrain vehicles (ATVs) and dirt bikes recreationally, thus informing injury prevention efforts.
Methods A retrospective review was completed of patients younger than 18 years who presented after recreational ATV or dirt bike crash to a single American College of Surgeons-verified level 1 pediatric trauma center (2010–2019). Demographic, injury, and outcome data were collected. US Census data regarding median and per capita income, poverty prevalence, and scholastic graduation rates were recorded for each patient’s home county. Relationships between helmet use at the time of injury, demographics, and socioeconomic variables were examined.
Results The cohort comprised 680 injured recreational ATV (n=510; 75%) and dirt bike (170; 25%) riders. Unhelmeted riders (n=450) were significantly older (median age 13 vs 11 years; p=0.008) and more often rode ATVs (n=399). Significantly greater percentages of females (77.9%; p<0.001) and passengers (89.5%; p<0.001) were unhelmeted at the time of injury. Residents of counties with lower median and per capita income, higher poverty prevalence, and lower high school and college graduation rates were significantly more likely to be unhelmeted at the time of their crash (p=0.003). In multivariable analysis, unhelmeted injuries were independently associated with ATV use (OR=6.757; p<0.0001), passenger status (OR=6.457; p<0.0001), and older age (OR=1.219; p<0.0001).
Conclusion In children, ATV use, passenger status, and older age associated independently with unhelmeted riding in recreational vehicle crash. Residence in a county with both lower median income and scholastic graduation rates associated with unhelmeted crashes, and lower median income significantly predicted unhelmeted crashes. This study revealed socioeconomic factors that identify communities with greatest need for injury prevention initiatives.
Level of evidence III—retrospective comparative epidemiological study.
- accident prevention
- socioeconomic factors
- pediatrics
- head injuries, closed
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Although helmets have been shown to reduce morbidity and mortality resulting from all-terrain vehicles (ATVs) and dirt bike crashes, unhelmeted riding remains a persistent issue among children and teenagers, with up to 80% neglecting to wear a helmet.
Factors reported to increase a child’s likelihood of riding without a helmet include female sex, adolescent age, riding as a passenger, and riding a larger ATV than recommended for a child’s size.
What this study adds
In addition to clarifying individual factors that increase a child’s likelihood of experiencing an unhelmeted crash, this study is the first to identify specific socioeconomic factors that place a child at greater risk for experiencing an unhelmeted crash.
How this study might affect research, practice or policy
We hope these findings can better tailor and target injury prevention outreach programs focused on helmet use and safe riding practices for recreational ATVs and dirt bike riders living in high-risk counties.
Background
Off-road motorized vehicles—specifically all-terrain vehicles (ATVs) and dirt bikes—pose significant safety risks to children, especially when ridden without a helmet.1–5 The most recent US Consumer Product Safety Commission report on off-road motorized vehicles identified from 2015 to 2019 over 524 600 emergency department-treated injuries and 2258 deaths in the USA for all ages.4 Of these, disproportionately higher fatalities were reported in children aged 12–15 years when compared with their population representation.4 Risky riding practices—such as riding without a helmet, with passengers, and on paved roads—are widespread, particularly in children and adolescents.5–8
Although helmets have been shown to reduce morbidity and mortality resulting from off-road motorized vehicle crashes,1–3 9 unhelmeted riding remains a persistent issue among children and teenagers, with up to 80% neglecting to wear a helmet.3 5 6 10–12 Factors reported to increase a child’s likelihood of riding without a helmet include female sex, adolescent age, riding as a passenger, and riding a larger ATV than recommended for a child’s size.5 6 13–17 Furthermore, one study found that individuals who have been injured in a prior off-road vehicle crash were still less likely to wear a helmet in the future,18 suggesting that high-risk behaviors are engrained and difficult to change.19
Despite previous efforts to promote safe riding practices through professional society statements, policy,20–22 and education initiatives,7 23–25 little change in crash incidence or helmet use among children who ride ATVs and dirt bikes over the past decade has been realized.8 26–29 The economic impact of these injuries on individual families as well as the medical system is significant in terms of financial cost as well as future years of work lost due to morbidity.27 30–32 Moreover, our group recently reported increased consumption of neurosurgical resources among unhelmeted riders of off-road recreational vehicles.33
The myriad factors influencing a child’s likelihood to be injured while riding an ATV without a helmet can be organized using an epidemiological triangle approach that includes host, agent, and environmental factors.15 The physical environment is readily apparent, encompassing factors such as road surface, weather, and terrain. By contrast, a child’s social environment is less visible but equally—if not more—important to consider.16 24 34–36 This study, therefore, aimed to identify socioeconomic factors associated with unhelmeted crashes among children riding ATVs and dirt bikes in a recreational setting, thus informing future injury prevention efforts. We hypothesized that children living in communities with lower measures of socioeconomic status would be at greater risk to sustain an unhelmeted crash.
Methods
Study design and cohort
A retrospective study was conducted of all patients younger than 18 years who presented to a single American College of Surgeons (ACS)-verified level 1 pediatric trauma center and were evaluated by the pediatric trauma surgery team between January 1, 2010 and December 31, 2019, following an ATV or dirt bike crash.37 38 Per our institutional standard of practice, patients older than 15 years of age who present as a level I trauma are triaged to the adult hospital, whereas patients 16 and 17 years of age who present as level II or III trauma are triaged to the children’s hospital; however, no strict age-based exclusion criteria were applied for the purpose of this study. Because helmets are required in a competitive setting for both ATVs and dirt bikes, patients were excluded if the crash occurred in an organized competition (n=70) or if helmet status at the time of crash could not be determined (n=18; figure 1). The data accession and storage were performed in accordance with the Health Insurance Portability and Accountability Act in a secure REDCap database.39 Equator Network Strengthening the Reporting of Observational Studies in Epidemiology guidelines were followed as appropriate for this retrospective study.40
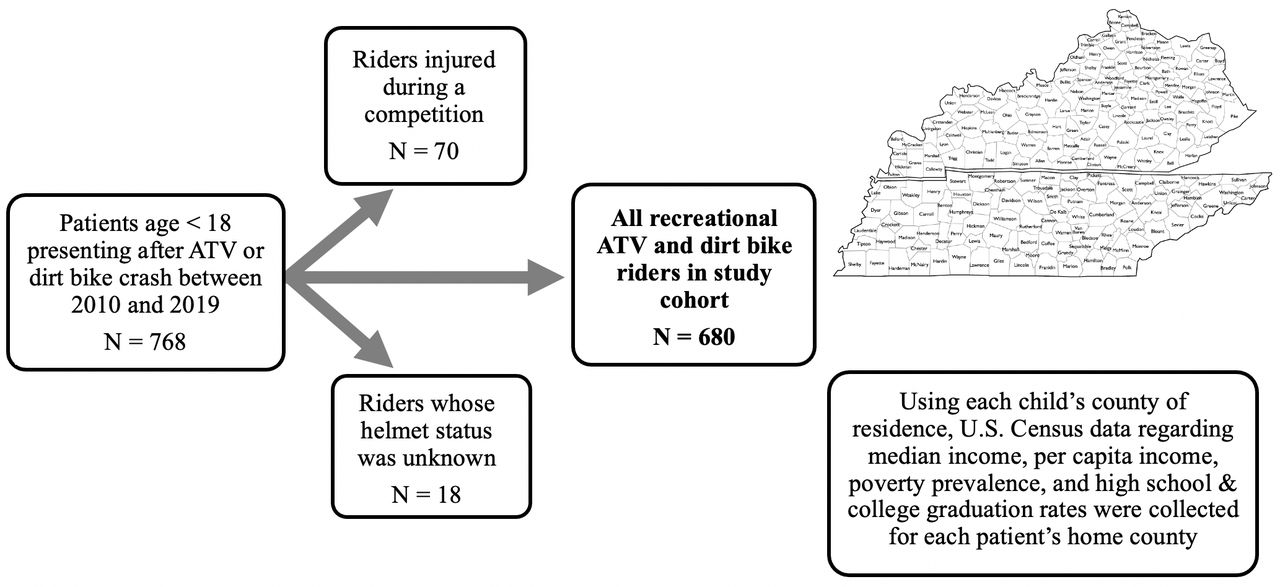
Schematic of study cohort selection. Patients were initially identified using an institutional trauma registry, and clinical data were collected using retrospective review of the electronic medical record. ATV, all-terrain vehicle.
Data collection and crash variables of interest
Patient data retrieved from the institutional trauma database included demographics such as age, sex, race, home county, and injury county. Patient records were then reviewed manually to extract additional injury and outcome data, and all extracted data were stored securely using a REDCap database. Variables of interest included patient mechanism of injury (rollover, crash on jump, ejection, collision with solid structure, collision with other vehicle), location of crash (home/yard, street, farm/field, or racetrack), driver status (passenger or driver), vehicle type (ATV or dirt bike), intubation prior to hospital arrival, Glasgow Coma Scale (GCS), and Injury Severity Score (ISS) on admission. Helmet status was classified as either helmeted or unhelmeted, determined by review of first responder documentation as well as clinical and social work notes.
Socioeconomic variables
To evaluate socioeconomic factors influencing helmet use in children, US Census data regarding median income, per capita income, poverty prevalence, as well as high school and college graduation rates were collected for each patient’s home county. From the institutional trauma registry containing each child’s county of residence, a list of all counties was made, and the US Census database was queried to obtain the aforementioned socioeconomic variables for each county.41
Statistical analysis
Relationships between helmet use, rider demographics, and home county socioeconomic measures were examined using univariate and multivariable statistical analyses. Categorical variables are presented as frequency and proportion. Continuous variables are presented as mean (±SD), except in the case of non-normal distributions, which are presented as median (IQR). Statistical significance for continuous variables was calculated using non-parametric, Mann-Whitney U tests or one-way analysis of variance with a significance level of p<0.05. Categorical variables were analyzed with a χ2 or Fisher’s exact test with a significance level of p<0.05.
Results
Demographics and crash profile
Overall, 680 patients (510 ATVs and 170 dirt bikes) were evaluated for injury. The cohort was predmoninantly male (n=485, 71.3%) and racially self-identified as white (n=633, 92.8%). The majority of riders were unhelmeted at the time of their crash (n=450, 66.2%). Unhelmeted riders were significantly older (median age 13 (IQR: 9.0–14) vs 11 (IQR: 8.0–14) years; p=0.008) and more often rode ATVs (n=399, 88.7%; p<0.001). Females had a higher prevalence of unhelmeted riding at the time of injury compared with males (77.9% vs 61.4%; p<0.001). Most passengers rode without a helmet (89.5%), accounting for 41.8% of the unhelmeted group but only 9.6% of the helmeted group (p<0.001). Additionally, unhelmeted riders disproportionately required helicopter transportation to the hospital compared with the helmeted group (40.0% vs 27.8%; p=0.004). No difference in race or ethnicity between helmeted and unhelmeted riders was detected. Furthermore, no difference in location of crash (home/yard, street, farm/field) was observed between groups nor in proportion of patients who came directly from the scene of the crash as opposed to transferring from an outside hospital. Insurance type (private, public, military, self-pay) did not differ significantly according to helmet use (table 1).
Demographics and crash profile
Injury characteristics and clinical outcomes
Unhelmeted riders were more often intubated before hospital arrival (5.1% vs 1.3%; p=0.014) and more frequently admitted to the pediatric intensive care unit from the emergency department (19.8% vs 9.60%; p<0.001). Unhelmeted riders had a higher mean ISS compared with helmeted riders (11.1 vs 9.45; p=0.047). Although injuries in the unhelmeted group tended to be more severe as measured by ISS, no significant difference in overall incidence of solid organ injury or in individual solid organ injury patterns between groups emerged. A greater proportion of patients in the unhelmeted group had a GCS of 8 or lower compared with the helmeted group at presentation (5.8% vs 1.7%, p=0.015). Furthermore, a greater proportion of unhelmeted riders suffered skull fractures (17.8% vs 4.3%; p<0.001) and intracranial hemorrhages (16.2% vs 3.9%; p<0.001) compared with the helmeted group. As recently reported by our neurosurgical colleagues, neurosurgical consultation was required for 118 unhelmeted riders (26.2%) but only 21 helmeted riders (9.1%) (p<0.001); neurosurgical intervention was required for 12 unhelmeted riders (2.7%) and only 1 helmeted rider (0.4%) (p=0.040) in this cohort33 (table 2).
Injury characteristics and clinical outcomes
Socioeconomic features of home county
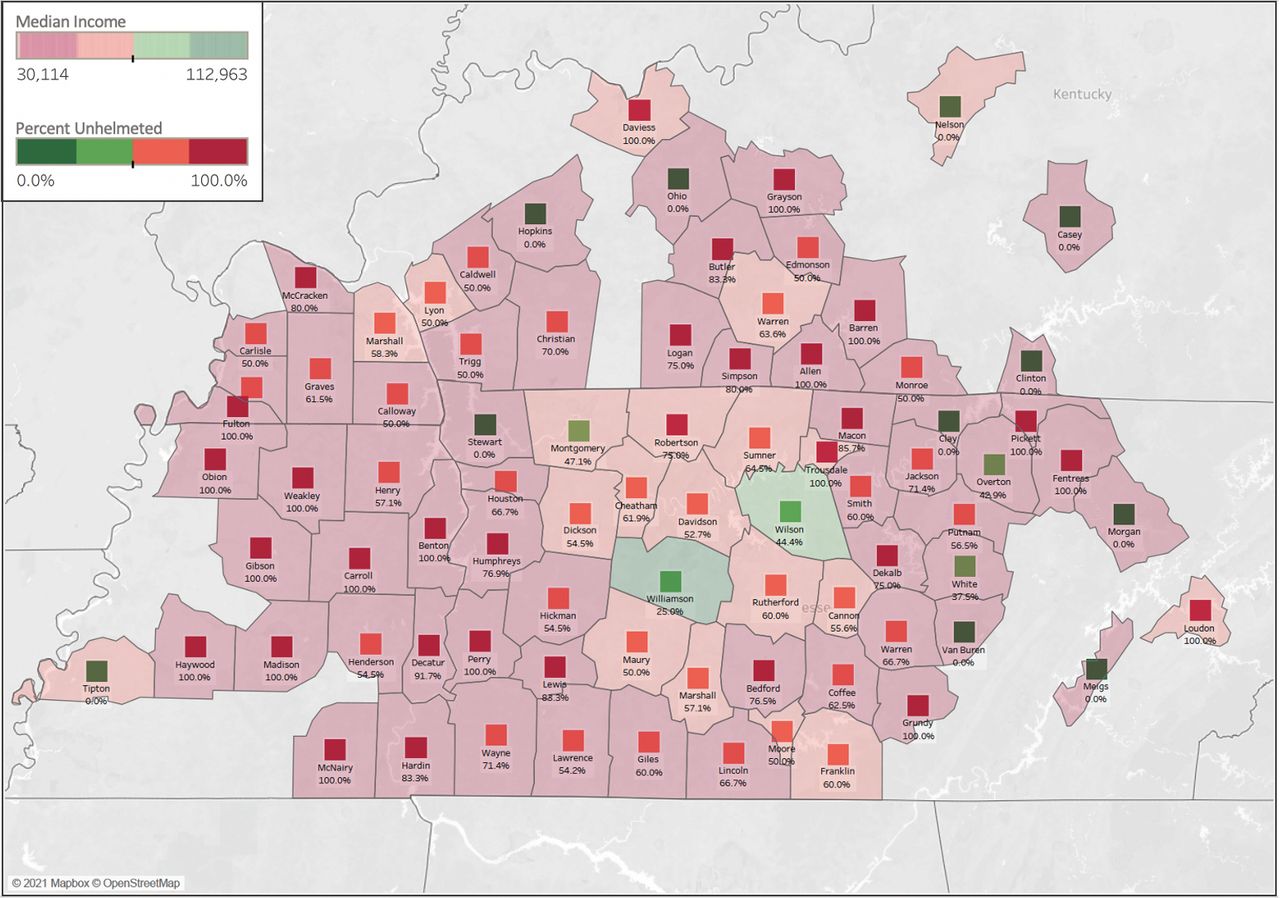
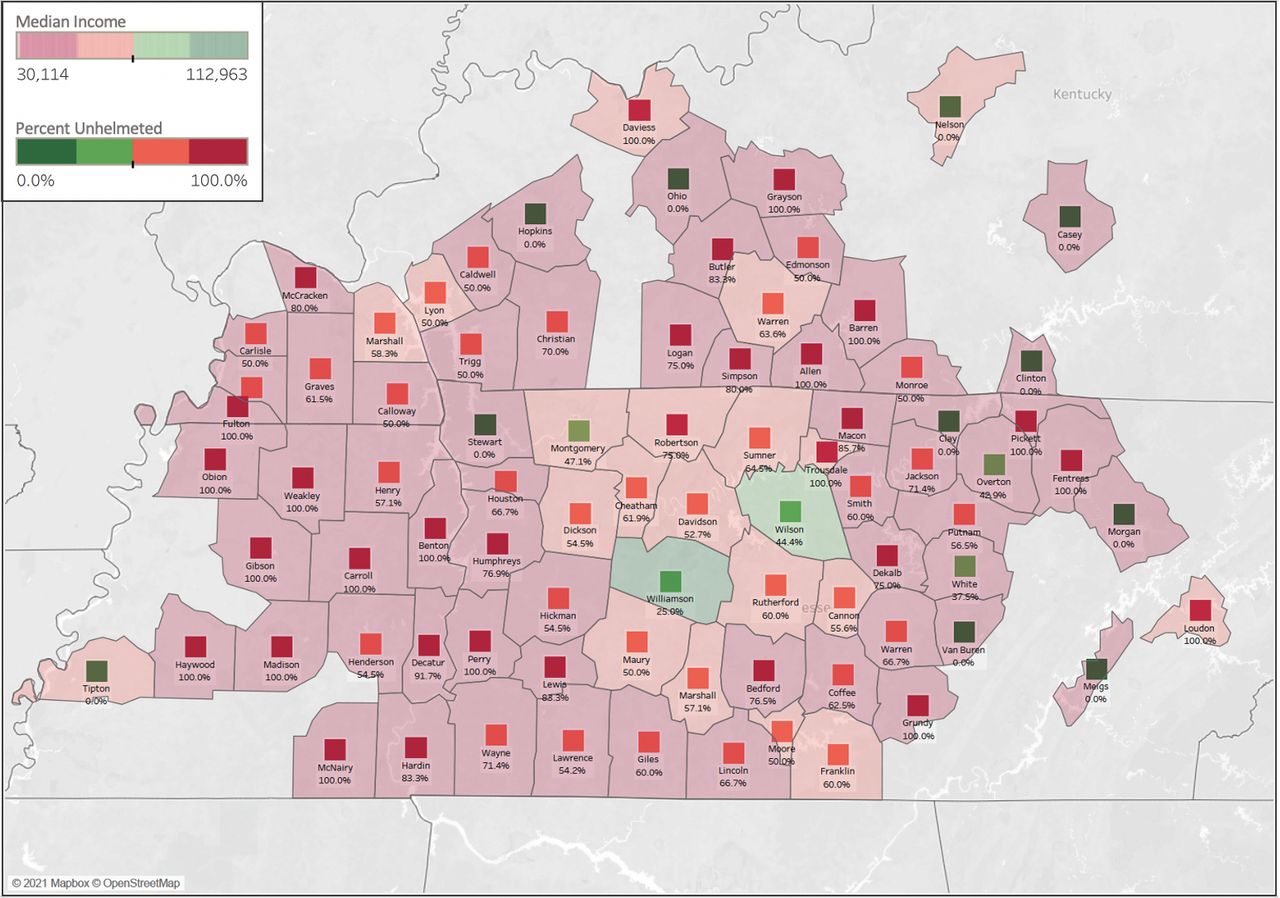
Regarding socioeconomic variables, the average home county median income was significantly lower for children who rode unhelmeted compared with those who wore a helmet at the time of their crash (US$52 111 vs US$57 029; p<0.001). Mean per capita income was also lower for children who rode unhelmeted compared with children who rode with a helmet (US$27 252 vs US$29 248; p=0.003). Conversely, the mean per cent of individuals living below the poverty line in one’s home county was higher among the unhelmeted riders compared with helmeted (13.9% vs 12.8%, p=0.001). Finally, high school graduation rate of home county was lower for the unhelmeted group compared with the helmeted group (85.8% vs 87.0%; p=0.002), as was college graduation rate (21.6% vs 25.7%; p<0.001). Interestingly, no significant difference in insurance type between the two groups emerged (figure 2, table 3).
{kind=link}
{kind=link}
By county in Tennessee and Kentucky, median income and percentage of crashes occurring without a helmet. Counties are shaded by median income, with red representing low income and green representing high income. Per cent unhelmeted is shown in the box overlying each county, with red representing ≥75% unhelmeted and green representing ≤25% unhelmeted.
Socioeconomic features of home county
Multivariable analysis
In multivariable analysis, unhelmeted riding was predicted by ATV use (OR=6.757; p<0.001), riding as a passenger (OR=6.457; p<0.001), and older age (OR=1.219; p<0.001). Lower median income of home county predicted unhelmeted riding at the time of crash (p=0.009), with a decrease in median income from the 75th to 25th percentile making unhelmeted riding 1.4 times more likely. In other words, a child living in a county with a median income in the bottom 25% of all counties was 1.4 times more likely to ride without a helmet compared with a child living in a county with a median income in the top 25%. Sex did not significantly predict helmet use in multivariable analysis. In bivariate correlation analysis, median income was shown to correlate with high school graduation rate (R=0.74; p<0.001) and college graduation rate (R=0.85; p<0.001). However, home county scholastic graduation rates were not independent predictors of helmet use in multivariable analysis (table 4).
Multivariable regression for variables predicting unhelmeted riding
Discussion
This study identified demographic and socioeconomic factors associated with unhelmeted recreational ATV and dirt bike injuries. We found in univariate analysis that unhelmeted crashes significantly associated with older age, female sex, ATV use, and riding as a passenger, consistent with prior studies.5 6 13–16 In multivariable analysis, unhelmeted riding at the time of crash was predicted by ATV use, passenger status, and older age. Regarding socioeconomic factors, unhelmeted riding associated with residence in a county with lower median and per capita incomes, higher poverty prevalence, and lower high school and college graduation rates. Lower median income of home county predicted unhelmeted riding at the time of ATV or dirt bike crash.
Considering all study data, we foremost identified counties with highest rates of unhelmeted crashes, which overlapped considerably with counties reporting lower measures of socioeconomic status (figure 2). Although the absolute difference in median income was approximately US$5000, for families earning lower incomes in the range we identified (US$50 000–US$60 000), a roughly 10% difference in income may impact the ability and decision to purchase appropriate protective gear for ATV and dirt bike riding, especially in families with multiple riders. Alternatively, unhelmeted riding may be most prevalent in counties with lower median income and education levels as a result of limited or ineffective injury prevention outreach.17 Reviewing the epidemiology of pediatric injuries that present to comprehensive trauma centers, geographic differences can help direct and tailor injury prevention initiatives to targeted areas that are likely to have the highest impact.37 Consistent with our findings, a recent study using geospatial mapping in ATV crashes reported that isolated rural ATV crash victims were less likely to be helmeted, and rural victims were over-represented among fatalities.35 This trend may be represented in our data by the finding that unhelmeted riders disproportionately required helicopter transportation to the hospital compared with the helmeted group. This disparity may be due to unhelmeted riders’ sustaining more severe injury necessitating air transportation, or due to a greater proportion of unhelmeted riders living in rural areas further from a trauma center.
Furthermore, within these resource-constrained counties, we determined that older age, ATV use, and riding as a passenger confer greater likelihood of an unhelmeted crash. No difference in insurance type between the two groups appeared, although prior research has noted private insurance to be more frequent in helmeted riders compared with unhelmeted.42 Prior research on this topic has also found that rural, non-Hispanic, white men are most likely to die from an ATV injury, and that mortality rate on ATV declined by an estimated 3.1% for every unit rise in the per cent of the college-educated population.16 Demographically, our study cohort was 92.8% white and 71.3% male. Only 3.1% self-identified as Hispanic. The homogeneity of our study cohort makes it challenging to discern other demographic trends that might exist.
With the understanding that education is often the most effective injury prevention intervention, our findings can be leveraged to target injury prevention initiatives to the counties and individuals most at risk for experiencing an unhelemted crash. Prior educational initiatives have focused on both promoting helmet use and teaching safe riding practices, reporting variable success.7 23–25 One key barrier to success is that many adolescents report that they prefer to listen to a friend or peer—particularly one with experience riding ATVs or dirt bikes—as opposed to medical personnel or public health experts regarding safe riding habits.8 43 Effective, community-based injury prevention programs tend be multifaceted and leverage existing community organizations and infrastructure, such as hospitals, schools, the media, and/or sponsorship by private industry.44 45 Coupled with peer-to-peer interventions and knowledge of developmental psychology, these programs may serve as yet another effective avenue in changing behaviors among youth.46 47 Moreover, injury prevention messages that reach children and adolescents without involving caregivers fall short, as behavior modeling and rule enforcement are key components of improving helmet use and safe riding practices.48 49 Indeed, our institution recently launched the ‘Ride On TN’ ATV safety program through partnership with local 4-H and Future Farmers of America groups. The program includes two phases: a ‘hospital training’ phase in which students are introduced to the medical impacts of unsafe ATV use and a ‘community outreach’ phase through which students engage in a peer-to-peer education campaign. As of the 2020–2021 school year, the program has expanded to include seven high-risk counties; however, due to the COVID-19 pandemic the ‘hospital training’ phrase could only be offered virtually. A longer follow-up period is necessary to comprehensively assess the clinical impact of this program.
The key limitation of our study is that, although injury and outcomes data were collected for each individual, all variables regarding economic and education status were collected at the county level via published US Census data. It is difficult, therefore, to attribute county-level economic and scholastic information to the individual rider and their family. However, for the purposes of targeting injury prevention initiatives, county-level information about helmet use and socioeconomic status are useful to guide interventions geographically. Additionally, because all data were collected from a single level 1 pediatric trauma center, it is possible that our study disproportionately captures more severe injuries requiring a higher level of care. This study does not include children who may have received care at a local hospital, and we therefore cannot comment on total incidence of crashes or percent of unhelmeted crashes in a county. We can comment only on children within our institution’s geographical catchment area and children with injuries severe enough to warrant transport to an ACS-verified level 1 pediatric trauma center. Furthermore, although our institution has a large catchment area in the southeastern USA, these trends might not apply to other regions of the country. A similar analysis on a nationwide level would be interesting and helpful to further inform policy changes. Variability also exists between ATV and dirt bike fatality rates by state, with states having some level of safety legislation reporting substantially fewer deaths and lower fatality rates than states without ATV safety laws.20 22 However, compliance with and enforcement of these laws is also variable, and policy alone is insufficient to change behavior for many riders.
Conclusion
To promote helmet use when riding recreational off-road vehicles, we recommend a multifaceted ATV and dirt bike education and safety program that is peer-driven and incorporates community organizations in counties with lower median incomes and scholastic graduation rates, where unhelmeted crashes are disproportionately more common. Furthermore, we encourage partnering with national organizations to develop media campaigns and uniformed messaging around risky ATV and dirt bike riding. Future research on population-level factors that impact helmet use are needed, as are systems-level changes in education and outreach to address these disparities.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the institutional review board (no. 130583, 210071).
References
Footnotes
Presented at This study has been presented as an oral presentation at the Tennessee Chapter of the American College of Surgeons as well as in poster form at the American College of Surgeons Annual Congress and the American Academy of Pediatrics Conference.
Contributors Conception and design: KLV, HNL. Acquisition of data: KLV, JHA, AMY-K, KGM, ALG, OG, PU. Analysis and interpretation of data: KLV, JHA, AMY-K, PU, HNL, CMB. Drafting the article: KLV, PU, HNL. Critically revising the article: JHA, AMY-K, KGM, ALG, OG, CMB. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: KLV. Statistical analysis: KLV, JHA, PU, OG, HNL. Administrative/technical/material support: PM, PU, ALG, OG, HNL, CMB. Study supervision: PU, HNL. Guarantor: HNL.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests AMY-K serves on the scientific advisory board for BlinkTBI, which had no role or involvement in this study. The remaining authors have no conflicts of interest to disclose related to this topic.
Provenance and peer review Not commissioned; externally peer reviewed.