Article Text

Abstract
Background Given the widespread use of bicycles on public roadways, bicyclists injured in automobile collisions present a familiar problem to trauma centers worldwide. The aims of this study are to characterize the current injury patterns and to quantify independent risk factors for preventable injury and death, with a focus on helmet utilization and traumatic brain injuries.
Methods This is a retrospective study using the American College of Surgeons Trauma Quality Improvement Program database for the period 2010 to 2016. Data were abstracted for bicyclists ≥16 years of age injured by an automobile. The primary outcome of interest was mortality. The secondary outcomes included intracranial, facial, and cervical spine injuries, as well as polytrauma. We used multivariate logistic regression to identify risk factors associated with outcomes.
Results Of the 980 955 cases in the database, 7159 (0.73%) were bicyclists involved in a collision with an automobile. The median age was 45 years and 85% of patients were male. Polytraumatic occurrences accounted for 58% of injuries. Helmet use was reported in 25.4% of cases, a rate that did not change significantly during the study period. Helmet utilization was higher in those aged >65 years and in patients located in the West and Northeast regions of the USA. Helmet use was associated with an overall lower incidence of all reported forms of intracranial injuries. Overall mortality was 7.4%. Independent risk factors associated with mortality included age >65, lack of helmet use, head injury, and abdominal injury.
Discussion Bicyclists injured in collisions with an automobile are at high risk of severe injury and mortality. Preventive strategies should target older bicyclists, helmet utilization, and increasing helmet accessibility for all bicyclists using roadways.
Level of evidence Level IV.
- Automobile
- helmet
- TBI
Data availability statement
Data sharing not applicable as no datasets generated and/or analyzed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Although there is a significant amount of data on the protective effects of helmets for bicyclists as well as the injury patterns associated with falls from a bicycle, there are few studies that looked specifically at the mechanism of bicyclists versus automobiles (BVAs).
Our anecdotal experience as a level 1 trauma center in an urban environment is that the number of BVA collisions has been increasing in recent years and that these patients have more severe injuries than other mechanisms of bicycle falls.
BVA collisions represent a higher energy transfer mechanism and often lead to greater injury severity.
A clearer understanding of this trauma population will help to inform the development of enhanced preventive strategies to mitigate preventable bicycle-associated injuries, particularly traumatic brain injuries.
WHAT THIS STUDY ADDS
We show that bicyclists in accidents involving motor vehicles are at high risk of severe traumatic brain injury and mortality and that these injuries are associated with significant hospital resource utilization.
If we make the assumption that bicyclists generally represent a healthy segment of the population, injury prevention in this demographic will have a significant impact on quality of life and years of productivity.
Our data support current literature that helmets are associated with a protective effect against mortality, intracranial injury, and decreased hospital resource utilization.
Our article observed that socioeconomic status, geographical location, and substance use are additional independent risk factors for morbidity and mortality.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Succinctly, our results will help to inform targeted preventive strategies and direct resource allocation to patients and populations at increased risk of severe injury.
We think strongly that programs designed to increase helmet utilization should continue to be pursued, particularly for bicyclists interested in sharing roadways with automobiles.
Introduction
Bicycles are a widely used form of transportation throughout the world. Although bicycles are used in many settings, including as primary or alternative transit, sport, and recreation, there has been a surge in utilization in urban/metropolitan centers. Cyclists are vulnerable to severe injuries, particularly when the mechanism of injury involves a collision with a motor vehicle.1 Bicycle versus automobile (BVA) collisions are a common presentation of injury to trauma centers and represent a significant burden of healthcare costs, at $22.4 billion in 2013.2
Traumatic brain injury (TBI) is one of the most common causes of trauma-associated morbidity and mortality in the USA.3 TBIs sustained in bicycle accidents constitute one of the leading causes of sport-related brain injuries. Prior research examining the protective role of helmet use in TBI shows significant reduction in the incidence and severity of TBI in single-bike accidents4–9; however, the protective effect of helmets has not been well studied in BVA collisions.
The objective of this study is to perform an epidemiological analysis of bicyclists injured in collisions with automobiles. We characterize risk factors for mortality, TBI, and spinal cord injuries. Furthermore, we discern the protective effects of helmet utilization and describe the outcomes of these injuries using data from a national trauma registry database. A clearer understanding of this trauma demographic will help to inform the development of enhanced preventive strategies to mitigate preventable bicycle-associated injuries, particularly TBIs.
Methods
Data source and selection of variables
A 7-year (2010–2016) analysis of the American College of Surgeons Trauma Quality Improvement Program (ACS-TQIP) was performed. The ACS-TQIP is a nationwide trauma database that contains approximately one million patients, representing data from more than 800 trauma centers across the USA. The database includes morbidity and mortality outcomes of patients sustaining all types of traumatic injury, including those secondary to collisions with automobiles.10
Inclusion criteria were determined by age (>16 years) and by the associated International Classification of Diseases (ICD-9) code. Specifically, ICD-9 e-codes associated with BVA collisions were used: 811.6 (pedal bicyclist involving re-entrant collision with another motor vehicle), 812.6 (pedal bicyclist involving collision with motor vehicle), 813.6 (pedal bicyclist involving collision with other vehicle), 815.6 (other pedal bicyclist involving collision on a highway), 817.6 (non-collision pedal cyclist while boarding or alighting), and 818.6 (other collision involving pedal bicyclist). Transfer patients, or those transferred into an ACS-TQIP participating center from a lower level of care, were excluded from this study to maintain data homogeneity.
The primary endpoint of this study is mortality. The secondary outcomes included the following: intracranial hemorrhage (further characterized into subgroups: epidural, subdural, and subarachnoid hemorrhage), facial fractures, cervical spinal fracture, injuries by body region (thoracic, abdominal, pelvis, upper extremity, lower extremity), polytrauma, hospital length of stay, intensive care unit (ICU) length of stay, and ventilator days.
Statistical methods
Descriptive statistics (including mean, SD, median, IQR, frequency, and percent) were used for demographics and injury characteristics, including ethnicity, sex, Injury Severity Score (ISS), initial systolic blood pressure, and initial Glasgow Coma Scale score. Univariate analysis was employed to determine potential correlation with primary and secondary endpoints. The two-sample t-test and non-parametric Wilcoxon rank-sum test were used to compare mean and median differences between patients with different outcomes, respectively. χ2 test and Fisher’s exact test were used to compare proportions of categorical demographic or injury patterns between patients with different outcomes. Univariate and multivariate logistic regression was performed to evaluate the association between helmet utilization and outcome. Covariates in all of the multivariate models included age, gender, insurance status, and intoxication. For mortality analysis, intracranial injury and abdominal injury were added as covariates. A two-sided p value of <0.05 was considered statistically significant. Statistics were performed using SAS software (V.9.4; SAS Institute, Cary, NC).
Results
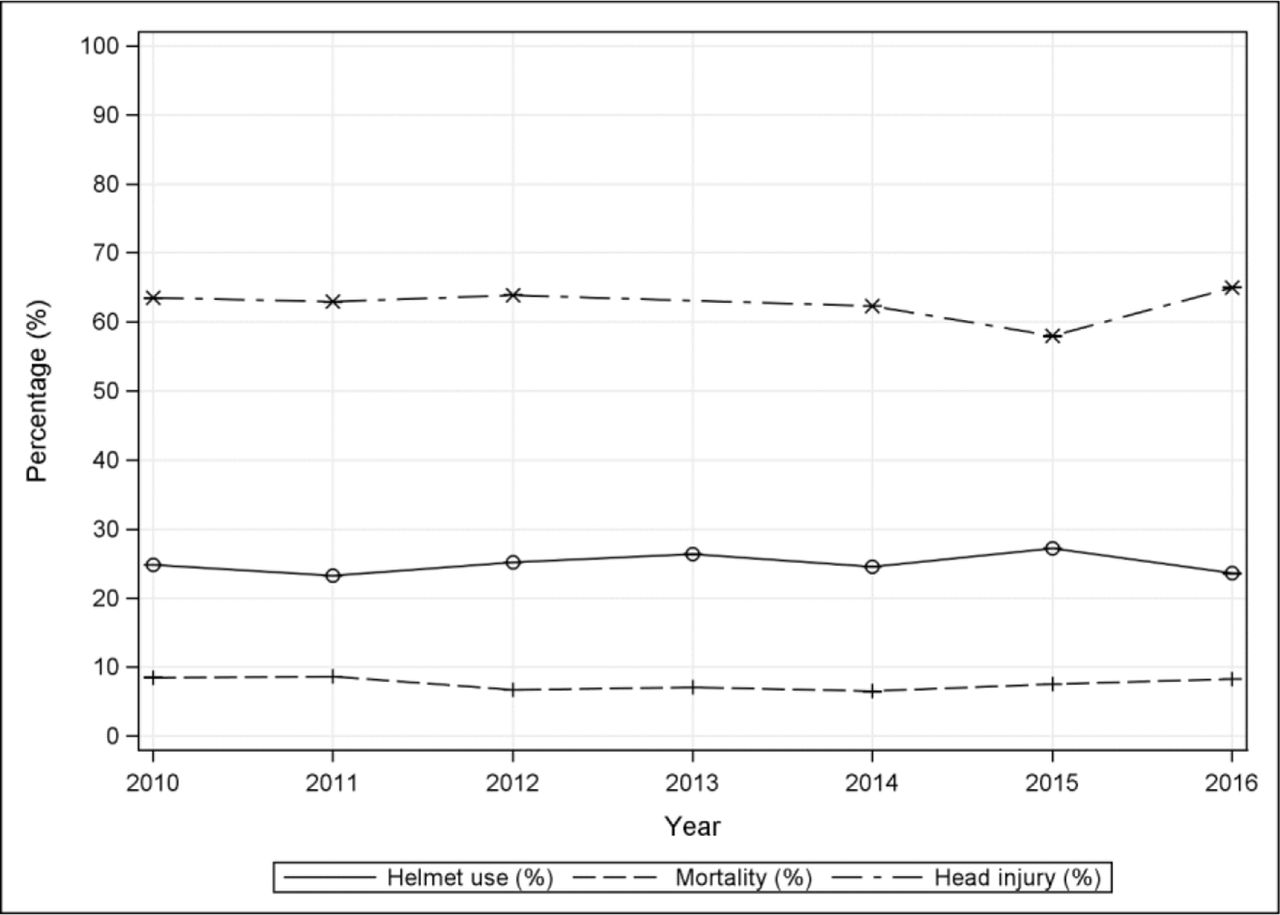
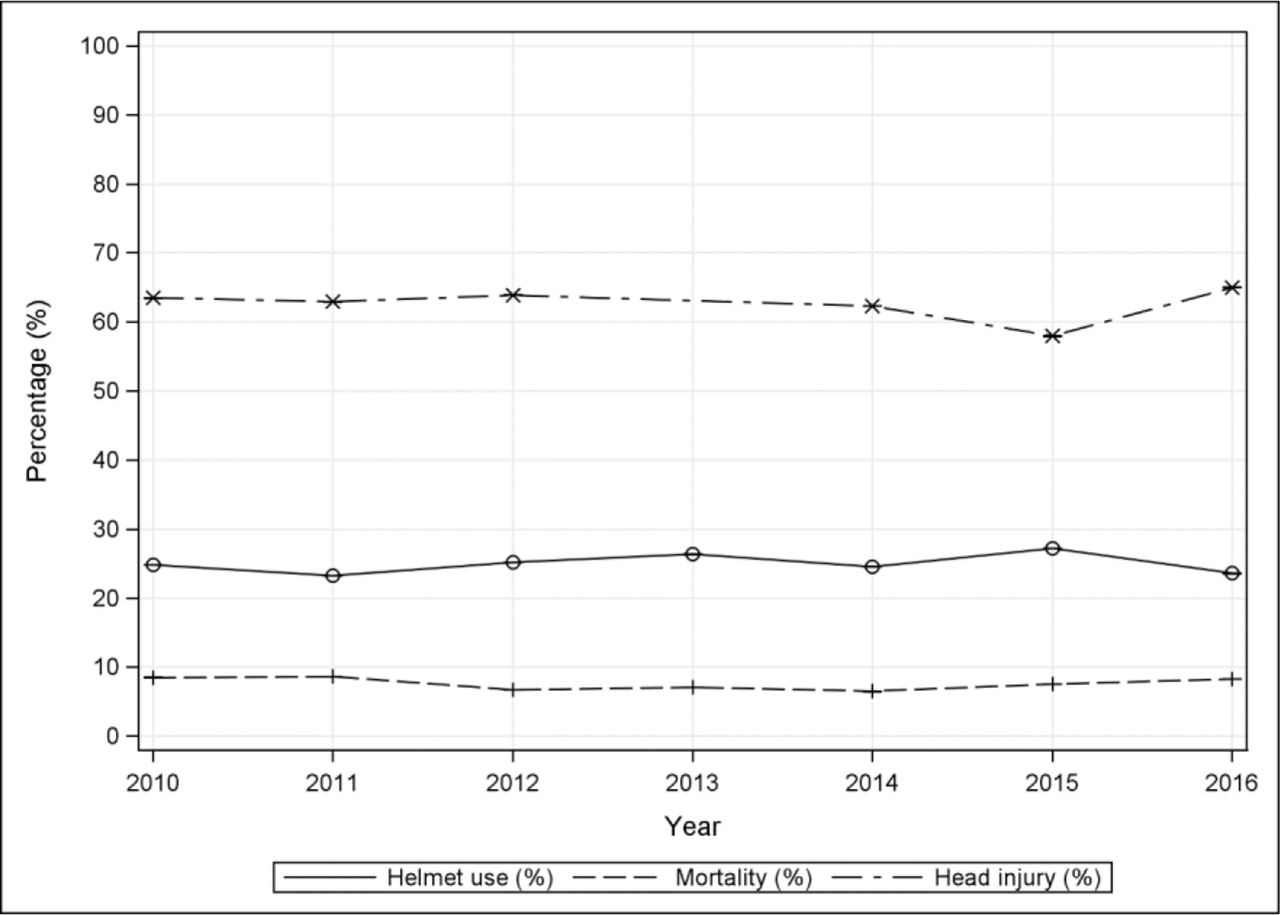
Of the 1 223 349 patients included in the ACS-TQIP database during the period of study, 8409 (0.7%) were bicyclists involved in a collision with an automobile. Of these, 1250 (14.8%) were excluded as they were transferred in from a separate trauma center, leaving 7159 for analysis. Table 1 displays the demographics and injury characteristics of the study population. The median age was 45, with the majority of studied bicyclists being male (85.3%). The median ISS was 14, with 48.0% of injuries categorized as severe (ISS >15). The overall mortality rate was 7.4%. The most common anatomic injury patterns included the head (53.5%), chest (44.8%), and lower extremities (34.7%). Of the reported injuries, 58.3% qualified as “poly-trauma,” affecting multiple anatomic systems; 25.4% were documented as wearing a helmet at the time of injury and 34.5% presented with evidence of alcohol or substance intoxication on arrival at the emergency department. Figure 1 illustrates that the rate of helmet use, head injury, and mortality did not change significantly during the study period (p>0.05 for all three outcomes over time).
{kind=link}
Helmet use, head injury, and mortality during the study period (2010–2016). Note that none of the trends over time were statistically significant (all p>0.05 by Pearson correlation coefficient test).
Characteristics of bicyclists involved in collisions with automobiles
Differences in patient characteristics stratified by helmet use are depicted in table 2. Helmet use was positively correlated with age (36% over 65 years were helmeted, 29% were 45–65 years, and 21% were <45 years) and negatively correlated with intoxication (17% helmeted patients were intoxicated vs. 40% non-helmeted) and insurance status (7% helmeted were uninsured vs. 19% of non-helmeted patients).
Patient characteristics associated with helmet use
Helmet utilization and clinical outcomes based on injury patterns are shown in table 3. In this study, helmet utilization was protective against mortality (adjusted OR (aOR) 0.53, 95% CI 0.42 to 0.67), all types of intracranial injury (aOR 0.69, 95% CI 0.61 to 0.77), including epidural, subdural, and subarachnoid hematoma, and facial fractures (aOR 0.76, 95% CI 0.66 to 89). Covariates and their associated ORs in the mortality regression analysis included age >65 (vs. ages 18–45, aOR 2.2, 95% CI 1.7 to 3.0; vs. ages 46–65, aOR 1.6, 95% CI 1.2 to 2.1), uninsured status (aOR 1.5, 95% CI 1.2 to 1.9), abdominal injury (aOR 2.3, 95% CI 1.8 to 3.1), and intracranial injury (aOR 2.2, 95% CI 1.7 to 2.7) as independent risk factors for mortality.
Mortality and injury risks associated with helmet use
Mandibular fractures did not appear to be significantly associated with helmet use (helmet 2.1% vs. non-helmeted 2.9%, p=0.10). Helmet use was associated with an increased risk of cervical spine injury (aOR 1.69, 95% CI 1.47 to 1.96). Of the 732 patients with cervical spine injury, only 12 (1.6%) sustained a concurrent spinal cord injury.
Hospital resource utilization stratified by helmet use is demonstrated in table 4. Helmeted bicyclists had shorter hospital length of stay (6.9 days vs. 9.5 days, p<0.001). For those admitted to the hospital, a 5.0% risk reduction for ICU admission was observed. For those admitted to the ICU, helmeted bicyclists saw shorter average ICU length of stay (7.5 days vs. 8.8 days, p<0.001) and a decreased incidence of intubation (16.3% vs. 26.0%, p<0.001).
Hospital resource utilization stratified by helmet use
Discussion
This study represents one of the largest database analyses describing bicyclists injured in the context of bicycle versus automobile collisions. With the rise in popularity of bicycling, particularly in urban environments, we posit that public health experts and medical practitioners can employ evidence-supported outcomes data to target interventions in their respective communities. The joint report “Bicyclists Fatalities and Serious Injuries in New York City” from the New York City Departments of Health and Mental Hygiene, Parks and Recreation, and Transportation, and the Police Department presents findings similar to our study.11 12
Regarding critical injuries sustained by bicyclists, Lustenberger et al1 found a mean ISS of 10.7±10.3, where 23% sustained severe or critical injuries (ISS >15). This was corroborated by Scott et al,13 with a mean ISS of 11.06±9.33, and Joseph et al,5 with a median ISS of 10, in smaller regional studies. In our nationwide analysis, we found an overall higher severity of injury (median ISS of 14), where 48% of injuries were categorized as severe (ISS >15). Our study population focused on BVA, which represents a higher energy trauma mechanism than bicycle accidents as a whole, thus contributing to the increased ISS observed in our study.
The protective effects of helmets in preventing severe head and intracranial injuries as well as mortality are well established. Joseph et al,5 using the National Trauma Data Bank, described intracranial injuries in bicycle-related accidents and showed that helmeted bicycle riders had 51% reduced odds of severe TBI and 44% reduction in mortality, findings that are in agreement with our study. These findings are further corroborated by a meta-analysis performed by Høye6 that involved 55 studies during a 28-year period (1989–2017) which noted helmet use was associated with reduction in any head injury (48%), severe head injury (60%), TBI (53%), and all-cause mortality in bicycle-related injuries (34%). The current study adds further weight to the body of evidence supporting the use of helmets as a means of primary prevention of injuries in bicycle-related trauma.
The association between helmet use and cervical spine injury is an area of active research. There is evidence that suggests helmets may increase the risk of cervical spine injury either from direct impact of the helmet to the riding surface or additional head/neck torsion caused by the weight of the helmet.8 Recent meta-analyses, however, refute this notion.6 7 Computational analyses simulating bicycle collisions with automobiles similarly conclude helmets confer protective effects against cervical spine injury.9 Our data show a significantly increased risk of cervical spine injury in helmeted cyclists, although the incidence of cervical spinal injuries was much lower than intracranial injuries and the observed prevalence of spinal cord injuries was very low. Thus, the marginal increased risk of cervical morbidity attributable to helmet use is far outweighed by the associated protective benefits against TBIs.
Our results agree with the trauma literature showing a significant protective effect with helmet use. Less clear, however, are the reasons why helmet utilization rates have not changed significantly despite such overwhelming evidence supporting their use. Jewett et al14 attempted to identify factors affecting helmet use, including the impact of living in an urban environment and socioeconomic status. Their study found that adults with an annual income greater than $85 000 and those living in an urban environment were more likely to use helmets. Similarly, we observed that lower socioeconomic status as reflected by lack of medical insurance was correlated with decreased helmet utilization. Residents of the Northeast and West were also more likely to use helmets, with 28.7% and 30.9% utilization rates, respectively. This may be due to the higher density of urban trauma centers in these geographical locations rather than the more rural regions of the USA.
Alcohol intoxication is a clear risk factor for serious injury in BVAs. This is the result of alcohol’s depressive effect on psychomotor skills and disinhibition resulting in higher risk-taking tendencies, including deferring helmet use. Li et al15 found 8% of cyclists with blood alcohol content (BAC) of 0.02 g/dL or higher were wearing a helmet, whereas 38% of cyclists with a BAC lower than 0.02 g/dL were wearing a helmet. Although causality cannot be established with the available literature, correlation is well established. This also falls in line with our observations that 17% of helmeted cyclists had a normal blood alcohol level versus 40% of unhelmeted cyclists who presented with a documented elevated blood alcohol level. These findings suggest that alcohol counseling and concomitant short brief interventions and referrals for treatment of alcohol misuse may present another area for targeted intervention as a means of primary prevention of future injuries.
The use of ICU resources leads to substantial costs to individuals, hospital systems, and the greater public at large. In the present study, helmet use was associated with a significant reduction in hospital length of stay, ICU admission rate, ICU length of stay, and reduction in the number of ventilation days. These findings are consistent with previous studies.13
There were several limitations to this study. First, this was a retrospective analysis using a national database registry. Although correlation may be easily observed, only inferences can be made with respect to causality. This study was subject to selection bias based on the available trauma centers submitting data to the ACS-TQIP database. The data set will invariably become more robust as the number of contributing centers is increasing annually; however, the total number and severity of injuries related to bicycles are likely underestimated given the voluntary nature of ACS-TQIP participation. There was no way to verify the correct data abstraction into the TQIP database from each center’s trauma registry. For this reason missing data were a significant limitation. Bias from missing and misclassified data was also an inherent limitation of this study.
Despite these limitations, we conclude that bicyclists in accidents involving motor vehicles are at high risk of severe TBI and mortality and that these injuries are associated with significant hospital resource utilization. If we make the assumption that bicyclists generally represent a healthy segment of the population, injury prevention in this demographic will have a significant impact on quality of life and years of productivity. Our data support the current literature that helmets are associated with a protective effect against mortality, intracranial injury, and decreased hospital resource utilization. Our article observed that socioeconomic status, geographical location, and substance use are additional independent risk factors for morbidity and mortality that can be specifically targeted for preventive strategies and resource allocation. Further efforts to build targeted safety outreach programs are currently warranted.
Data availability statement
Data sharing not applicable as no datasets generated and/or analyzed for this study.
Ethics statements
Patient consent for publication
Ethics approval
This study was exempt from approval by the NYPQ IRB.
Footnotes
Presented at This abstract was presented as a poster at the American College of Surgeons (ACS) Clinical Congress meeting in Boston, Massachusetts, on October 21–25, 2018.
Contributors AdR and PS designed the study. AdR and AT-D conducted the literature search and data collection. AdR, OFT, AT-D, EZ, KK, and PS analyzed the data and contributed to data interpretation. AdR, OFT, AT-D, EZ, KK, and PS wrote the article. AdR, OFT, AT-D, EZ, KK, and PS edited the article. AdR is the guarantor for this article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.