Article Text

Abstract
Objectives During temporary abdominal closure (TAC) with damage control laparotomy (DCL), infusion volume and negative-pressure wound therapy (NPWT) output volume are associated with the success and prognosis of primary fascial closure. The same may also hold true for anastomosis. The aim of this research is to evaluate whether the difference between early anastomosis and delayed anastomosis in DCL is related to infusion volume and NPWT output volume.
Methods This single-center retrospective analysis targeted patients managed with TAC during emergency surgery for trauma or intra-abdominal sepsis between January 2011 and December 2019. It included patients who underwent repair/anastomosis/colostomy in the first surgery and patients who underwent intestinal resection in the first surgery followed by delayed anastomosis with no intestinal continuity.
Results Seventy-three patients were managed with TAC using NPWT, including 19 cases of repair, 17 of colostomy, and 37 of anastomosis. In 16 patients (trauma 5, sepsis 11) with early anastomosis and 21 patients (trauma 16, sepsis 5) with delayed anastomosis, there was no difference in the infusion volume (p=0.2318) or NPWT output volume (p=0.7128) 48 hours after surgery. Additionally, there was no difference in the occurrence of suture failure (p=0.8428). During the second-look surgery after 48 hours, the anastomosis was further postponed for 48% of the patients who underwent delayed anastomosis. There was no difference in the infusion volume (p=0.0783) up to the second-look surgery between the patients whose delayed anastomosis was postponed and those who underwent delayed anastomosis, but there was a tendency toward a large NPWT output volume (p=0.024) in the postponed delayed anastomosis group.
Conclusion Delayed anastomosis may be managed with the same infusion volume as that used for early anastomosis. There is also the option of postponing anastomosis if the planned delayed anastomosis is complicated.
Level of evidence Therapeutic/Care Management, Level IV.
- abdominal injuries
- colectomy
Data availability statement
Data are available upon reasonable request. Relevant data are presented in the published manuscript. Data are available on reasonable request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic?
Delayed anastomosis is a treatment strategy used in damage control laparotomy (DCL). This research investigates the need to restrict infusion corresponding to delayed anastomosis by evaluating whether the difference between early anastomosis and delayed anastomosis in temporary abdominal closure management using negative-pressure wound therapy (NPWT) is associated with infusion volume and NPWT output volume.
What this study adds?
This research showed that infusion restrictions were not necessary in delayed anastomosis compared with early anastomosis.
How this study might affect research, practice or policy?
Improving treatment outcomes for patient management with delayed anastomosis.
Introduction
Delayed anastomosis is a treatment strategy that is incorporated into damage control laparotomy (DCL) according to the physiological indicators and intra-abdominal environments of patients who have no intestinal continuity after undergoing only intestinal resection during initial surgery for hollow viscous injury (HVI) or mesenteric injury (MI).1–6 After DCL, the patient is moved quickly to the intensive care unit for correcting hypothermia, acidosis, coagulative disorders and performing physiological optimization.1 7–9 Temporary abdominal closure (TAC) using negative-pressure wound therapy (NPWT) is the general approach used until repeat laparotomy is performed. These DCL treatment strategies are applied not only to trauma but also to intra-abdominal sepsis and are very important treatment strategies.10–12 However, the decision to perform anastomosis during the first procedure or delay is complex and must consider the patient’s physiological indicators, damage status, contamination status, and other factors.
It has been reported that during primary fascial closure (PFC) after TAC, excessive infusion leads to tissue edema and prevents successful PFC13–15 and that limited use of the crystalloid infusion protocol improves the success of PFC.16 For similar reasons, excessive infusion may lead to the development of intestinal edema, which may prevent successful delayed anastomosis or require colostomy to avoid anastomosis. In addition, the NPWT output volume in TAC is an important fluid balance index, and hypoalbuminemia, in which albumin is lost when protein-rich ascites are drained,17 may pose a risk of anastomotic leakage18–20 and present a disadvantage for the success of delayed anastomosis. However, there is little information regarding the differences and relevance of infusion volume and NPWT output volume during TAC for the management of early anastomosis and delayed anastomosis in DCL.
The purpose of this study was to evaluate whether the difference between early anastomosis and delayed anastomosis is related to the volume of fluid infusion and NPWT output in patients who underwent emergency surgery due to external injury or intra-abdominal sepsis and opted for DCL.
Methods
Target
This retrospective study was conducted at the Iwate Medical University Critical Care Center from 2011 to 2019 with patients who underwent emergency surgery due to HVI/MI caused by abdominal trauma and patients who underwent emergency surgery for lower digestive tract perforation with diffuse peritonitis and peritoneal contamination in the form of intra-abdominal sepsis. The study included patients who underwent repair/anastomosis/colostomy during the first DCL surgery and were managed with TAC using NPWT and patients who had no intestinal continuity after undergoing intestinal resection during the first surgery and were managed with TAC using NPWT. Clinical data and infusion volume, NPWT output, and urine volume up to 48 hours after surgery were extracted from chart review or clinical records review.
The study excluded patients who died within 48 hours after surgery, patients with solid organ injuries without HVI, patients who underwent non-surgical treatment (for MI or intra-abdominal hemorrhage), patients on maintenance dialysis due to chronic renal failure, and patients with iatrogenic injuries. Patients with perforated appendicitis and patients who underwent resurgery with DCL were not included in the study.
Treatment strategy
DCL, repair, resection and colostomy
Treatment was conducted at the discretion of the surgeon and not protocolized according to specific injury or perforation site and morphology or contamination status. According to the surgeon’s experience, bleeding and organ injuries in trauma cases and contamination and intestinal edema in intra-abdominal sepsis cases are the main reasons for choosing DCL. Intestinal resection was performed using a stapler. In cases in which delayed anastomosis was selected, the end of the intestinal resection remained stapled, and the intestine was left discontinuous and was directed into the abdominal cavity. No temporary ileostomy or colostomy was created until anastomosis was performed. For delayed anastomosis, second-look surgery was performed 48 hours after the initial surgery to evaluate whether to restore intestinal continuity or create colostomy. Other options included postponing anastomosis with no intestinal continuity and postponing abdominal closure. When TAC was continued, the condition of the intestinal tract was evaluated in a timely manner at the intensive care unit or high-dependency care unit, and the abdomen was closed after anastomosis or colostomy was selected at the discretion of the surgeon. Regarding the anastomosis technique, stapling anastomosis was performed in all cases, and hand-sewn anastomosis was not performed. For resection and anastomosis, a linear cutter (ETHICON, USA) was used. Functional end-to-end anastomosis was performed. Ileostomy was not performed after anastomosis.
Infusion resuscitation
The infusion dose was based on physiological indicators such as heart rate, blood pressure, etc, and the diameter of the inferior vena cava according to ultrasound examination. Infusion up to 48 hours after surgery included basic infusion crystalloid fluid, bolus-administered crystalloid fluid, and albumin preparations. For the crystalloid fluid, acetated Ringer’s solution was used. The administration of the albumin preparation was capped at 1 dose of 100 mL 20% albumin preparation per day. Albumin administration was indicated by the presence or absence of administration rather than by the infusion volume because the dose was limited. There was no protocol for bolus administration of crystalloid solution corresponding to the NPWT output amount. Furosemide was not used for up to 48 hours after surgery. When hemodynamics were unstable even after sufficient infusion (systolic blood pressure less than 90 mm Hg), the administration of 0.05 µg/kg/min of norepinephrine as a vasopressor was started.
Negative-pressure wound therapy
NPWT was performed with a handmade negative pressure system after the abdominal cavity was thoroughly rinsed with saline. The intra-abdominal organs were covered with a sterile vinyl sheet. A 28 Fr gastric catheter was placed on the top of the vinyl sheet, a transparent adhesive film was affixed to the top of the catheter, and TAC was performed with a suction pressure of −30 cmH2O. After that, an elastic band was used to cover the abdomen to prevent the abdominal wall from retreating. During TAC management, sedatives, analgesics, and neuromuscular blocking drugs were administered and controlled based on ventilator monitoring.
The same surgical team handled everything from the diagnosis to the surgery and postoperative management of patients with trauma and sepsis. The operations were performed by general surgeons with the assistance of senior surgeons with extensive experience in DCL and TAC management. Since a senior surgeon always intervenes, starting from the beginning of the surgery, the influence of the surgeon’s experience on the surgery was limited.
Definitions and study outcomes
Patients were classified as follows. Patients who underwent repair/anastomosis/colostomy during the DCL first surgery and were managed with TAC using NPWT were classified as DCL-early, and patients who had no intestinal continuity after intestinal resection during the first surgery and were managed with TAC using NPWT were classified as DCL-delay. Patients who underwent early anastomosis were classified as DCL-early anastomosis, and patients who underwent delayed anastomosis were classified as DCL-delayed anastomosis. Patients were also grouped according to whether they underwent delayed anastomosis during second-look surgery 48 hours after the initial surgery or their delayed anastomosis was postponed.
The important research results were infusion volume and NPWT output up to 48 hours after the initial surgery with early anastomosis and delayed anastomosis.
Secondary results were the delayed anastomosis implementation status and frequency of complications. Complications were surgical site infection (SSI), intestinal obstruction, and suture failure.
Statistical analysis
All statistical analyses were performed with the statistical package JMP V.11 (SAS Institute, Cary, North Carolina, USA). Continuous variables are expressed as the mean±SD. Categorical variables are expressed as frequency (n, %), as appropriate. Normal distribution of all data was confirmed using the Shapiro-Wilk test. The data were analyzed using the Χ2 test, Wilcoxon rank-sum test, and Kruskal-Wallis test. When a significant difference was found by the Kruskal-Wallis test, the significance of the difference was examined by the Wilcoxon rank-sum test; p values of <0.05 were considered to indicate statistical significance. As this study was a single-centre cohort study with a limited sample size, a sample size power analysis was not performed.
Results
Study population
A total of 109 patients were included in this study (figure 1). Among the 49 patients with trauma, 10 (20%) had penetrating trauma. Among the 49 trauma patients, injury to the large intestine that required repair or anastomosis was observed in 21. The site of large intestinal injury was the ascending colon in 33% (seven patients), the transverse colon in 38% (eight patients), the descending colon in 14% (three patients), the sigmoid colon in 28% (six patients) and in two different sites of the large intestine in three patients. The site of perforation of the lower digestive tract was the ascending colon in 15% (9 patients), the transverse colon in 8% (5 patients), the descending colon in 3% (2 patients), the sigmoid colon in 55% (33 patients), the rectum in 13 patients (21%) and several different sites of the large intestine in 2 patients. There were 73 patients who underwent DCL and were managed with TAC using NPWT, including 36 (73%) with trauma and 37 (62%) with intra-abdominal sepsis. Twelve patients died within 48 hours of the initial surgery. None of the patients were able to maintain their circulatory dynamics after the surgery. Seven trauma patients were excluded from the study. The time to death was 15.2±9.3 hours, the duration of surgery was 109.5±70.9 min, and the surgical blood loss was 2297.2±1811.9 mL.
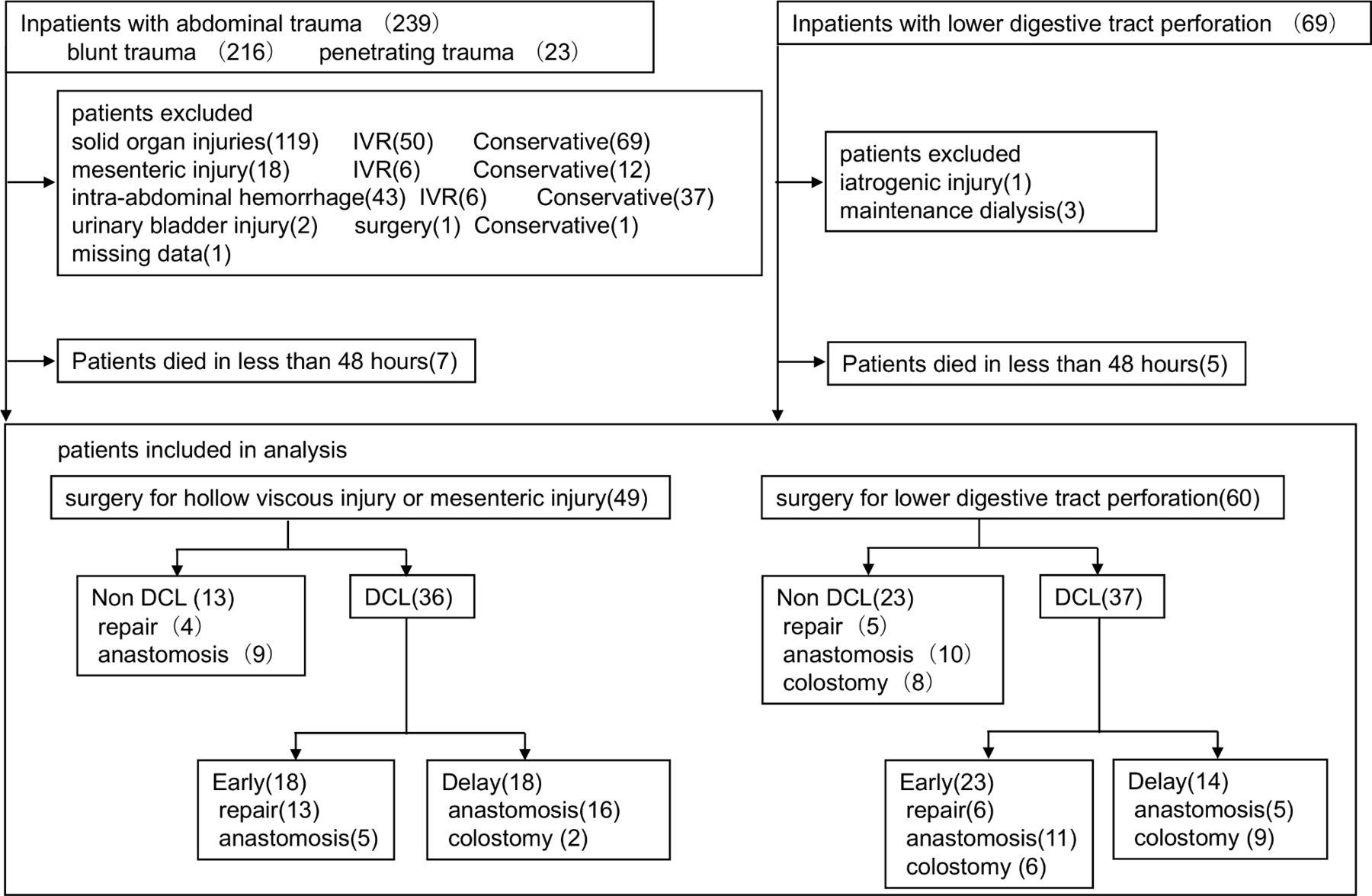
{kind=link}
Study flow chart. DCL, damage control laparotomy; IVR, interventional radiology.
Five patients with intra-abdominal sepsis were excluded. The time to death was 25.4±15.5 hours, the duration of surgery was 169.2±46.1 min, and the surgical blood loss was 356.4±471.2 mL.
Clinical characteristics of the no-DCL, and DCL-early and DCL-delay patients
The no-DCL group included nine patients who underwent repair, eight who underwent colostomy (including one who underwent the Miles technique), seven who underwent small intestine–small intestine anastomosis, six who underwent small intestine–colon anastomosis, and six who underwent colon–colon anastomosis.
The DCL-early group included 19 patients who underwent repair, 6 who underwent colostomy (including 3 who underwent the Miles technique), 1 who underwent stomach–small intestine anastomosis, 3 who underwent small intestine–small intestine anastomosis, 2 who underwent small intestine–colon anastomosis, 7 who underwent colon–colon anastomosis, and 3 who underwent colon–rectal anastomosis.
During the second-look procedure, the DCL-delay group included seven patients who underwent ileostomy, four who underwent colostomy, six who underwent small intestine–small intestine anastomosis, five who underwent small intestine–colon anastomosis, eight who underwent colon–colon anastomosis, and two who underwent colon–rectal anastomosis. Of the seven patients who underwent ileostomy, five required total colectomy.
The average Injury Severity Score (ISS) for overall trauma was 24.3±10. The average Acute Physiology and Chronic Health Evaluation II (APACHE II) score for overall intra-abdominal sepsis was 30.8±6.7. At the time of DCL, 21 patients (29%) had abdominal packing, including 19 trauma patients and 2 patients with sepsis. No patients were administered hypertonic saline.
The average infusion volume up to 48 hours from surgery in all patients who underwent DCL was 11246.5±4305.0 mL, the average NPWT output was 1239.9±712.0 mL, and the average urine volume was 2876.6±2253.1 mL.
In terms of the amount of bleeding during the initial trauma surgery, a significant difference was observed between the no-DCL and DCL-delay groups and between the DCL-early and DCL-delay groups (p=0.0002 and p=0.0004, respectively). In terms of the infusion volume 48 hours after surgery, a significant difference was observed between the no-DCL and DCL-early groups, between the no-DCL and DCL-delay groups, and between the DCL-early and DCL-delay groups (p=0.0001, p<0.0001, and p=0.0128, respectively). There was no difference in the NPWT output or the relaparotomy duration between the DCL-early and DCL-delay groups, and it was possible to achieve PFC in all cases (table 1). Anastomotic leak was observed in a total of six patients, including two in the no-DCL group (one who underwent repair and one who underwent colostomy) and four who underwent DCL (two who underwent repair and two who underwent anastomosis).
Clinical characteristics of the no-DCL, and DCL-early and DCL-delay patients
Comparison of the early-anastomosis and delayed-anastomosis groups
This category did not include patients who had undergone repair or colostomy. Only patients who underwent intestinal tract resection and anastomosis were included. Among the patients who underwent DCL, 16 underwent early anastomosis, and 21 underwent delayed anastomosis. There was no difference in terms of age, APACHE II score, or ISS. The delayed-anastomosis group included several patients with colon injury due to trauma (p=0.0271). The surgery duration was significantly shorter in the delayed-anastomosis group (p=0.0001). No difference was observed in infusion volume, NPWT output, or urine volume 48 hours after the initial surgery. There were no differences in SSI, intestinal obstruction, suture failure, or death within 28 days (table 2). The average time until anastomosis in the delayed-anastomosis group was 72.9±40.9 min. Of the 16 patients with intra-abdominal sepsis, 15 had non-malignant perforations. One patient with malignant perforation was included in the early-anastomosis group. There was no significant difference in total crystalloid administration, total NPWT output, or total urine output (p=0.3121, p=0.5312, p=0.7241, respectively), even after the exclusion of one patient with malignant perforation.
Background factors of early anastomosis and delayed anastomosis in DCL patients
Comparison of the patients who did or did not undergo delayed anastomosis during second-look surgery
During second-look surgery performed 48 hours after the initial surgery, anastomosis was performed in 11 patients and postponed in 10 patients. Among the 11 patients who underwent anastomosis during the second-look surgery, 10 underwent a simultaneous procedure to close the abdomen. Regarding the serum albumin value 48 hours after the initial surgery (before second-look surgery), there was no significant difference between the anastomosis group and the group for which anastomosis was postponed. No patients were completely weaned from norepinephrine at the time of the delayed anastomosis (table 3).
Background factors of patients performing or postponing delayed anastomosis during second-look surgery
Discussion
This research showed that there was no difference in the infusion volume and NPWT output volume between early anastomosis and delayed anastomosis during TAC in DCL. The presence or absence of anastomosis during TAC management does not affect NPWT output volume. In patients with delayed anastomosis who received the same infusion volume as the early-anastomosis patients, anastomosis and abdominal closure were possible in all cases, and infusion restrictions were not necessary in delayed anastomosis compared with early anastomosis. However, it is necessary to exercise care when performing delayed anastomosis. When a delayed anastomosis planned for 48 hours after initial surgery is complicated, the surgeon must consider postponing anastomosis instead of performing it forcibly. Moreover, the serum albumin value 48 hours after the initial surgery is not a useful indicator of whether delayed anastomosis should be postponed or conducted.
The drainage of ascites using NPWT during TAC has been shown to be beneficial due to such effects as the reduction of intestinal edema15 and the lowering of inflammatory mediator levels.21–23 However, there are also reports that suggest that NPWT output volume is correlated with infusion volume and is higher in fatal cases.24 When ascites are drained with NPWT, albumin is lost, which is associated with the failure of PFC after TAC.17 Moreover, hypoalbuminemia is a potential factor for dilutive hypoalbuminemia caused by infusion resuscitation25 26 and is associated with anastomotic leakage after digestive tract surgery.18–20 Loftus et al17 found that late hypoalbuminemia is associated with failure of PFC. In this study, no difference in the serum albumin level 48 hours after surgery was observed between the no-DCL group, the DCL-early group, and the DCL-delay group. Albumin loss due to NPWT output or dilution due to infusion, differenced between abdominal closure and laparotomy, was not related to the albumin value.
In this study, the delayed-anastomosis group included many cases of large intestine damage due to trauma, and bias was observed. Possible reasons are as follows: in large intestine injury, there is no protocol for selecting delayed anastomosis, and the surgeon may have consciously avoided selecting patients with factors such as dislodging of the colon (mobilization) for reconstruction, etc, that may prolong the duration of surgery or cause unnecessary bleeding.
As a result, delayed anastomosis clearly shortened the time of the initial surgery compared with early anastomosis. Additionally, many of the initial operations for which delayed anastomosis was chosen were daytime operations. We think that there was no conscious selection of the type of anastomosis based on the surgery day or the surgery start time. However, one factor is that many patients are examined on weekdays and during the day. The possibility that weekend or night surgery plays a role in choices regarding anastomosis needs to be re-examined with more cases from multiple centers.
The selection of delayed anastomosis over early anastomosis did not increase the need for renal replacement therapy or the administration of vasoactive drugs or albumin. Interestingly, the delayed-anastomosis group tended to have shorter laparotomy duration than the early-anastomosis group. The financial burden associated with TAC management is a result of delayed anastomosis. Delayed anastomosis involves considerable trauma and may be associated less with intra-abdominal contamination than with intra-abdominal sepsis and persistent inflammation resulting from intra-abdominal sepsis and intestinal edema.27 The laparotomy duration found in this study is considered to be a localized result in view of bias regarding the disease and that the abdomen was closed at the discretion of the surgeon.
Additionally, there was no difference in the serum albumin value between the group that underwent delayed anastomosis during second-look surgery and the group in which delayed anastomosis was postponed. From these results, we cannot say that the serum albumin value after 48 hours from the initial surgery is a useful indicator of anastomosis. Considering the limited doses of albumin preparation administered and the low number of suture failures, the administration of exogenous albumin to prevent anastomotic leakage and reduce intestinal edema in cases of delayed anastomosis is not always useful.
The NPWT output was lower, and the urine volume tended to be higher, in the group that underwent anastomosis during second-look surgery than in the group with postponed anastomosis. Sustainable maintenance of urine volume is considered to have reduced NPWT output, and the suppression of intestinal edema made it possible to perform anastomosis. The group in which anastomosis was postponed had higher physiological severity and more frequently received renal replacement therapy. There was no protocol for postponing delayed anastomosis, and the decision was made at the discretion of the surgeon. In the group with postponed anastomosis, the arterial oxygen pressure/fractional inspired oxygen ratio before the second-look surgery tended to be lower, and C-reactive protein tended to be high, and general conditions and inflammation may have been involved in the postponement of anastomosis. Regarding delayed anastomosis after 48 hours, the large NPWT output may be associated with the postponement of anastomosis reflecting persistent inflammation, intestinal edema and general conditions. Additionally, low NPWT output is not necessarily disadvantageous for delayed anastomosis. The effect of drainage due to NPWT output over 48 hours must be comprehensively evaluated in combination with other body fluid balance indicators. It is difficult to think of PFC and anastomosis as the same procedure since their purpose, time to implementation and such differ.
In NPWT management, the optimal negative pressure treatment to maximize tissue growth is approximately −125 mm Hg, and the pressure level when active bleeding due to coagulative failure is suspected is approximately −75 mm Hg.28 29 Loftus et al16 17 27 30 reported that 1300 mL to 1900 mL was the median value of NPWT output up to 48 hours after TAC in four studies that reported NPWT output. However, this could not be confirmed except in one report in which the NPWT negative pressure (suction amount) was −75 mm Hg. In this study, the median value of NPWT output up to 48 hours after surgery was 1080 mL. The NPWT output was less than that in the previously mentioned report. Our suction pressure setting was −30 cmH2O (1 mm Hg=1.36 cmH2O), and low pressure management was considered one of the factors for this comparably low output. Our suction pressure setting was maintained at a low pressure to avoid excessive suction of ascites and to maintain physiological ascites absorption in the abdominal cavity. This study showed that the presence or absence of anastomosis does not impact NPWT ejection volume; however, since the NPWT output volume is predicted to depend on the suction pressure, it is necessary to consider the difference in suction pressure.
The purpose of performing early anastomosis during the initial surgery and selecting TAC is to move the patient to intensive care with the aim of controlling rapid bleeding and contamination, shorten the surgery time to the greatest possible extent, and encourage early physiological optimization.31 However, it is necessary to reconsider some matters, such as the need for TAC with early anastomosis and whether patients for whom early anastomosis is possible might not have been selected for delayed anastomosis. Regarding DCL, overuse32 and increased risk of abdominal complications33 have also been pointed out. In addition, it is necessary to recognize that delayed anastomosis itself can have negative impacts; reports have described it as a disadvantageous treatment strategy34 and have raised the possibility of ongoing peritonitis,35 increased anastomotic leakage if PFC is not possible during second-look surgery,36 and other factors. For anastomosis, we chose stapling anastomosis, which is less dependent on the practitioner’s experience. However, it should be remembered that hand-sewn anastomosis is safe and is superior in situations such as intestinal edema.
This study has several limitations. First, our data were based on a limited number of diseases and cases, and this was a retrospective analysis of data obtained from a single facility. Since the study was not randomized, the results are limited, and there is a risk of bias. Second, the albumin value included in the ascites drained from NPWT was not measured, and therefore, the amount of albumin lost could not be clarified. Third, there are no clear criteria regarding the decision to perform or postpone delayed anastomosis. It is necessary to establish objective treatment selection criteria that do not depend on the subjective judgment of the surgeon. Fourth, patients with trauma and patients with sepsis are not completely comparable. This study reports a restricted result. In the future, reconsideration to address multiple limitations is required.
Conclusions
Compared with patients who underwent early anastomosis, those for whom delayed anastomosis was selected during DCL do not necessarily require infusion restrictions for the purpose of anastomosis. The presence or absence of anastomosis during TAC management does not affect the NPWT output volume, and both early anastomosis and delayed anastomosis can be managed with the same infusion volume. However, in cases in which the planned delayed anastomosis is complicated, it is necessary to postpone anastomosis rather than perform it.
Data availability statement
Data are available upon reasonable request. Relevant data are presented in the published manuscript. Data are available on reasonable request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
The protocol of the study was approved by the Iwate Medical University review board (MH2018-611). Consent to participate is not applicable because the data sets were pseudonymous and this study was retrospective.
Acknowledgments
We thank American Journal Experts (https://www.aje.com) for English-language editing.
References
Footnotes
Contributors YT, SS, and MK designed the study. YT, AK, SS, YN, HS, and KI collected the patient’s clinical data. YT and MK contributed to writing the article. YN, SE, YI, and AS contributed to data interpretation and article drafting. YT, SS, HS, and MK contributed to the statistical analysis and data interpretation. AS contributed to critical revision of the article. All authors read and approved the final article. MK is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.