Article Text

Abstract
Objectives Data from the Centers for Disease Control and Prevention (CDC) show that firearm deaths are increasing in the USA. The aims of this study were to determine the magnitude of potential years of life lost due to firearms and to examine the evolution of firearm deaths on the basis of sex, race, and geographical location within the USA.
Methods Data was extracted (2009–2018) from the National Vital Statistics Reports from the CDC and the Web-based Injury Statistics Query and Reporting System database. Years of potential life lost was calculated by the CDC standard of subtracting the age at death from the standard year of 80, and then summing the individual years of potential life lost (YPLL) across each cause of death.
Results The YPLL in 2017 and 2018 was higher for firearms than motor vehicle crashes (MVCs). In 2018, the YPLL for firearms was 1.42 million and 1.34 million for MVC. Males comprised the majority (85.4%) of the 38 929 firearm deaths. White males had the most YPLL due to suicide, with 4.95 million YPLL during the course of the 10-year period; black males had the most YPLL due to homicide with 3.2 million YPLL during the same time period. The largest number of suicides by firearms was in older white males. Firearm-related injury deaths were highest in the South, followed by the West, Midwest, and Northeast, respectively.
Conclusion Firearms are now the leading cause of YPLL in trauma. Firearm deaths have overtaken MVC as the mechanism for the main cause of potential years of life lost since 2017. Suicide in white males accounts for more YPLL than homicides. Deaths related to firearms are potentially preventable causes of death and prevention efforts should be redirected.
Level of evidence Level III—Descriptive Study.
- firearms
- suicide
- homicide
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Traumatic injuries remain the leading cause of death in the USA for individuals up to the age of 46 years.1 The epidemiology for trauma, causes of death, and injury has been dynamic in the USA as it continually evolves with society and technological changes. Motor vehicle crashes (MVCs) have been the single largest cause of death and have been responsible for the most years of potential life lost (YPLL) due to trauma. Firearm deaths, however, have been increasing during the last decade based on the data from the Centers for Disease Control and Prevention (CDC). With these changes, the YPLL from trauma would also be changing. Thus, the aim of this study was to calculate the YPLL and report the evolving nature of firearm-associated deaths within the USA. We also examine the potential years of life lost within specific subpopulations and geographic regions. By understanding the epidemiology of trauma, it may allow for better allocation of resources to where they are needed the most. It may aid with better awareness, public information and injury prevention efforts.
Methods
Data from the annual National Vital Statistics Reports (NVSR, 2009–2018) were extracted and analyzed. Data from the years 2019 and 2020 were not published at the time these data were analyzed. NVSR is an intergovernmental system of sharing data on the vital statistics of the population of the USA. The finalized information on deaths is derived from state-reported death certificates. NVSR is a monthly report since 1998 and is an official data source for the USA and is from the National Center for Health Statistics, a division of the CDC. A database regarding firearm-related deaths was generated using these annual reports. Data were calculated using the Web-based Injury Statistics Query and Reporting System database (WISQARS).2 YPLL was calculated by the CDC standard of subtracting the age at death from the standard year of 80, and then summing the individual YPLL across each cause of death. Although the current average expected life span in the USA is 78.7 years according to the CDC, the WISQARS only allows YPLL calculation to be either 75 or 80 years and thus we used 80 years as it was closer to the actual life span.
We examined the leading causes of injury and death within the population as a whole and calculated YPLL. YPLL from firearm deaths was further analyzed based on age, gender, injury intent, and geographical region. The total number of deaths and YPLL from firearms and MVCs on the basis of age and gender was extracted from the WISQARS database. The CDC defines four geographical regions within the USA—North, South, Midwest, and West—for which the total deaths and YPLL were also extracted from their database. Generalized additive model was applied to evaluate the significance of change of trend using R software and JoinPoint. The term MVC was used to represent the terminology motor vehicle accidents (MVAs), although the NVSR still reports on MVA and does not yet use the terminology MVC.
Results
YPLL by mechanism (MVC vs firearm)
During the course of the study period, the total 10-year cumulative YPLL for MVC and firearms were 12.9 million years and 12.6 million years, respectively. Firearms surpassed MVC as the leading cause of traumatic death in 2017, as there was 1.44 million YPLL due to firearms compared with 1.37 million YPLL due to MVC (figure 1). This trend continued into 2018 with 83 037 more YPLL attributed to firearms versus MVC. From 2009 to 2018, the annual percent change (APC) of firearm deaths increased by 0.72 yearly (p<0.001), whereas the average APC of MVC decreased by 0.07 yearly (p<0.001) (figure 2).
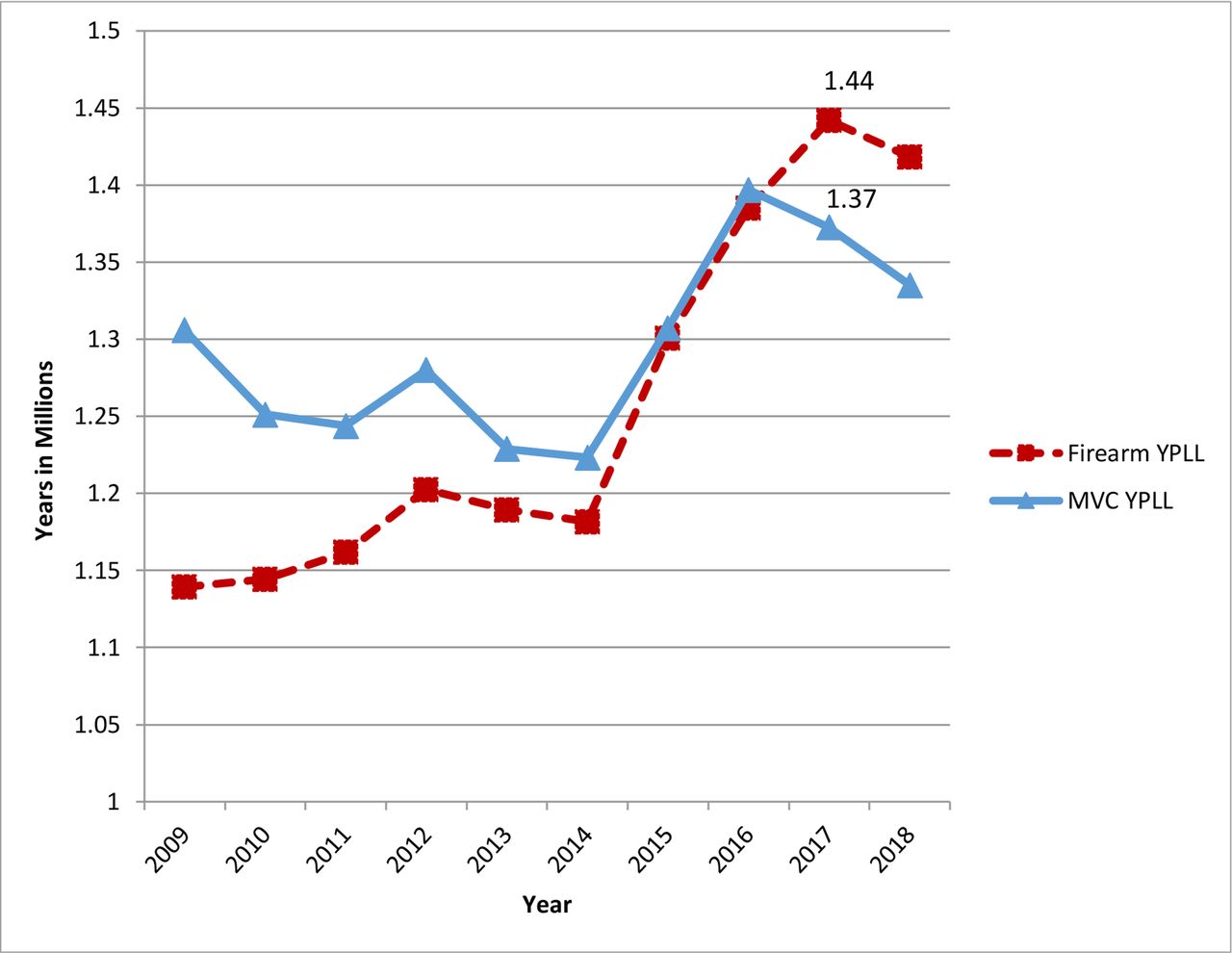
Cumulative YPLL. MVC, motor vehicle crash; YPLL, years of potential life lost.

Annual percent change—firearms versus MVC. MVC, motor vehicle crash.
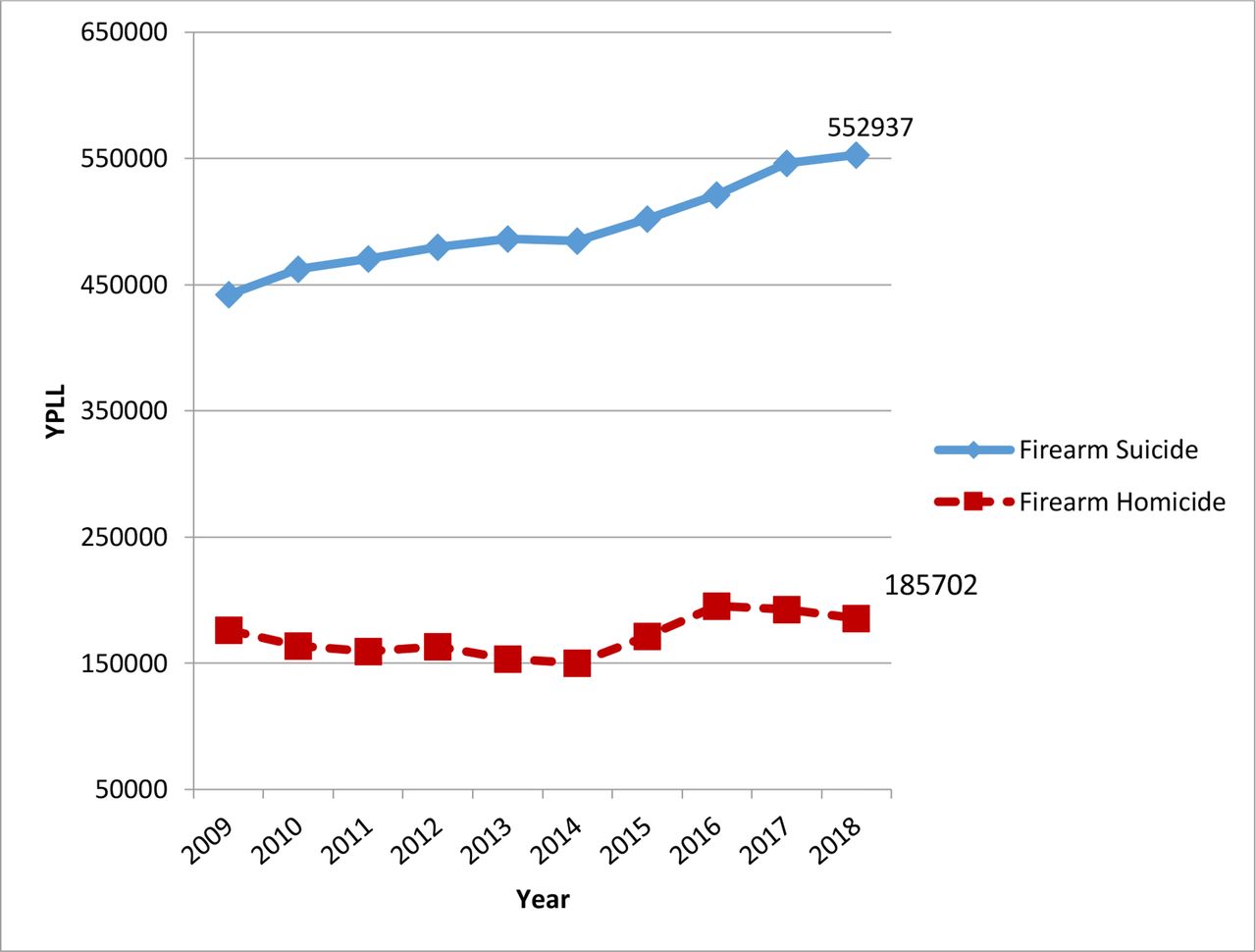
Throughout the 10-year study period, firearm suicide and firearm homicide deaths both increased (figure 3). Suicide by firearm accounted for 18 735 trauma deaths in 2009 and increased to 24 432 deaths in 2018. This increase in firearm suicides led to an increase in YPLL with 571 720 years lost in 2009 compared with 741 869 YPLL in 2018. Firearm homicide also increased from 11 493 deaths in 2009, to 13 958 deaths in 2018. This resulted in 633 656 YPLL in 2018, which is an additional 80 396 YPLL compared with 2009 (554 260 YPLL). Legal firearm intervention deaths, which is defined as a firearm death inflicted by the police or other law enforcement agents acting in the line of duty, were relatively constant, with 333 deaths in 2009, and 539 deaths in 2018. This accounted for 22 702 YPLL in 2018.

Total firearm deaths by mechanism, 2009–2018.
Firearm death: populations affected
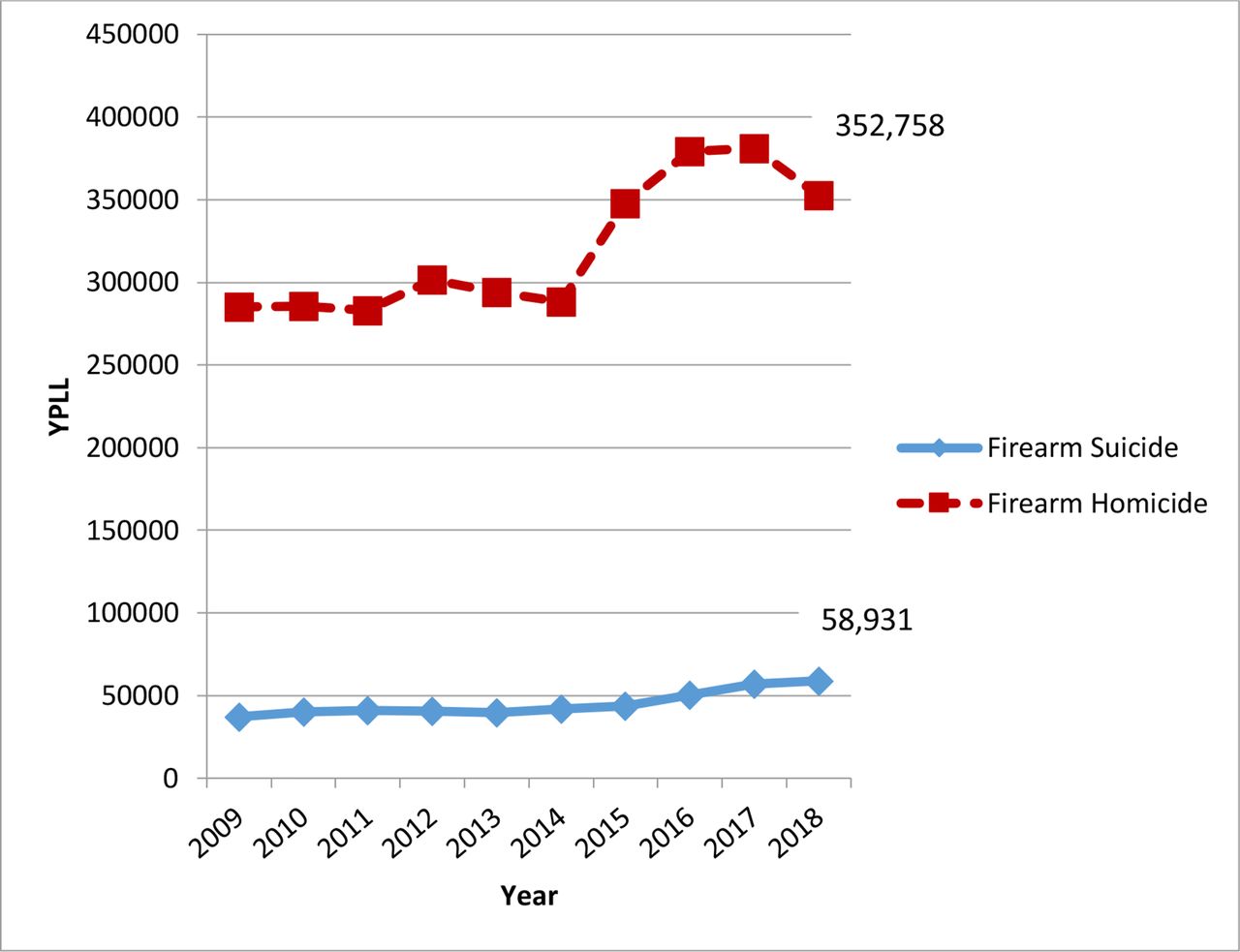
Males comprised the majority of the 38 929 firearm deaths reported by the CDC in 2018 with 33 258 deaths (85.4%). Firearm suicide was highest among white males in 2018 comprising 49.3% of total firearm deaths, whereas firearm homicide was highest in the black male population, comprising 18.3% of total firearm deaths. During the 10-year period, white males had a total of 4.95 million YPLL due to firearm suicide compared with 1.7 million YPLL due to firearm homicide (figure 4). Middle-aged and older white males had significantly higher rates of firearm suicide, with 30 774 deaths in the age group 45–54 years, 31 092 deaths in the age group 55–64 years, and 46 078 deaths in the 65 years and older age group during the course of the 10-year period. The total number of deaths from firearm suicide for white males under the age of 45 years was 62 430 during the same period—46% less than those 45 years and older. The 4.95 million YPLL due to firearm suicide in white males represent over one-third of all YPLL related to firearm deaths. The APC of white male suicides during the study period was 0.43 (p=0.001).

White male firearm suicide versus homicide YPLL. YPLL, years of potential life lost.
Black males had a total of 3.2 million YPLL due to firearm homicides compared with 0.4 million YPLL due to firearm suicide during the study period (figure 5). There were a total of 63 414 firearm homicide deaths, with the majority of firearm homicide deaths in the 15–24 (24 601 deaths) and 25–34 (21 599 deaths) age groups. The APC of black male suicides during the 10-year period was 0.79 (p<0.001).

Black male firearm suicide versus homicide YPLL. YPLL, years of potential life lost.
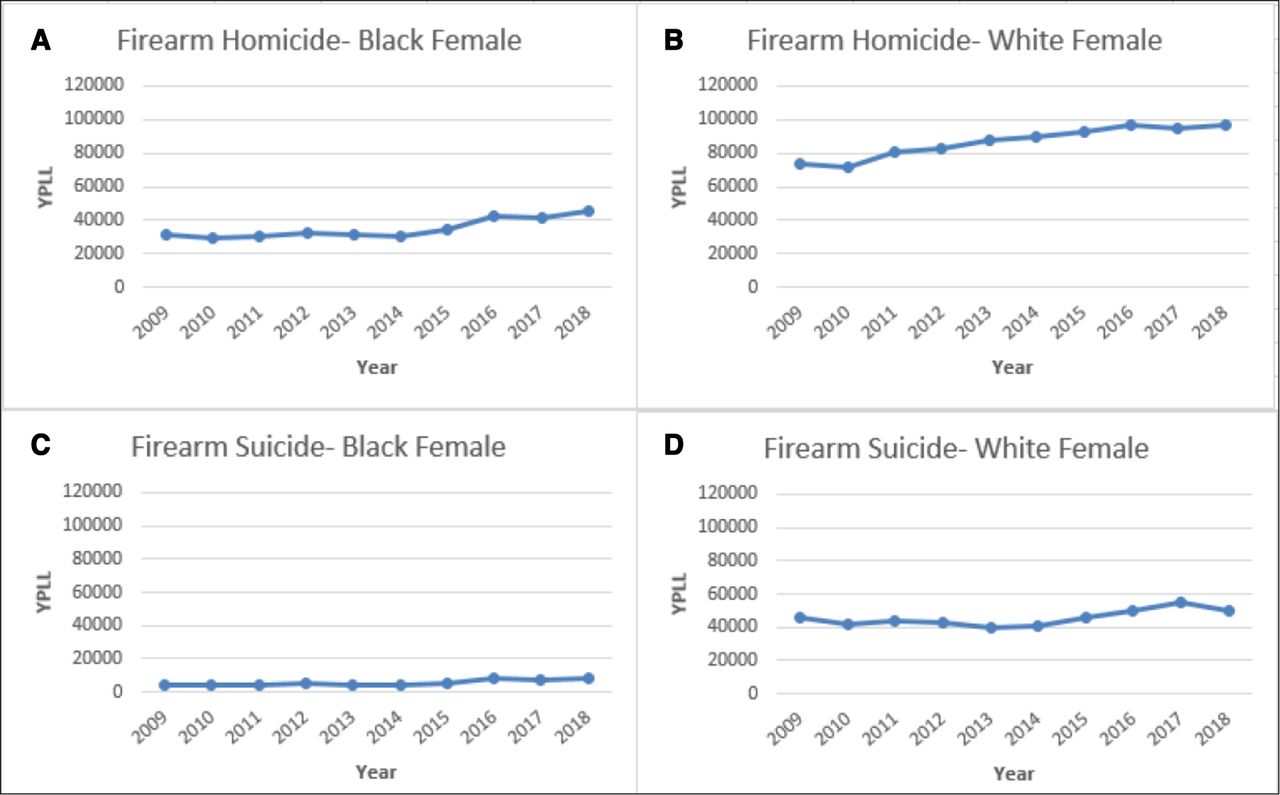
White females had a total of 1.3 million YPLL secondary to firearm deaths throughout the study, with 867 890 YPLL and 456 203 YPLL for firearm suicide and homicide, respectively. During this time, firearm suicides increased by 31.5%, whereas homicides increased by 9.9%. Black females had a higher YPLL secondary to firearm homicide compared with firearm suicide—347 941 YPLL vs 55 799 YPLL (figure 6).

Firearm death, YPLL females. YPLL, years of potential life lost.
Regionally, the South had the highest YPLL due to firearms with 5.7 million years lost, followed by the Midwest, West, and Northeast (figure 7). The Northeast was the only region during this time period for which homicide contributed to a higher number of YPLL as opposed to suicide (700 000 vs 612 000). In 2018, suicide was responsible for higher YPLL than homicides in all regions.

Firearm homicide/suicide by region, 2009–2018. YPLL, years of potential life lost.
Discussion
There has been a significant shift in the USA with respect to the cause of trauma-related deaths as well as the epidemiology of populations affected. Death due to trauma yields a higher YPLL than most other causes of mortality as trauma patients are typically younger at time of death.1 Although the predominant cause of YPLL due to trauma deaths was previously attributed to MVC, the paradigm has shifted as we now see that firearms are the leading cause of YPLL since 2017. Although the total number of deaths in the black male population due to firearm homicide was significantly less than the total number of white male suicides during the study period (63 414 vs 170 388), the younger age of these black male homicide victims increases the overall YPLL. For each death, on average, black male homicides accounted for 50.5 YPLL, whereas white male suicides accounted for 29.1 YPLL.
Previous studies have shown that firearm ownership, mass shootings, injuries, and death are more of a problem in the USA as compared with other developed countries.3 Of more than 1 billion estimated firearms worldwide, 85% of the firearms are in civilian hands, whereas only 13% are in military arsenals.4 The USA alone is estimated to have 393.3 million firearms compared with 16.8 million in Mexico and 12.7 million in Canada.4 These numbers, however, may grossly underestimate the number of firearms as these are estimates and there is a significant number of unregistered firearms, many of which are acquired through illegal trafficking.5 6
Although the WHO states that suicides are preventable, it is not realistic that all suicides are preventable.7 The cause of suicide is multifactorial with mental illness often playing a major role in victims. Studies have shown that major depressive disorders are present in approximately 50% of the suicide victims, and that financial, relationship, and other outside stressors are frequently present in these individuals.8 These stress-inducing variables of life can accumulate, with many elderly adults reporting feelings of loneliness and isolation.9 Loss of a job or retirement with subsequent reliance on social security income has been cited as a major stressor in older adults as the loss of financial resources causes individuals to perceive themselves as a burden to family members and society.10 This is further compounded in individuals who identify themselves as their job, as the loss of their job further exacerbates lack of kinship and inclusion.10 The availability of firearms makes the impulsive behavior somewhat less reversible, and the effectiveness of firearms makes the attempts often successful. Studies investigating fatality rate by suicide method reveal that firearms are 89.6% effective compared with other methods of suicide.11 12 Up to 70% of suicides are based on impulsive behavior and suicide attempts are typically made after less than 3 hours of contemplation.12
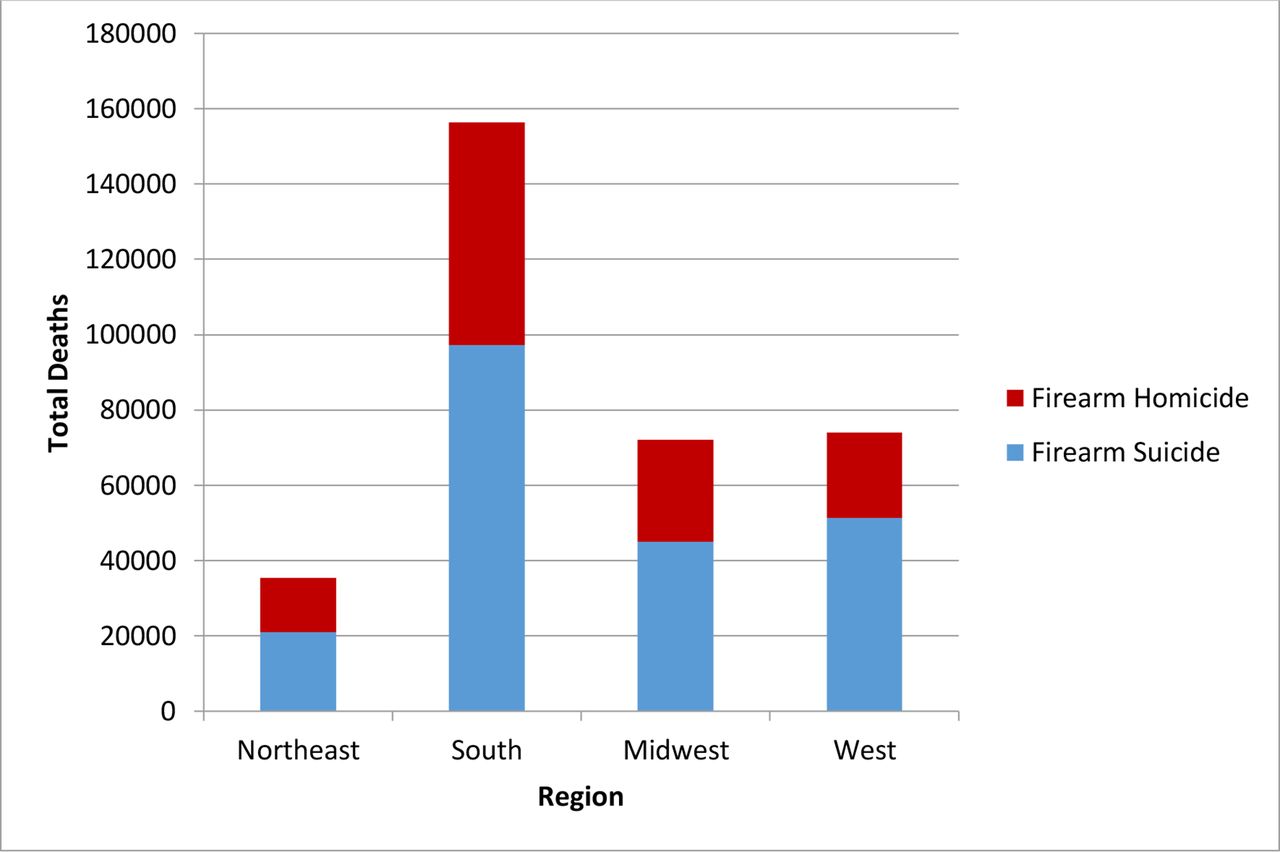
Regionally, the South had the highest number of firearm deaths with 157 907 deaths during the 10-year period, whereas the Northeast had the lowest number of firearm deaths with 35 789 (figure 8). All regions had a higher total number of firearm deaths related to firearm suicide as opposed to homicide; however, despite 6856 more suicide deaths in the Northeast, the YPLL was higher for firearm homicides compared with suicides (700 639 YPLL vs 612 598 YPLL). The Bureau of Alcohol, Tobacco, Firearms, and Explosives releases an annual statistical update regarding firearms commerce in the USA which has consistently revealed that the Southern region of the USA has the most number of registered firearms.13 In 2018, there were over 3 million registered firearms in the South, with Texas and Florida as the two states with the highest number of registrations in the USA. Although the number of firearms within a state or region will not fully predict suicide, homicide, or violent crime rates, availability of firearms should be taken into account when discussing trauma and injury prevention strategies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
YPLL by region, 2009–2018. YPLL, years of potential life lost.
The demand for total freedom and the second amendment have resulted in high access to firearms in this country and this is undisputable. The main argument is that the right to bear arms to prevent injury or to defend against aggressors may result in a small number of preventable deaths is a plausible theory, however, the data reveal that the resulting access to firearms has equated to magnitudes of death due to firearm suicides in the same individuals demanding access to firearms. Effective suicide prevention efforts should include limiting access to all methods of suicide—including firearms—for at-risk populations.
Limitations
Within the CDC WISQARS database, firearm deaths are currently only categorized into three different mechanisms: homicide, suicide, and legal firearm interventions. The legal firearm interventions remained constant throughout the study period and were not statistically significant in comparison with the YPLL secondary to homicide and suicide; therefore, it was only briefly mentioned in our article. Although the data obtained for this study are publicly available through the CDC website, there has been no previous systematic analysis and presentation of these data as has been performed in this study. This study summarizes the available data and therefore cannot fully determine the etiology behind the changes in YPLL caused by firearms without demonstrating bias.
Conclusions
YPLL due to firearms in the USA has continued to rise since 2009. Although deaths from MVC used to be the single largest cause of traumatic death and YPLL in the USA, deaths and YPLL by firearms have now surpassed it. Suicide is responsible for the most YPLL due to firearm deaths, and continues to increase in the USA at an alarming rate. The predominant populations that are affected by firearm deaths are older, white males secondary to suicide, and younger black males secondary to homicide. More resources should be redirected and allocated to these at-risk populations to decrease this potentially preventable cause of death and years of life lost.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants. Due to the de-identified nature of the data set, informed consent and IRB approval were waived.
Acknowledgments
The authors are grateful to Jonathan Butler from the New York Medical College Department of Statistics for help with analyzing data collected.
Supplementary materials
Press release
Footnotes
Contributors PR and KP contributed to planning, conception and design, and editing. RL was responsible for planning and editing. JK did the planning, reporting, acquisition of data, analysis and preparation of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.