Article Text

Statistics from Altmetric.com
A patient in their 20s presented to the emergency department after a motor vehicle collision. The patient was noted to be tachycardic, with systolic blood pressure in the 90s. The initial Glasgow Coma Scale (GCS) score was 7 (E1, V2, M4). The patient was intubated for low GCS and transfused two units of packed red blood cells with improved vital signs. Whole-body CT was obtained and found to have subarachnoid hemorrhage and subdural hematoma with multiple facial fractures. CT of the chest and abdomen demonstrated Chance fracture of the thoracic spine at T9–10 level and a small mesenteric hematoma. Additional X-rays noted bilateral radial fractures and right femur fracture. The patient was admitted to the surgical intensive care unit (ICU) for hemodynamic monitoring, serial laboratory evaluation with abdominal examination, and further management of multisystem injuries. After stable head CTs, pharmacologic venous thromboembolism prophylaxis was initiated on hospital day 3. Spinal fusion was performed on hospital day 5, followed by internal fixation of extremity fractures on hospital day 6.
On hospital day 7, the patient was taken for MRI of the cervical spine for the evaluation of ligamentous injuries; however, it was aborted when the patient was found to be severely agitated and tachycardic after being transferred to the MRI table. During the transport back to the surgical ICU, the patient became extremely bradycardic and lost carotid pulses. Cardiopulmonary resuscitation (CPR) was immediately initiated by the critical care transport team. On arrival to the surgical ICU, advanced cardiac life support was initiated and return of spontaneous circulation was achieved, although the patient remained profoundly hypotensive requiring multiple vasopressors and intermittently required CPR for pulseless electrical activity. A bedside transthoracic echocardiography performed by a surgical intensivist demonstrated severe dilation and hypokinesis of the right ventricle, consistent with right ventricular strain likely due to massive pulmonary embolism (PE) (figure 1, online supplemental video).
Supplementary video
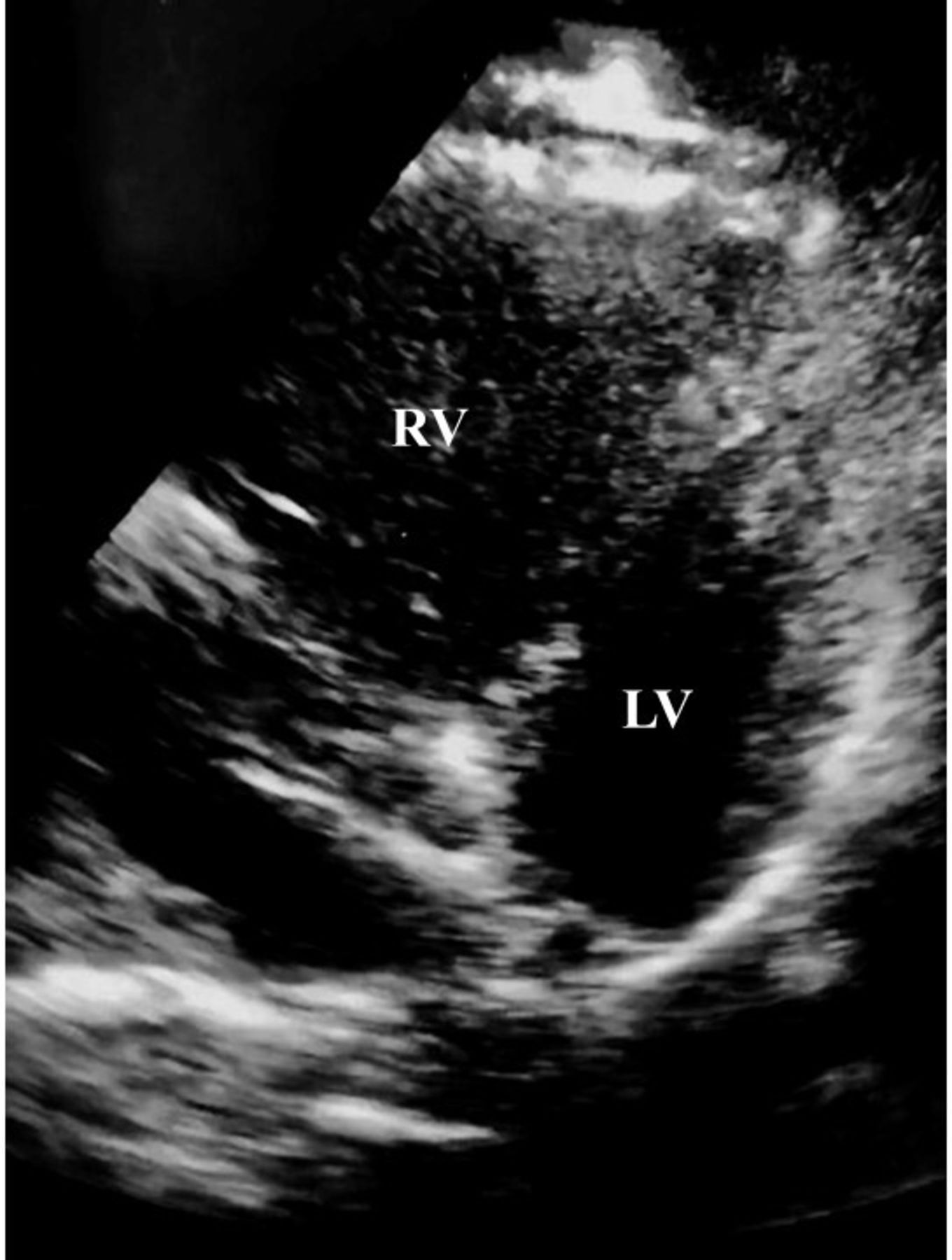
Bedside transthoracic echocardiography demonstrating dilated RV suggestive of right ventricular strain. LV, left ventricle; RV, right ventricle.
What would you do?
Continue CPR until the patient is stabilized for CT pulmonary angiography.
Continue CPR and initiate systemic thrombolytic therapy.
Place the patient on venoarterial extracorporeal membrane oxygenation (VA-ECMO) and consider catheter-directed thrombectomy.
What we did and why
3. Place the patient on venoarterial extracorporeal membrane oxygenation (VA-ECMO) and consider catheter-directed thrombectomy.
Given the patient’s known traumatic brain injuries (TBIs), systemic thrombolysis for massive PE was deemed high risk for hemorrhagic complications. While CPR was being performed, the patient was emergently started on VA-ECMO via right groin access (23 Fr venous and 17 Fr arterial cannulas) (figure 2). Once hemodynamic status became stabilized with VA-ECMO, the patient was taken to the angiography suite urgently for catheter-directed thrombectomy after discussion with the neurosurgical service who agreed that anticoagulation therapy with heparin infusion on VA-ECMO was an acceptable risk. On pulmonary angiogram, large clot burden was noted in the left main pulmonary artery extending into segmental branches. Mechanical thrombectomy was performed using a clot aspiration device with improvement of blood flow in the left main pulmonary artery on repeat angiograms (figure 3). The right-sided angiogram demonstrated a large clot in the main pulmonary artery with extension into the superior branches, and thrombectomy was also performed.
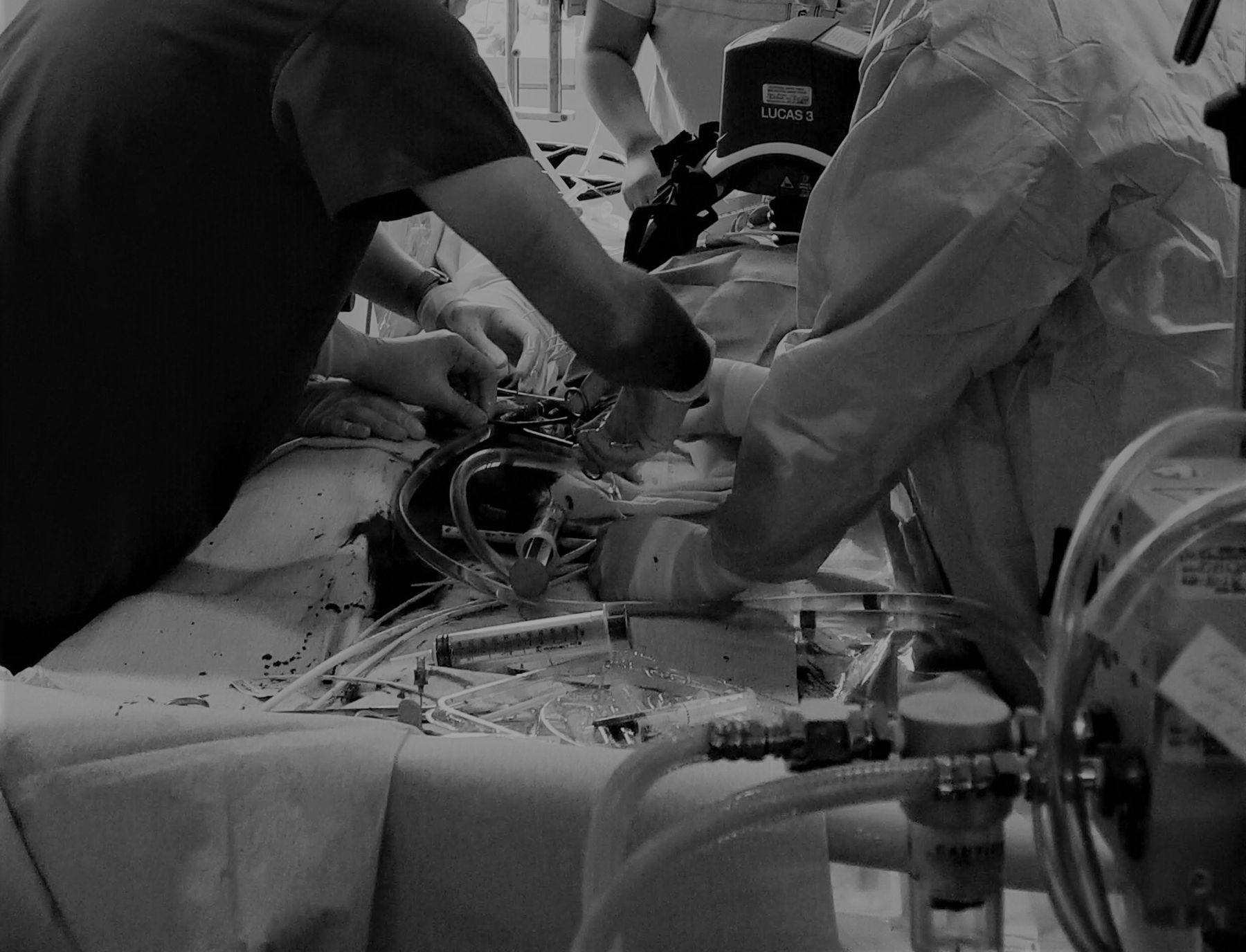
Cannulation for VA-ECMO was performed during ongoing CPR. CPR, cardiopulmonary resuscitation; VA-ECMO, venoarterial extracorporeal membrane oxygenation.

{kind=link}
{kind=link}
{kind=link}
Blood clot removed from the pulmonary artery during catheter-directed thrombectomy.
After the procedure, the patient was taken back to the surgical ICU and continued on VA-ECMO. A repeat head CT after the initiation of anticoagulation therapy demonstrated no evidence of worsening hemorrhagic TBI. With significant improvements in the patient’s hemodynamic status, ECMO was weaned during the course of 5 days and the patient was successfully decannulated on hospital day 12. Although a tracheostomy was required for liberation from the ventilator and renal replacement therapy for acute kidney injury, the patient’s care was eventually transitioned to an acute rehabilitation hospital on hospital day 34. The patient returned to our trauma surgery clinic 3 months later and was noted to have made a full functional recovery.
Although most of the published trauma experience with ECMO is venovenous-ECMO, little is known about indications for the use of VA-ECMO in trauma patients. VA-ECMO by nature provides cardiac as well as pulmonary support. This potentially allows adjustments in circulatory flow to allow for repair of complex cardiothoracic injuries and can be indicated for post-traumatic cardiogenic shock in patients with pre-existing cardiac dysfunction. Particularly, in patients who sustained severe chest trauma requiring pneumectomy, VA-ECMO may allow for clinically significant offloading in the setting of acute right heart failure. That same principle was likely the reason for the success of VA-ECMO in the aforementioned patient with massive PE. This technique should be used cautiously in trauma patients with significant coagulopathy, ongoing concern for severe TBI or solid organ injuries, as VA-ECMO can exacerbate the coagulopathy and result in life-threatening hemorrhage.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @reyshenry
Contributors Study concept and design—RH, JG, BF, MM, AM and KM. Data collection and analysis—RH, JG, BF, MM, AM and KM. Writing—RH and JG. Critical revision—BF, MM, AM and KM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.