Article Text

Abstract
Objectives Pruritus is a common and often distressing complication after a burn injury. The purpose of this review is to explore the efficacy of drugs classically used to treat neuropathic pain in the management of pruritus after burn injury.
Methods A systematic literature search of medical databases was conducted to find studies investigating drugs listed in the National Institute for Health and Care Excellence (NICE) guideline (CG173, “neuropathic pain in adults”) for the management of pruritus after burn injury in patients of any age. Controlled studies were stratified by the drug class studied and their risk of bias before conducting meta-analysis. A narrative review of case series or observational studies was presented. Severity of pruritus at any time point, with all quantitative and qualitative measures, was included.
Results Fifteen studies were included in the final analysis, 10 investigated the use of gabapentinoids, 4 studied doxepin, and 1 local anesthetic agents. Meta-analysis of three randomized controlled trials (RCTs) demonstrated that the use of gabapentinoids was associated with an improvement in mean VAS (Visual Analog Scale) 0–10 scores of 2.96 (95% confidence interval (95% CI) 1.20 to 4.73, p<0.001) when compared with placebo or antihistamine. A meta-analysis of four RCTs investigating topical doxepin showed an improvement in mean VAS scores of 1.82 (95% CI 0.55 to 3.09, p<0.001). However, when excluding two studies found to be at high risk of bias, no such improvement was found (−0.32, 95% CI −1.64 to –0.99, p=0.83).
Conclusion This study suggests that gabapentinoids are beneficial in the management of burn-related pruritus. There is a lack of evidence to suggest that doxepin is an effective treatment. Topical local anesthetic agents may be safe and beneficial, but studies are scarce.
Level of evidence Systematic review, level II.
- burn
- patient outcome assessment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Burn injuries are acute traumatic insults. However, even with successful treatment, it is increasingly recognized that such injuries have far reaching and long lasting consequences.1 After even relatively minor burns, patients experience a persisting inflammatory response and immune dysfunction,2 leading to an increased risk of cardiovascular disease,3 cancer,4 infections,5 and early death.6 Although seemingly minor in comparison, pruritus is an additional long-term consequence that is common and significantly affects the quality of life of patients surviving burns.
There is a high prevalence of sensory disorders such as chronic pain, paresthesia, and pruritus in burns patients.7 The incidence of pruritus has been reported to be 93% at hospital discharge,8 67% to 73% at 2 years,8 9 and 44% at 4 years to 10 years.8 9 Factors such as deep dermal injury, greater total body surface area (TBSA) burned, an increased number of surgical interventions, female gender, and symptoms of post-traumatic stress disorder increase the risk.9
Achieving meaningful control of pruritus symptoms can be difficult and only a paucity of clinical trials have evaluated interventions.10–12 Histamine produced both from mast cell degranulation and as a by-product of collagen formation is thought to be a major contributor to the development of pruritus. A survey performed in the UK showed that over 90% of burns units used antihistamines as the first-line treatment.13 However, the involvement of various other peripherally acting pruritogens and the pathophysiological changes that occur more centrally mean that antihistamine monotherapy is often inadequate, especially in chronic pruritus.14
Although the neuronal pathways involved in the perception of pain have been extensively explored, the equivalent neuroanatomical basis for pruritus remains incompletely understood. A subset of afferent slow conducting C-fibers are activated by pruritogens including histamine, acetylcholine, calcitonin gene-related peptide, bradykinin, leukotrienes, prostaglandins, and various cytokines.15 Pain and pruritus share a similar neurophysiological basis, thought to be a consequence of evolutionary changes15 and after activation, these C-fibers conduct impulses in a similar manner to the pain pathway via the dorsal root ganglion, spinothalamic tract, thalamus, and then to various higher centers including the somatosensory cortex.14 15
Similarities have been drawn between chronic pruritus and neuropathic pain. Clinical features such as hyperknesis and alloknesis mirror the hyperalgesia and allodynia seen in neuropathic pain secondary to peripheral and central sensitization.14 16 17 Such pathological processes are reflected in one classification of pruritus, as pruritogenic, neuropathic, neurogenic, and psychogenic.16
The objective of this narrative, systematic review is to evaluate the effectiveness of agents used in neuropathic pain, as detailed by the National Institute of Clinical Excellence (NICE),18 in the management of pruritus after a burn injury.
Methods
Registration
This review was registered on the PROSPERO Register of Systematic Reviews, ID number CRD42020164777. The PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses) guidelines for the conduct of systematic reviews were followed throughout.19
Eligibility criteria
Articles were included that investigated the management of pruritus in patients of any age that had sustained a burn injury with the use of neuropathic agents that are listed in the NICE guideline (CG173) “neuropathic pain in adults: pharmacological management in non-specialist settings”.18 Given the likelihood of several studies being observational in nature, no restrictions were made regarding the use of a control group. Animal studies, human volunteer studies, literature reviews, and conference abstracts were excluded, otherwise no restrictions on the type of study were made.
Search strategy
Three databases, MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials (CENTRAL), were searched with no time period or language restrictions (last accessed January 7, 2021). The search strategies for each database can be found in the online supplemental material.
Supplemental material
Study selection
After amalgamation of search results from the three sources and removal of duplicates, two authors (CM, WN) independently conducted a title review, abstract review, and then full article review to select articles for inclusion. Any disagreement between the two reviewers was resolved by a third reviewer (LP). The references of all titles included in the data analysis were screened for further articles to be included.
Data extraction
Data were extracted by CM using a predefined spreadsheet which included study design, patient demographics, interventions, and outcomes. In the event of missing data, study investigators were contacted.
Outcomes measured
The outcome of interest was the severity of pruritus at any time point. No specific restrictions were used, with all quantitative severity scales, qualitative measures, and questionnaire methods of assessment included. For inclusion in meta-analysis, any quantitative scales were converted to an 11-point continuous scale and the mean difference between groups reported.
Risk of bias assessment
Each included study was assessed independently by CM and WN using a specific risk of bias tool. The RoB2 (the updated Cochrane risk of bias tool) was used for randomized controlled trials (RCTs), and ROBINS-I tool for non-randomized studies. The quality of evidence for the outcomes of interest were assessed using the GRADE (Grading of Recommendations, Assessment, Development and Evaluations) system.20
Data synthesis
Studies were categorized based on the intervention studied, specifically the neuropathic agent of interest, and are presented in tables for each class of agent. In controlled studies using the same drug or class of drug (eg, gabapentinoids) and comparable outcome measures (eg, a continuous variable such as visual analogue scale), results were collated using a random-effects meta-analysis, and two-sided p values and 95% confidence intervals were calculated. Heterogeneity was expressed as an I2 statistic for studies included in meta-analyses. No specific sensitivity analyses were performed; however, studies were stratified by their risk of bias and meta-analyses were conducted separately for those at high and low/moderate risk and then combined.
For agents where only case series or observational studies were available, a narrative review of the study findings was undertaken.
Numeric data were extracted from graphs if the required data were not included elsewhere in an article using Graphgrabber (V.2.0.2, Quintessa Ltd, Oxfordshire, United Kingdom). Meta-analysis was conducted using the software package Revman (V.5.4.1, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration).
Results
Study inclusion
The literature search returned 5469 articles after removal of duplicates. The PRISMA flowchart (see online supplemental figure S1) details the selection process. One article required translation from Chinese.

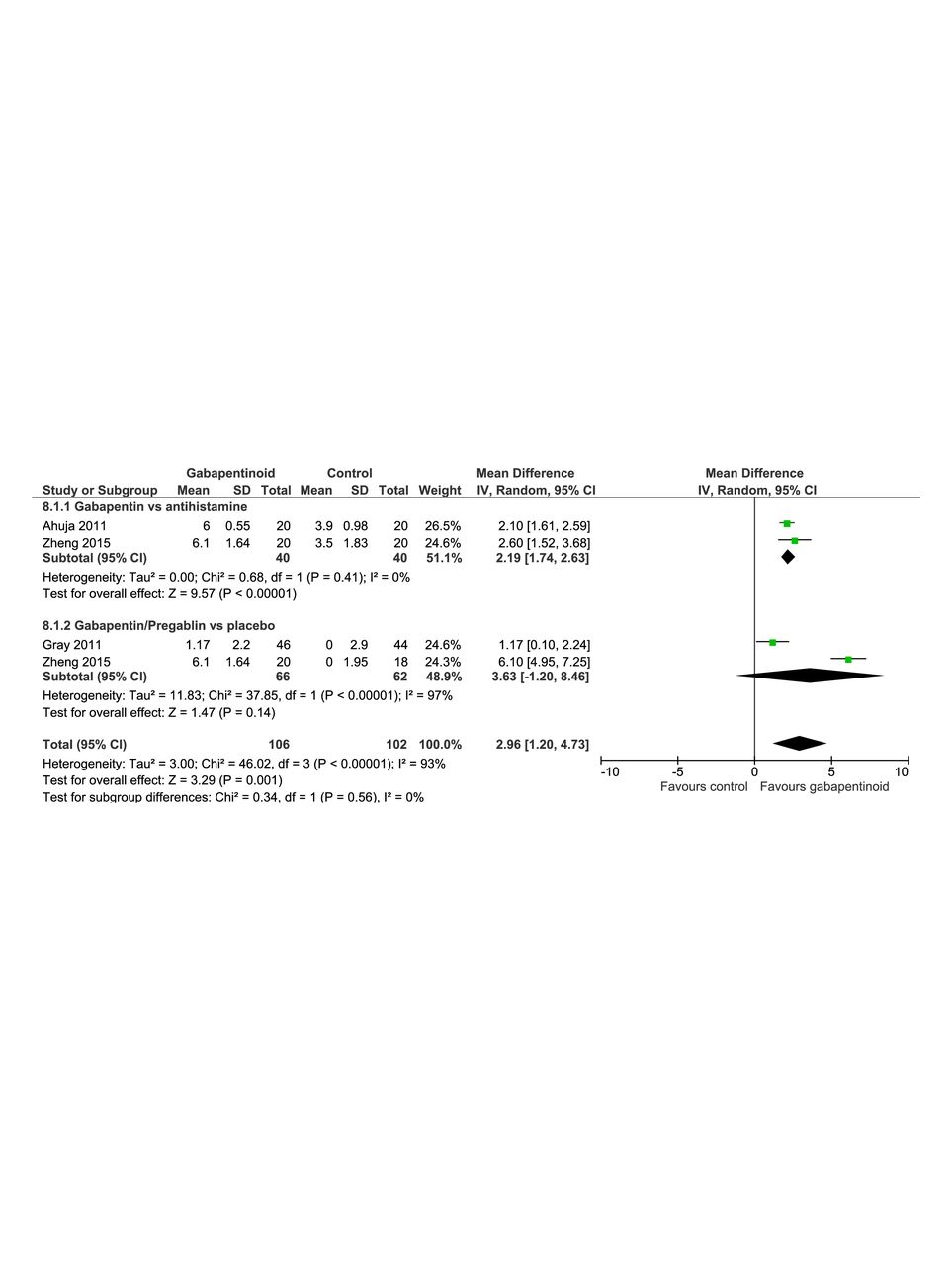
Forest plot showing the reduction in mean VAS (Visual Analog Scale) in each treatment arm, comparing gabapentinoids with controls. 95% CI, 95% confidence interval.
Three main classes of neuropathic agents were investigated in the articles included in the final analysis:
Gabapentinoids (gabapentin and pregabalin).
Topical doxepin.
Topical local anesthetic agents.
Gabapentinoids
Ten articles21–30 investigated gabapentinoids in the management of pruritus after burn injury. Four studies were RCTs (table 1) and six were observational studies with varying methodology (table 2).
Randomized controlled trials of gabapentinoids
Observational studies of gabapentinoids
Randomized controlled trials
Three RCTs provided sufficient data to perform meta-analyses. Two studies21 30 included groups comparing gabapentin to a control arm given an antihistamine, cetirizine. Both studies demonstrated a mean reduction in pruritus severity, measured on 0 to 10 VAS (Visual Analog Scale) of around 6 points in the gabapentin group over the 28-day trial period. Those treated with cetirizine had a reduction of 3.9 and 3.5. The meta-analysis demonstrated a greater reduction in VAS score of 2.19 (95% CI 1.74 to 2.63) with gabapentin compared with cetirizine (figure 1).
Studies by Gray et al24 and Zheng et al30 included cohorts treated with a placebo. Gabapentinoids differed between studies, with Gray et al using pregabalin 150 o 600 mg daily and Zheng et al using gabapentin 600 mg daily. Meta-analysis demonstrated an improvement in 0 to 10 itch severity score of 3.63 (95% CI −1.20 to –8.46) when a gabapentinoid was used in comparison to placebo (figure 1).
Combination of the above subgroup meta-analyses demonstrated an improvement in VAS of 2.96 (95% CI 1.20 to 4.73) when gabapentinoids are compared with control.
Although pruritus was not reported as a primary outcome in the study by Gray et al, it did report elements of the NPS (Neuropathic Pain Scale) including a 0 to 10 scale of pruritus severity. The effect of pregabalin on pruritus appeared much smaller than that demonstrated by the other studies included in the meta-analysis, with an improvement in mean scores of 1.17 (95% CI 0.10 to 2.24).
A further RCT was not included in the meta-analysis.22 Although the percentage changes in mean VAS scores were reported, the analysis did not include sufficient information regarding the distribution of the sample data, such as SD, to allow inclusion.22 This trial did, however, demonstrate a 78.9% fall in mean pruritus VAS scores in the group given pregabalin in comparison to 33.3% in the placebo group when focusing on patients with the most severe initial VAS scores (9 to 10). The placebo and antihistamine groups in this study suffered high dropout rates, however, potentially reflecting inadequate symptom relief.
Both RCTs conducted by Ahuja et al21 22 also included groups given a gabapentinoid and antihistamine in combination but found no additional benefit when compared with gabapentinoid alone.
Observational studies
Of the six observational studies (table 2), three were considered to be at serious risk of bias, two at moderate risk, and one to be of low risk (see online supplemental table S2). Sources of possible bias were primarily outcome measurements, which were often generated by research staff rather than patient reported.
Mendham et al27 reported improvements in itch intensity when gabapentin was used in children with persisting itch despite treatment with antihistamines. Unfortunately, this outcome was measured solely on subjective reporting by nursing staff, parents, and children.
Goutos et al23 investigated the use of two antipruritic protocols, with early or late introduction of gabapentin as part of incremental pharmacotherapy. In 41.5% of patients given gabapentin as the first-line agent, satisfactory itch control was achieved, in comparison to just 10% when cetirizine was used first line.
Zachariah et al29 reported improved mean itch severity scores when gabapentin was given to pediatric and adult patients complaining of pruritus with inadequate relief on antihistamines and emollients. On a scale ranging from 7 to 21, mean itch severity scores fell from 13.35 to 8.36 within 1 month of treatment and this effect was sustained for the 6-month follow-up period.
Kaul et al25 conducted a retrospective review of drug prescribing data of 136 mainly pediatric patients given gabapentin, pregabalin, or a combination of both for pruritus or neuropathic pain. Although 91.4% of patients had an adequate response to treatment with gabapentin alone for pruritus, the measure of this outcome relied on adequate documentation in the patient medical notes and there was no comparator or control group.
Nieuwendijk et al28 investigated the incidence, severity, and risk factors associated with pruritus in pediatric burn injury, then went on to describe pharmacotherapies used with 17.9% having received gabapentin. Unfortunately, as the study was principally designed to explore factors associated with pruritus, no conclusions could be drawn on the effectiveness of the pharmacological therapy.
Kneib et al26 conducted a retrospective cohort study investigating the use of a neuropathic pain and pruritus protocol. Patients were started on incremental doses of gabapentin if itch scores remained greater than 4 (on 0 to 10 NRS) despite initial treatment with cetirizine. Comparison was made between various groups including pre-protocol and post-protocol introduction as well as patients that received gabapentin early (<72 hours), late (>72 hours), or not at all. There was no difference in itch severity odds ratios between any group at discharge through to 24 months.
Topical doxepin
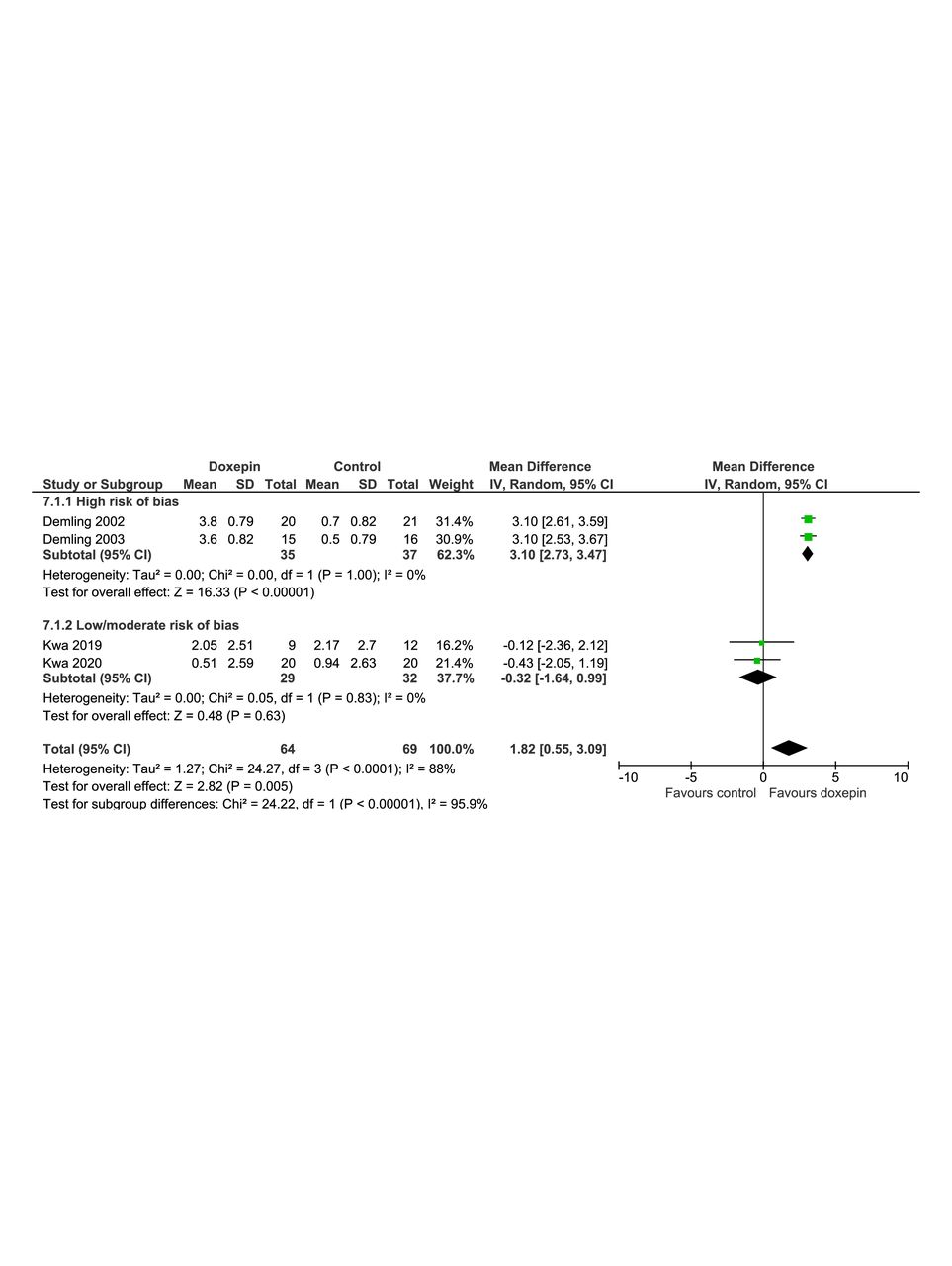
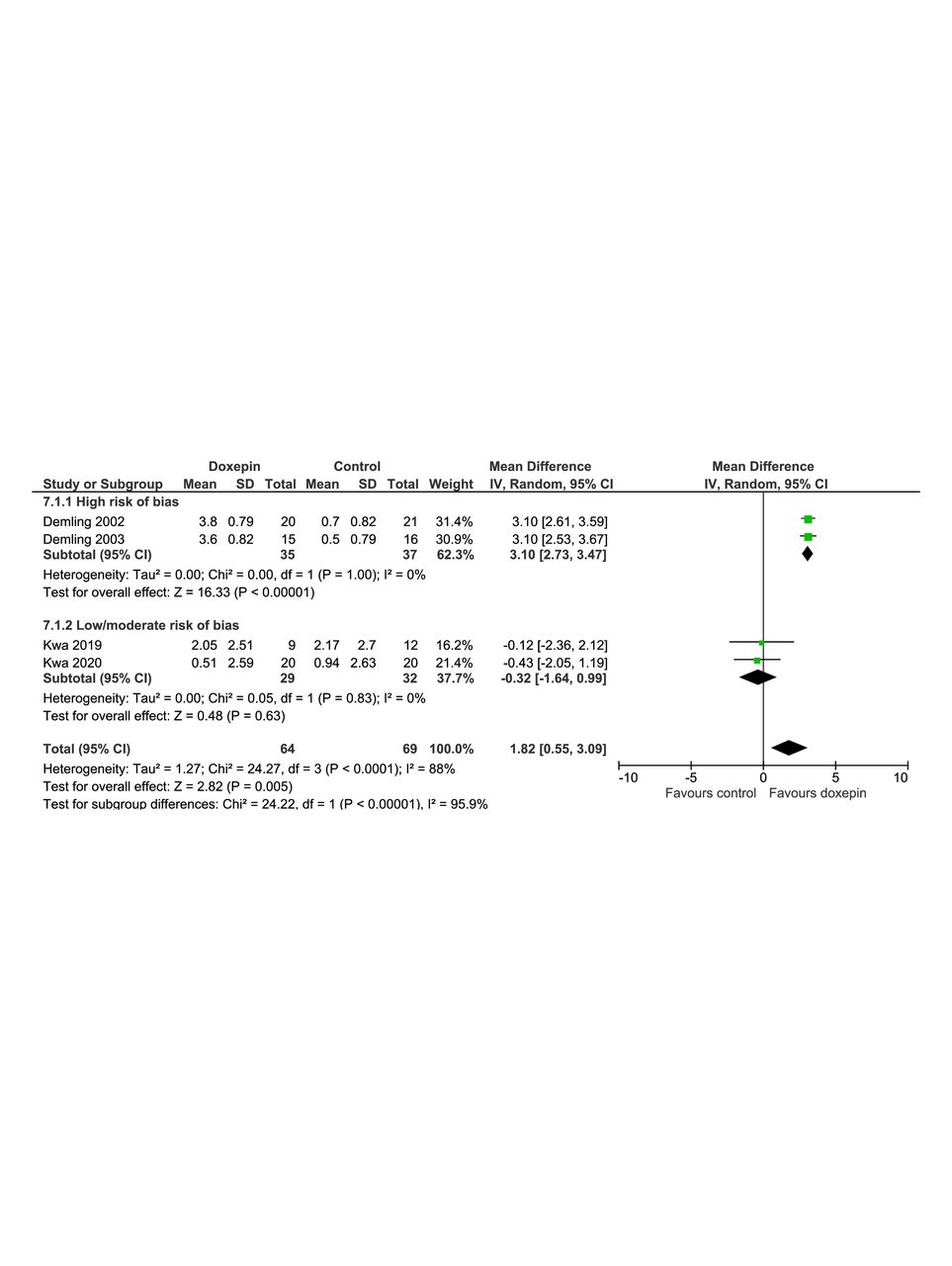
Doxepin is a tricyclic antidepressant agent, but due to its potent antihistaminergic activity, is used topically to treat pruritus in eczema. Four studies31–34 investigated the use of topical doxepin on pruritic burn scars in adult patients (table 3). Given significant differences in both the results of these studies and the risk of bias assessments, meta-analyses are presented on studies at high risk and low/moderate risk of bias separately and then combined (figure 2).
Studies of topical doxepin
{kind=link}
{kind=link}
Forest plot showing the reduction in mean VAS (Visual Analog Scale) in each treatment arm, comparing topical doxepin with controls. 95% CI, 95% confidence interval.
Demling et al performed two single center RCTs comparing topical doxepin to standard care.31 34 The results of both trials showed a marked improvement in itch VAS scores at all time points compared with standard care. The results of a meta-analysis including these studies demonstrated an improvement in mean VAS score of 3.10 (95% CI 2.73 to 3.47). Both of these studies were found to be at high risk of bias from a lack of blinding and unclear randomization methods (see online supplemental table S1). Additionally, the control arm of “standard care” involved titration of oral antihistamines that all participants were already taking prior to enrollment rather than introduction of another therapy or placebo.
Kwa et al conducted two multicenter, blinded RCTs investigating the use of doxepin cream. The first study32 showed no difference in itch intensity at any time point between doxepin cream and the control group. Due to difficulty recruiting to the trial and a high dropout rate, this study was underpowered. A second study33 addressed these recruitment issues using a cross-over study design comparing doxepin against placebo without the inclusion of an antihistamine. Again, this demonstrated no difference in itch intensity between groups. A meta-analysis of both articles by Kwa et al (figure 2) using outcome data at 14 days showed no difference in changes in VAS scores in comparison to placebo or antihistamines, with a mean VAS change of −0.32 (95% CI −1.64 to 0.99).
All four studies investigating doxepin have been included in the final meta-analysis (figure 2) with no adjustment made for the risk of bias assessment. This demonstrated a reduction in mean VAS of 1.82 (95% CI 0.55 to 3.09). This result should be interpreted with caution as, when assessed using the GRADE tool, was found to be of very low quality, principally due to the high risk of bias (see online supplemental table S3).
Topical local anesthetics
One study35 investigated the use of a topical local anesthetic agent in the management of pruritus after burn injury in children 1 to 5 years old. EMLA cream, a mixture of prilocaine and lidocaine, was applied to healed partial thickness burns with persisting pruritus in five patients. The main purpose of this study was to assess the safety and pharmacokinetics of this therapy.
This study was performed over 3 days, with the first 2 days acting as a control for the treatment being implemented on day 3. There was an improvement in itch intensity as measured by a VAS and number of pruritic episodes. Owing to the young age of the children, outcome measures were made by parents, nursing staff, and the study investigators, potentially introducing an element of bias. This study suggested that the use of such topical local anesthetic agents was safe and may have potential benefit.
Discussion
This systematic review identified 15 studies investigating the use of various drugs often used to manage neuropathic pain to treat pruritus after burn injury. The analysis has demonstrated that gabapentin is effective in treating pruritus after a burn injury, resulting in an improvement of around 2 points on a VAS when compared with antihistamines.
When compared with placebo, gabapentinoids were also beneficial, although the confidence intervals in the meta-analysis were wide. The drugs used in each of the two included studies also differed, as did the indication for their initiation. Zheng et al30 investigated gabapentin in the management of pruritus, whereas Gray et al24 investigated the use of pregabalin in patients with neuropathic pain, demonstrating a much smaller improvement in pruritic symptoms. This perhaps reflects the patient selection in this study whereby pain was the cardinal symptom, rather than pruritus. Given these limitations, it is therefore not possible to conclude whether this improvement is reproducible among the class of gabapentinoids or only evident with gabapentin.
Gabapentinoids are now used for a wide variety of indications. Although structurally similar to the inhibitory neurotransmitter GABA (gamma aminobutyric acid) found throughout the central nervous system they do not act on GABA receptors and their benefit in the management of pain and pruritus is likely to be due to action at voltage-gated calcium channels and NMDA (N-methyl D-aspartate) receptors within the spinal cord and brain, inhibiting the release of excitatory neurotransmitters.36
Previous studies have demonstrated the benefit of gabapentinoids in reducing central sensitization and wind-up phenomenon to an acute painful stimulus in an effort to treat neuropathic pain.37 38 Such pathophysiological changes are characterized by alterations in the function of nociceptive neuronal pathways in response to persistent activation, inflammation, or injury. These changes lower the thresholds by which nociceptive neurons are activated, resulting in chronic pain syndromes and additional features such as hyperalgesia and allodynia.39 Given similar theories have been outlined to explain the pathological changes that result in chronic pruritus after burn injury, it is therefore logical that gabapentinoids may improve itch.14
The anti-neuropathic effects of gabapentinoids are increasingly used in a spectrum of pruritic and painful conditions, many of which these drugs are not licensed for.40–49 Such expanding uses of these drugs have seen an increase in gabapentinoid prescriptions across the UK, Europe, and North America.50–53 However, the potential harm from such agents, particularly gabapentinoids, is becoming clear. A systematic review of 59 studies highlighted the increasing use of gabapentinoids for recreational use and abuse.54 In Scotland, gabapentinoids are increasingly implicated in drug-related deaths, with toxicology reports from 2017 implicating gabapentin in 14% of such deaths and pregabalin in 12%.50 Given the risks of dependence and harm with the use of these drugs,50 55–57 gabapentin and pregabalin were categorized as Class C controlled substances in the UK in April 2019.58 In the USA, pregabalin has been a Schedule 5 controlled substance since its release in 2005 and some states have recently reclassified gabapentin in the same category. Patients with a previous history of psychiatric comorbidity, alcohol, or drug misuse are at even higher risk of harm when prescribed gabapentinoids.54 55 In the context of individuals suffering a burn injury, such comorbidities are not uncommon, prompting vigilance when prescribing these drugs.59–61
Furthermore, more work is required to establish the clinical significance of a reduction in VAS of around 2 points when compared with antihistamines alone, particularly given the potential for harm. The threshold whereby a treatment effect measured on such a scale is considered beneficial remains a topic of debate.62
Although observational data suggest topical EMLA may be a safe and potentially effective therapeutic option when used on healed burn wounds in children, such therapy will be limited by the size of pruritic area. Systemic absorption and the risk of local anesthetic toxicity must always be considered, particularly with larger areas of application. Topical lidocaine is increasingly being used in multiple conditions63–67 but the evidence for benefit in neuropathic pain is lacking, with NICE concluding that the evidence is insufficient to issue any recommendation on its use.18 Topical lidocaine, however, has been effective in managing pruritus in animal models,68 pruritus ani,69 and notalgia paresthetica.70
Although topical doxepin showed promise in healed burn wounds in early studies, such results have not been replicated in more recent trials described in this review. Although our meta-analysis of all studies investigating doxepin suggests an improvement in pruritic symptoms, this should be interpreted with caution due to the high risk of bias of two of the included studies.
This systematic review has several limitations. The paucity of RCTs included in our final analysis reflects the quality of evidence investigating these drugs in patients with burns. This resulted in only small numbers being included in the meta-analyses and a narrative review being conducted for the remaining studies.
Although the drugs we investigated are classically used to manage neuropathic pain, we elected not to focus on this specific pain condition, but rather pruritus given the increasing use of such drugs in other pruritic disorders and the recognized clinical and pathophysiological similarities between neuropathic pain and pruritus. Although some studies have demonstrated a reduction in morphine consumption and improved acute pain scores with the use of gabapentin,71–73 there is a lack of evidence studying their specific use in neuropathic pain in patients with burns.74
The VAS or other numerical scoring systems were commonly used to report pruritus outcomes. However, other methods included itch episodes, breakthrough doses of antihistamines, and the itch severity scale. Difficulties were encountered due to these multiple reporting methods. Similar issues have been highlighted in other systematic reviews, often from pain management literature, highlighting the difficulties in standardizing and validating such outcome measures.75
This systematic review also limited the interventions being investigated to those drugs listed by NICE for the management of neuropathic pain. Despite this wide inclusion criteria including multiple drugs and drugs classes, the literature search did not return any information on therapies such as other tricyclic antidepressants, including amitriptyline, or selective serotonin reuptake inhibitors that have been used to manage pruritus in other conditions.76 77 Other therapies beyond pharmacological management may be of benefit in pruritus, namely, psychotherapy such as cognitive behavioral therapy, transcutaneous electrical nerve stimulation, and acupuncture. These were not addressed in this review.9
Conclusions
Gabapentin appears effective in the management of pruritus associated with burn injury. Topical lidocaine may be a safe and effective option for managing pruritus in small surface area healed burns. Topical doxepin, although used to manage pruritus in eczema, does not appear to be effective in burn injuries.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank the burn team at Glasgow Royal Infirmary for their advice on guidance, especially Mr Stuart Watson, Ms Eleanor Roberston, Katrina Dalgarno, Gillian Calder, and Ellen Meland.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CM preformed literature searches, study review and selection, conducted data collection and analysis, and drafted and revised the article. CM is the guarantor. WN performed study reviews and data collection. LP supervised literature review and study selection. TQ and KP revised the manuscript and supervised all aspects of the study. MS supervised statistical analysis and revised the manuscript. AM, NA, CG, and MB contributed to the planning of the study and revised manuscript drafts.
Funding Open access funding costs were provided by a grant from the Association of Anaesthetists, grant number NIAA19R213.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.