Article Text

Abstract
Background The early COVID-19 pandemic period significantly strained the US healthcare system. During this period, consultations and admissions for acute medical conditions decreased, which was associated with an increase in disease-specific morbidity and mortality. Therefore, we sought to determine what, if any, effect the early COVID-19 pandemic period had on the presentation, management, and histopathologic severity of acute appendicitis.
Methods We performed a retrospective, observational study to compare the frequencies with which patients presented with acute appendicitis, the proportion of whom were managed surgically, and the distribution of histopathologic disease severity among all resected appendix specimens during the early COVID-19 pandemic period (March 6–June 30, 2020) to equivalent time periods for the 3 preceding/pre-pandemic years (2017–2019).
Results Compared with equivalent pre-pandemic time periods, during the COVID-19 pandemic period there was no significant difference in the number of patients who presented for acute appendicitis, there was a decreased rate of surgical management (81% vs 94%; p=0.014), and there was an overall increase in the incidence of perforated appendicitis (31% vs 16%; p=0.004), including by histopathologic diagnosis (25% vs 11%; p=0.01).
Discussion Despite potential patient hesitancy to present for care, the early COVID-19 pandemic period was associated with no significant change in the number of patients presenting with acute appendicitis; however, there was a significant increase in the incidence of perforated appendicitis. This study highlights the need to encourage patients to avoid late presentation for acute surgical conditions and for the robust planning for the medical management of otherwise surgical abnormalities during episodes of restricted or limited resources.
Level of evidence Level III.
- COVID-19
- appendicitis
- appendectomy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Acute appendicitis is one of the most common acute surgical conditions. Operative management by appendectomy is the standard treatment, although there is a push towards an antibiotic-first approach in some patient populations.1 In stable patients with clinical and radiographic evidence of perforated appendicitis, initial medical management with the option of interval appendectomy is also a safe alternative.2 Preoperative prediction of severity of appendicitis based on clinical, laboratory, and radiographic evidence can vary greatly among individual cases and among interpreting physicians.3 Definitive disease severity can be assessed by histopathologic assessment of resected tissue.
The early COVID-19 pandemic period was associated with marked changes in the rates of presentation, diagnosis, and management of many non-COVID-19-related illnesses. Emergency department visits, hospital admissions, and surgical emergencies for non-respiratory illnesses decreased during the early pandemic period.4 5 Although professional societies encouraged models of healthcare delivery that would limit risk of exposure of both providers and patients to SARS-CoV-2, there is no biologic reason for the incidence of acute surgical conditions to decrease during a respiratory disease pandemic. This raises the concern that patients may have delayed or even avoided seeking medical care due to fear associated with the COVID-19 pandemic. Delayed diagnosis of, or medical intervention for, acute appendicitis can lead to perforation and is associated with increased costs, increased complications, and worse clinical outcomes.6 7 Considering the uncertainty of the risk of surgery to both patients and treating clinicians, professional societies made recommendations to alter management of diseases such as appendicitis, suggesting antibiotics over surgical management.8 Therefore, we sought to determine what, if any, impact the early COVID-19 pandemic period (March 6–June 30, 2020) had on the presentation, management, and histopathologic severity of acute appendicitis.
Methods
Our institutional electronic medical record database was queried for all patients who presented to the Johns Hopkins Hospital between March 6 and June 30 in 2017–2020 with a clinical diagnosis of acute appendicitis (International Classification of Diseases—10th Revision: K35, K36). This cohort included all patients with the above diagnoses who were managed either operatively or non-operatively. We also confirmed that for the patients who underwent appendectomy, a pathological report was generated for the appendix specimen. Clinical histories for every identified case of acute appendicitis were reviewed. Cases between March 6 and June 30, 2020 were included to focus our study on the early pandemic period in the USA. Cases during the same time interval in the three previous years (2017–2019) were included as non-pandemic cohorts.
Pathological reports for each surgical case were reviewed by a board-certified pathologist and pathology resident. Histopathologic appendicitis severity was categorized based on the American Association for the Surgery of Trauma grading scale: 0, histologically unremarkable/no acute inflammation; 1, suppurative appendicitis; 2, gangrenous appendicitis; or 3, perforated appendicitis.9 Cases where other diseases, not associated with acute appendicitis, were observed were categorized as ‘Other’.
We compared patient count data from the pre-pandemic periods (2017–2019) with that of the early COVID-19 pandemic period for each outcome (demographics, rate of operative management, histopathologic appendicitis severity score, and rate of perforated appendicitis). Statistical analysis was performed using IBM SPSS Statistics (V.25). Pearson χ2 or Fisher’s exact test was applied where appropriate. Tests with a p value of <0.05 were considered statistically significant.
Results
There were 65, 63, 81, and 74 patients diagnosed with and treated for acute appendicitis between March 6 and June 30 in 2017, 2018, 2019, and 2020, respectively. The age and sex of patients in these four cohorts were similar with a female proportion ranging from 23% to 33% and a median age ranging from 12 to 16 years (table 1).
Cohort demographics and rate of operative management of acute appendicitis
Of the patients who presented for and were diagnosed with acute appendicitis, 60 (92%), 60 (95%), 76 (94%), and 60 (81%) were managed surgically by appendectomy in 2017, 2018, 2019, and 2020, respectively (table 1). Compared with the early pandemic period, there was a significantly greater rate of surgical management for acute appendicitis in the pre-pandemic period (relative risk (RR): 1.16, 95% CI: 1.03 to 1.20, p=0.01) (table 1). Of the patients managed surgically, there were no significant differences among the cohort demographics (table 1).
We categorized the severity of acute appendicitis in cases that were managed surgically using the pathological specimens based on a 4-tier scale from histologically unremarkable (0) to perforated (3). There were 15 (25%) cases of perforated appendicitis identified during routine histopathologic examination in the early pandemic period. During the pre-pandemic period, in 2017, 2018, and 2019, there were significantly fewer cases of perforated appendicitis: 5 (8%), 7 (12%), and 11 (14%), respectively (RR: 0.47, 95% CI: 0.26 to 0.84, p=0.01) (table 2). Conversely, there were 7 (12%), 5 (8%), 5 (7%), and 1 (2%) specimens from 2017, 2018, 2019, and 2020, respectively, that demonstrated no significant pathological findings (RR: 5.2, 95% CI: 0.71 to 38, p=0.10) (table 2). The frequency and proportion of the cases of appendicitis with intermediate histopathologic severity were similar among all cohorts (table 2).
Histopathologic severity of appendicitis from surgical resection specimens
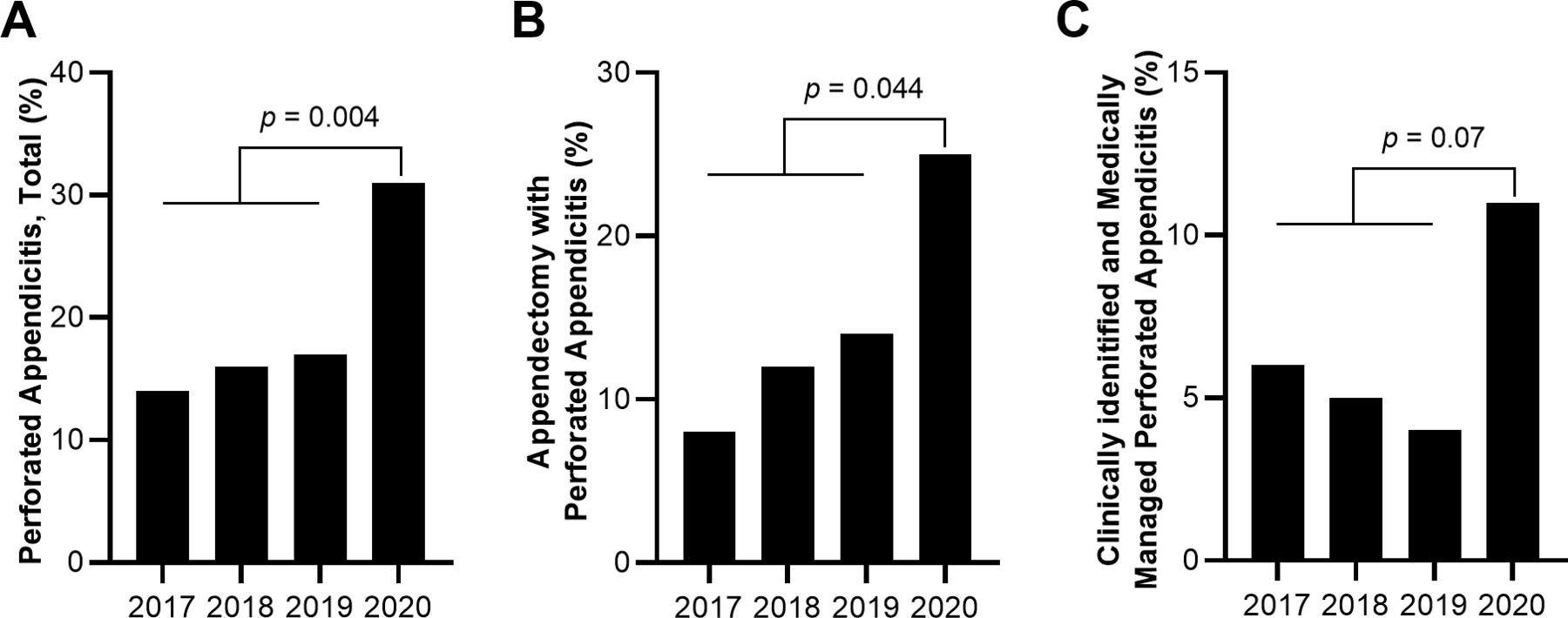
We compared the incidence of perforated appendicitis that was diagnosed clinically and by histopathology. In 2017, 2018, 2019, and 2020, there were 9 (14%), 10 (16%), 14 (17%), and 23 (31%) total cases of perforated appendicitis, respectively. Compared with the early pandemic period in 2020, there were significantly fewer total cases of perforated appendicitis in the pre-pandemic cohorts (RR: 0.51, 95% CI: 0.32 to 0.81, p=0.004) (table 3 and figure 1). This included significantly fewer cases of perforated appendicitis diagnosed by histopathologic examination of resected tissue from during the pre-pandemic periods as compared with the early COVID-19 pandemic cohort (RR: 0.54, 95% CI: 0.30 to 0.98, p=0.044) (table 3 and figure 1).
Incidence of perforated appendicitis

{kind=link}
Proportion of perforated appendicitis among all cases of acute appendicitis. (A) Total perforated appendicitis. (B) Cases of perforated appendicitis diagnosed after operative management/appendectomy and identified by histopathology. (C) Cases of perforated appendicitis diagnosed clinically and managed medically.
Discussion
In this study, we have shown that during the early COVID-19 pandemic period, at a single US institution, as compared with the 3 previous years, the number of patients who presented for acute appendicitis did not significantly change, that operative management of acute appendicitis decreased, and that this pandemic period was associated with a significant increase in the incidence of perforated appendicitis.
At the start of the COVID-19 pandemic, a global lack of understanding of this novel virus and disease led to national and global changes in medical practice. Non-emergent visits and procedures were postponed and focus was turned to minimizing transmission and management of patients who were affected by SARS-CoV-2.10 Acute care surgeons and their staff, who frequently manage acute appendicitis, were limited due to the need to support the critical care of patients with COVID-19 and ensuring trauma care was also uninterrupted.11 In addition, stay-at-home orders, public uncertainty, and fear of a novel human pathogen likely led to patient hesitancy to seek medical care. Indeed, during the early pandemic period, there was a decrease in the frequency of patients with non-emergent conditions. However, the significant decrease in multiple emergent medical and acute surgical conditions in the USA and globally was unexpected.12 13 Here we have shown that at a single US tertiary care hospital, the rate of patient presentation for acute appendicitis did not decrease during the early pandemic period, as compared with equivalent time periods from the 3 preceding years. Other studies from international and US hospitals have reported discordant results with respect to the rate of acute appendicitis diagnosis during the early pandemic period, which may be due to, in part, their comparison with rates only of the year prior, in 2019.5 13–16 However, studies that have also evaluated total acute care surgical cases during the early pandemic period have consistently demonstrated decreased volume, with the most dramatic decreases seen in acute biliary and bowel surgical conditions and, at most, only modest decreases in acute appendicitis.5 16 Therefore, the early COVID-19 pandemic period appears to be associated with significant decreases in total acute surgical case volume, with rates of presentation and management of specific acute surgical conditions varying among institutions and countries, consistent with the variable regional responses and attitudes towards the pandemic at the time.
The decreased rate of acute surgical and medical conditions raises the concern that patients may have delayed or even avoided seeking medical care during the early pandemic period out of fear of viral transmission or misunderstanding of public health recommendations. In at least two studies that focused on acute coronary syndrome and myocardial infarction, the early COVID-19 pandemic period was associated with delayed patient presentation, increased disease severity, and increased morbidity and mortality.4 More generally, the early pandemic period was associated with a significant increase in non-COVID-19-related deaths.17 With respect to acute appendicitis, delayed presentation and intervention increases the risk of disease progression and perforation.6 7 The incidence of perforated appendicitis in non-pandemic periods is estimated between 13% and 20%.18 We found the incidence of perforated appendicitis in our pre-pandemic cohorts to be between 14% and 17%, but noted a significant increase to 31% during early pandemic period. Moreover, there was a trend towards nearly twice as many cases of perforated appendicitis diagnosed clinically and medically managed, as compared with previous years. This alarming increase in perforated appendicitis during the early pandemic period, along with the trend of decreased histologically unremarkable/normal surgical pathological specimens, suggests delayed patient presentation and warrants further investigation into additional factors that may have contributed to these outcomes.
The COVID-19 pandemic presented an intriguing situation in which we were able to evaluate the issue of how to manage cases of acute appendicitis. Although the average rate of surgical management of acute appendicitis in the USA is approximately 95%,19 we and others have described a significant decrease in the rate of surgical management of acute appendicitis during the early COVID-19 pandemic period. Several studies have investigated the use of antibiotics in uncomplicated acute appendicitis. Most notably, results from the recent, US-based Comparison of Outcomes of Antibiotic Drugs and Appendectomy trial suggest that antibiotic treatment for uncomplicated acute appendicitis is non-inferior to appendectomy with respect to standard health status measures.20 Future studies aimed at more comprehensively evaluating the trends of presentation and management of acute appendicitis during the COVID-19 pandemic will be important in understanding whether management and outcomes data from this period will be useful in informing future practice.
This project has some limitations. First, we present here data from only a single large, academic teaching center that may not be generalizable to other hospitals. Second, we do not include any long-term follow-up data, which is most likely relevant to patients initially treated non-operatively. Therefore, future studies aimed at understanding long-term outcomes of the cases of appendicitis diagnosed and managed during the early COVID-19 pandemic period will elucidate the ultimate rate of interval appendectomy and of the morbidity associated with this pandemic period.
In conclusion, as in previous viral pandemic and epidemic periods, the early COVID-19 pandemic period was associated with recommendations to modify healthcare delivery to limit viral transmission. As a result, the COVID-19 pandemic was remarkable for a decrease in admission for acute surgical and medical conditions. Here, we have shown that, at a single tertiary care hospital, the incidence of acute appendicitis did not decrease during the early pandemic period, but that this period was associated with a significant reduction in the rate of operative management of acute appendicitis and with a significant increase in the incidence of perforated appendicitis. These data will be particularly relevant in informing institutional and public health measures aimed at minimizing morbidity and mortality associated with acute surgical conditions in future pandemics or resource-limiting situations.
Ethics statements
Ethics approval
This study was approved by the Johns Hopkins University School of Medicine Institutional Review Board (#259607) with a waiver of informed consent.
Acknowledgments
This publication was made possible by the Johns Hopkins Institute for Clinical and Translational Research (ICTR) which is funded in part by grant number UL1 TR003098 from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research.
References
Footnotes
Contributors TDZ—study design, data analysis, manuscript writing and submission preparation. EMB—study design and manuscript writing. ECP—study design and manuscript writing. AAW—data analysis and manuscript review. ED—data analysis and manuscript review. ERH—manuscript writing and review. KJS—study design, data analysis, manuscript writing and review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The contents are solely the responsibility of the authors and do not necessarily represent the official view of the Johns Hopkins ICTR, NCATS or NIH.
Competing interests ERH reports research funding from the Patient-Centered Outcomes Research Institute (PCORI), the Agency for Healthcare Research and Quality (AHRQ), the NIH/NHLBI, the DOD/Army Medical Research Acquisition Activity, and the Henry M Jackson Foundation for the Advancement of Military Medicine (HJF). ERH receives royalties from Lippincott, Williams, Wilkins for a book—'Avoiding Common ICU Errors'. ERH was a paid speaker for the Vizient Hospital Improvement Innovation Network (HIIN) VTE Prevention Acceleration Network.
Provenance and peer review Not commissioned; externally peer reviewed.