Article Text

Statistics from Altmetric.com
History
A 48-year-old man playing cards was accused of cheating. An assailant with a shotgun wounded the victim in the area of the right biceps muscle. When personnel from emergency medical services arrived, they applied a pressure dressing to the right arm to control profuse hemorrhage.
Examination
The patient was awake and alert with a heart rate of 130 beats per minute and a systolic blood pressure of 110 mm Hg. The pressure dressing over the right arm was saturated with blood and was removed. Findings on examination included the following: a 20×12 cm cavity in the anterior right arm; absence of much of the right biceps muscle; absence of the brachial artery and venae comitantes; an intact median nerve; limited function of the right elbow; intact function of the right wrist and fingers; and absent right radial and ulnar pulses at the wrist.
Management
A pressure dressing was reapplied to the open wound in the right arm. As a blood specimen was drawn for type and cross-match, resuscitation with a crystalloid solution was initiated. An X-ray of the right arm documented that the shotgun pellets were all in the area of the right biceps muscle (figure 1). After administration of a cephalosporin antibiotic, the patient was moved to the operating room.
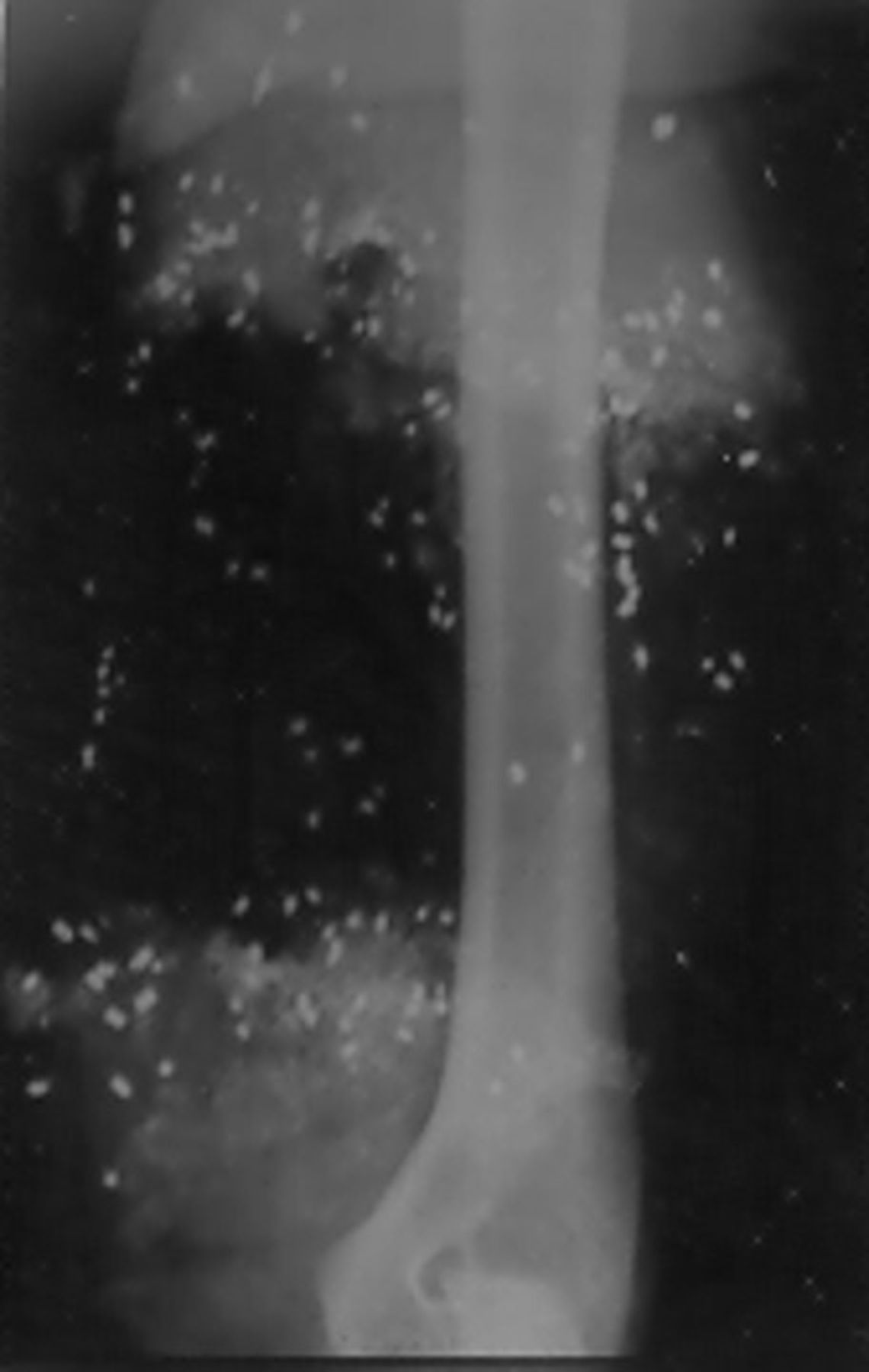
X-ray of the right humerus documents no fracture and limited distribution of pellets.
Skin preparation and draping included the chest and the entire right upper extremity from the left nipple to the right fingernails and from below the umbilicus to the toenails bilaterally. After the pressure dressing was removed, there was profuse venous hemorrhage from the open wound in the anterior right arm. Attempts at suture and metal clip control of multiple open veins had an only modest effect on controlling the hemorrhage.
Question
Based on the injuries described, your choice for management at this point would be to:
Management
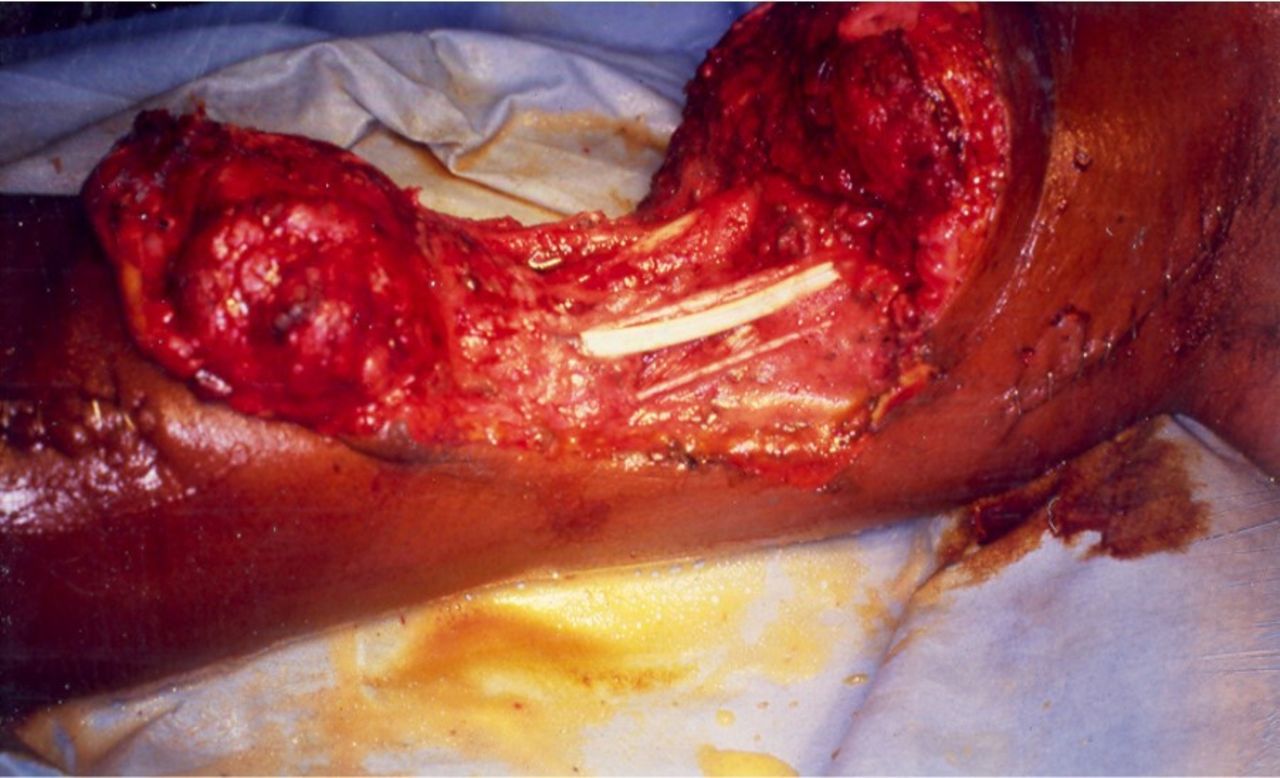
With no injuries to the right humerus or to the nerves in the arm and with intact function of the right wrist and fingers, an amputation in the proximal right arm as a therapeutic option was rejected. To control venous hemorrhage, the ends of one of the brachial venae comitantes were isolated in the open wound. Then, a 4 mm polytetrafluoroethylene (PTFE) interposition graft was inserted into the venous system with continuous 6-0 polypropylene sutures on both end-to-end anastomoses (figure 2). After the release of the bulldog clamps on the reconstituted brachial vein, the hemorrhage in the large open wound essentially ceased.

Open wound of the right arm after 4 mm polytetrafluoroethylene graft was inserted into the brachial vein.
An extra-anatomic arterial bypass appeared to be the best option in this patient with segmental loss of the brachial artery under a large defect in the soft tissue.
Longitudinal proximal and distal incisions were then made in the medial right arm outside the open wound to allow for exposure of the ends of the brachial artery. Once exposed, #3, #4 and #5 Fogarty balloon catheters were passed proximally and distally into the right brachial artery to remove any thrombus. Each end of the artery was then infused with 20 mL of a solution of heparinized saline (50 units of unfractionated heparin/1 mL of saline).
An anteromedial incision was then made in the right groin and extended down the right thigh over the course of the greater saphenous vein. A 30 cm segment of the vein was excised, and the remaining ends of the vein in the right groin and distal thigh were ligated with 2-0 silk ties. The excised saphenous vein appeared healthy and dilated to a 6 mm diameter when injected under pressure with heparinized saline (figure 3).

Measuring length of the extra-anatomic saphenous vein bypass graft.
A subcutaneous tunnel on the posteromedial right arm outside and inferior to the large open wound was created bluntly using a #8 Bakes biliary dilator and a DeBakey aortic clamp. After the reversed saphenous vein graft was filled with heparinized saline, it was pulled through the subcutaneous tunnel with the DeBakey clamp. With the distal tie on the saphenous vein graft removed, injection of heparinized saline confirmed that the graft was not twisted in the tunnel.
The proximal and distal anastomoses of the right brachial artery outside the open wound to the tunneled extra-anatomic reversed saphenous vein graft were made with continuous 6-0 polypropylene sutures (two sutures, 180° each, for each anastomosis). Prior to completion of the distal anastomosis, proximal and distal flushing were completed in the usual fashion. Once the proximal bulldog vascular clamp was removed, there was pulsatile flow in the graft and return of palpable right radial and ulnar pulses at the wrist.
The longitudinal skin incisions over the proximal and distal artery-graft anastomoses were then closed in layers. This was performed using 3-0 absorbable suture in the subcutaneous tissue and 3-0 nylon sutures in a vertical mattress fashion in the skin. The base of the large open wound in the right arm was covered with a porcine xenograft (to protect the median nerve and the 4 mm PTFE graft in the right brachial vein), and the cavity above was packed open with dry mesh gauze.
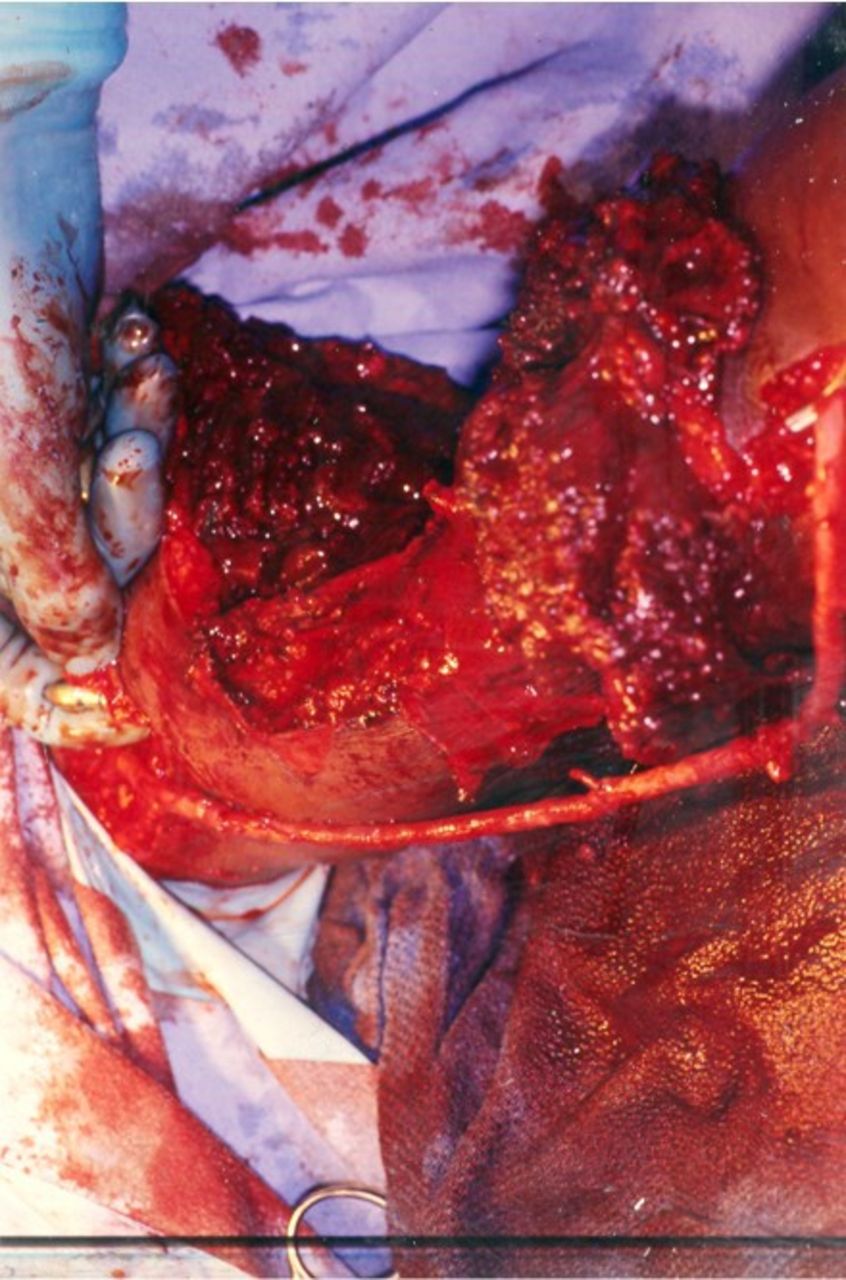
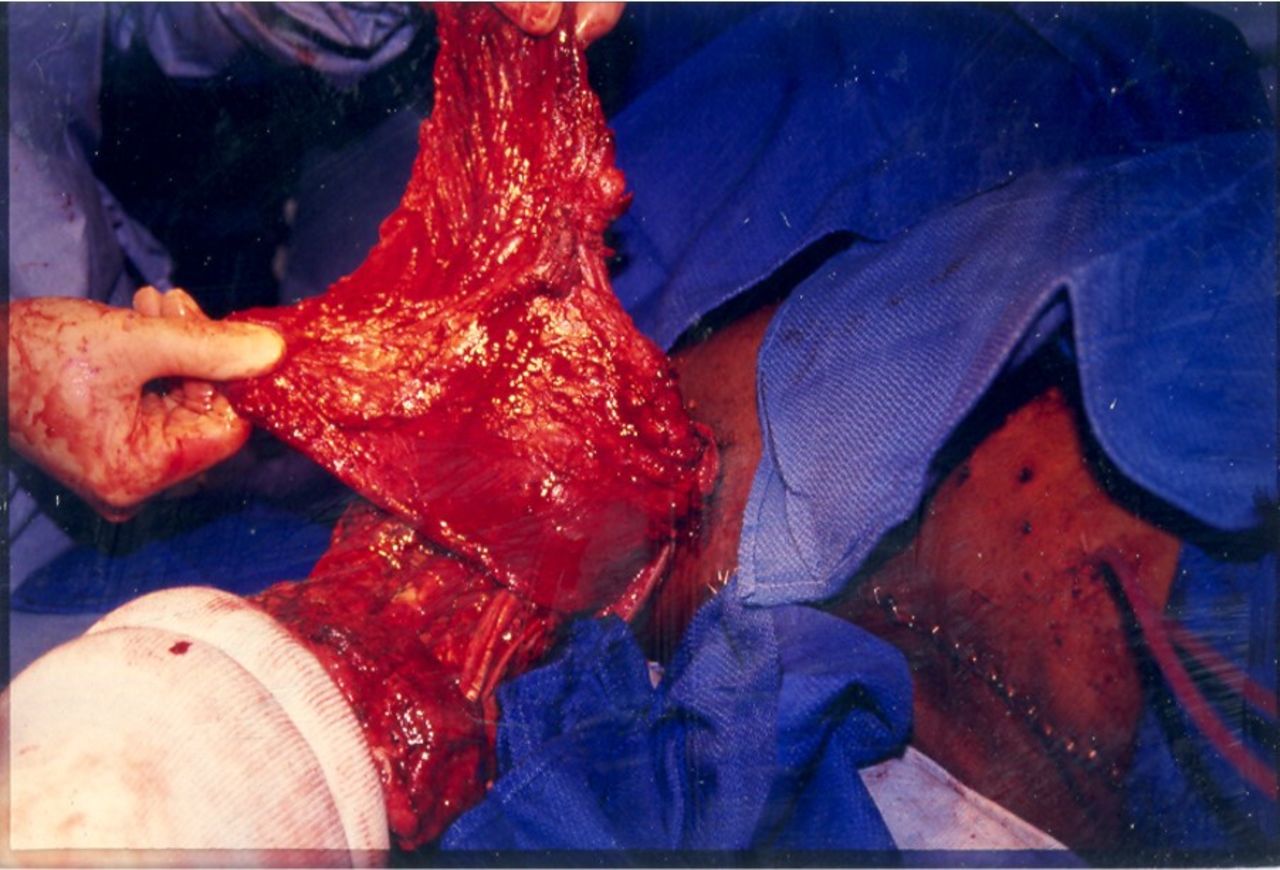
On the fifth postoperative day, the plastic surgery service elevated and rotated a flap of the right latissimus dorsi muscle into the defect in the right biceps muscle (figure 4). This muscle flap was immediately covered with a split-thickness skin graft, which healed completely (figure 5). At the time of discharge on the 27th day after injury, the patient had normal pulses at the right wrist, a healed wound over the right arm, and excellent function of the right elbow—flexion to 100° and extension 20° short of normal.

Elevation of the right latissimus dorsi muscle flap.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Split-thickness skin graft over the right latissimus dorsi muscle flap inserted into the defect in the right biceps muscle.
Discussion
The injuries in this patient do not fit the classic definition of a “mangled extremity” (some combination of injuries to the artery, bone, nerve, tendon, and soft tissue).1 All trauma surgeons would agree, however, that the patient sustained a severe injury to an upper extremity in which immediate amputation was a consideration. The sequence of management in such a patient has been described in a prior “Case of the Month” in Trauma Surgery & Acute Care Open.2
As the patient did not need an airway or assistance with breathing, control of hemorrhage was the priority in the operating room after the pressure dressing was removed. Temporary control of hemorrhage from an injury to a proximal extremity can be attained by application of a tourniquet or blood pressure cuff. The major disadvantage to this approach is the increase in venous hemorrhage that results depending on the pressure applied by the compression device. Permanent options for control of venous hemorrhage include suture ligation, application of metal clips, or use of electrocautery. The latter option routinely fails in patients with elevations in venous pressure. In the patient described, re-establishing venous outflow with the insertion of a PTFE prosthesis into the right brachial vein led to a remarkable decrease in bleeding from the large open wound as previously described. It was assumed that the small (4 mm) diameter prosthetic graft would, at best, acutely decompress the congested distal arm and forearm, but would thrombose in the early postoperative period.3
There is little enthusiasm for performing amputation at different levels of the injured upper extremity unless there is a segmental, avulsion-type, or crush injury.4 If these contraindications to repair or replantation5 are present and amputation is necessary, the application of a myoelectric upper limb prosthesis in the later postoperative period is an option.6 Whereas the function of prostheses in the upper extremity has improved exponentially during recent military conflicts, intricate functions of the human hand are difficult to replicate.7
As noted in the case presentation, the intact neural function in the patient’s hand mandated operative repair rather than proximal amputation. The large defect in the soft tissue over the segmental loss of the right brachial artery mandated the insertion of an extra-anatomic saphenous vein graft away from the open wound in the right biceps muscle.8 9 The muscle flap rotated into the open wound by the plastic surgery service in the postoperative period covered the defect in the soft tissue and, possibly, contributed to the long-term excellent function of the right elbow.
Ethics statements
Patient consent for publication
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.