Article Text

Abstract
Background Reducing length of stay (LOS) is a major healthcare initiative. While LOS is closely linked to the diagnosis and procedure in elective surgery, many additional factors influence LOS on a trauma service. We hypothesized that more standardized patient management would lead to decreased LOS.
Methods Retrospective analysis of Trauma Registry data compared LOS before (PRE) and after (POST) implementation of standardized processes on a trauma service. Patients were subdivided by age (over and under 65 years). Data were compared using unpaired t-test, χ2 test and analysis of variance tests, where appropriate.
Results 1613 PRE and 1590 POST patients were compared. Although age and Injury Severity Score were similar, median LOS decreased by 1 day for the group overall (p<0.0001), and for subgroups over and under the age of 65 years (p<0.0001). Older patients were discharged home 13% more often in POST, compared with 4% more for younger patients.
Conclusions Improved standardization of processes on a trauma service reduced LOS in patients of all ages. A prospective study may identify specific factors associated with prolonged LOS, to allow further improvement.
Level of evidence III.
Study type Therapeutic/Care management.
- length of stay
- nurse practitioner
- geriatrics
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Length of stay (LOS) is a major driver of healthcare costs in the USA.1 It is closely measured and benchmarked by hospitals and healthcare systems. In elective surgery, LOS is related to the diagnosis and procedure and is to a large degree predictable.2 In contrast, the LOS of trauma patients is influenced by many factors beyond the diagnoses and procedures, including complications,3 4 pre-existing comorbidities,5 frailty,6 psychiatric illnesses,7 therapy/rehabilitative needs and resources or options for discharge disposition.8–10
The introduction of ‘fast-track’ and enhanced recovery after surgery (ERAS) protocols have resulted in remarkable decreases in LOS and costs among elective surgery patients in numerous disciplines.11 The outcomes are due in large part to the implementation of standardized, evidence-based practices with multidisciplinary team involvement and the continuous auditing and feedback of results.11 Multidisciplinary teams have also been found to reduce LOS in patients requiring tracheostomy after neurological trauma.12 Although ERAS principles have been employed with success in emergency general surgery (EGS)13 14 and in trauma patients undergoing laparotomy,15 their applicability across the spectrum of trauma patients is unclear. Care pathways may be applied to single-system injuries (eg, hip fractures), but there are many other variables at play in multisystem injured patients. Moreover, most of the variability in LOS among EGS patients was recently found to be related primarily to non-clinical factors.16 As we manage the clinical issues in our trauma patients, we frequently have to reconcile social issues such as lack of social support, homelessness and alcohol or drug abuse, in a discharge plan.
We recognized the need for more standardized patient management protocols and multidisciplinary team involvement in our trauma service and hypothesized that implementation of such processes would lead to reduced LOS. We further sought to determine whether we could identify specific factors that prolong LOS in order to improve the allocation of resources and discharge planning efficiency.
Methods
Scripps Memorial Hospital La Jolla is a 431-bed hospital verified by the American College of Surgeons (ACS) as a level II trauma center. In mid-November 2017, a formalized trauma service was created. Prior to this time, a group of four full-time and one part-time trauma surgeons shared trauma call. Each surgeon individually managed their admitted patients, with occasional cross-coverage as needed. Four advanced practice providers (APPs) assisted with management on the wards and in the trauma clinic, but not the emergency department (ED) or intensive care unit (ICU). Trauma case managers (CMs) and social workers (SWs) provided in-house coverage 6 days a week and on-call coverage on Sundays. After the addition of one more trauma surgeon in October 2017, the new trauma service was operationalized in mid-November 2017. The full-time trauma surgeons rotated each week as the trauma service rounder, managing all aspects of trauma inpatient care: ICU, wards, operating room (OR) and bedside procedures and trauma clinic coverage. One APP was assigned primarily to the ICU each day, and another to the ward. Our APPs perform all of the discharge work on the trauma service. Beginning in July 2018, in-house CM and SW coverage expanded to include Sundays. The SWs and CMs participated in our morning meeting (07:00–08:00 hours) beginning in the POST period.
This study was performed as part of our Trauma Performance Improvement and Patient Safety Program, as stipulated by the ACS Committee on Trauma. Data were collected from our Trauma Registry on patients from the 13 full calendar months prior to the initiation of the rounding service (PRE; October 1, 2016– October 31, 2017) and 13 months after (POST; December 1, 2017–December 31, 2018). All patients admitted to the trauma service, or to other services with trauma service consultation, were included. Hospital LOS was the primary outcome of interest. Patients who died during the primary hospitalization were excluded. To be consistent with ACS reports from the National Trauma Data Bank and Trauma Quality Improvement Program, LOS data are reported as median values.14 In order to examine the impact on geriatric patients specifically, patients were subdivided patients into those who were under the age of 65 years (YOUNGER) and those who were 65 years of age and older (OLDER). Data were compared using unpaired t-test (when comparing mean values), Mood’s median test (when comparing median values), χ2 test and analysis of variance test, where appropriate. Statistical significance was defined as p<0.05.
Results
A total of 3203 patients were admitted: 1613 in the PRE period and 1590 in the POST period. Characteristics of the two groups are presented in table 1.
Characteristics and outcomes of trauma patients admitted before (PRE) versus after (POST) implementation of formalized trauma service
Overall, 65% of the patients were male with a mean age of 52.1±23.3 years; mechanisms of injury did not change over time. The mean Injury Severity Score (ISS) was lower in the POST period (9.4 vs 9.9, p=0.03). After implementation of the formalized trauma service, there was an overall reduction in median LOS which decreased from 3 (IQR 2–4) days PRE to 2 (IQR 1–3) days POST (p<0.0001).
The OLDER subgroup of patients comprised 33% of the overall population. Mean ISS was no different between the OLDER (10.0±6.6) and YOUNGER (9.9±7.8) patients in the PRE period; in the POST period, mean ISS was the same among the OLDER patients (10.0±6.4) but slightly lower among the YOUNGER patients (9.1±7.5, p=0.02) (table 2). Median LOS decreased by 1 day in both age subgroups from PRE to POST (p<0.0001).
Characteristics and outcomes of patients 64 years and under and 65 years and older, before (PRE) versus after (POST) implementation of formalized trauma service
The presence of comorbid medical conditions was much higher among OLDER than YOUNGER patients in both time periods (table 2). Both age groups had fewer comorbid conditions in the POST period compared with the PRE period (p<0.0001). The rate of unplanned readmission within 30 days did not change between the two time periods (1.8% vs 1.9%). Among the YOUNGER group, readmission rate was 1.2% PRE and 1.5% POST; among the OLDER patients, the readmission rate was 2.0% PRE and 2.5% POST.
The hospital day of discharge is depicted in figure 1. In the PRE period, 390 (24%) of 1613 patients were discharged with LOS 1 day; this increased to 30% (473 of 1590) in the POST period. Total discharges with LOS 1–2 days increased from 44% PRE to 50% POST.

Number of patients by hospital length of stay (LOS) for all patients, PRE versus POST implementation periods.
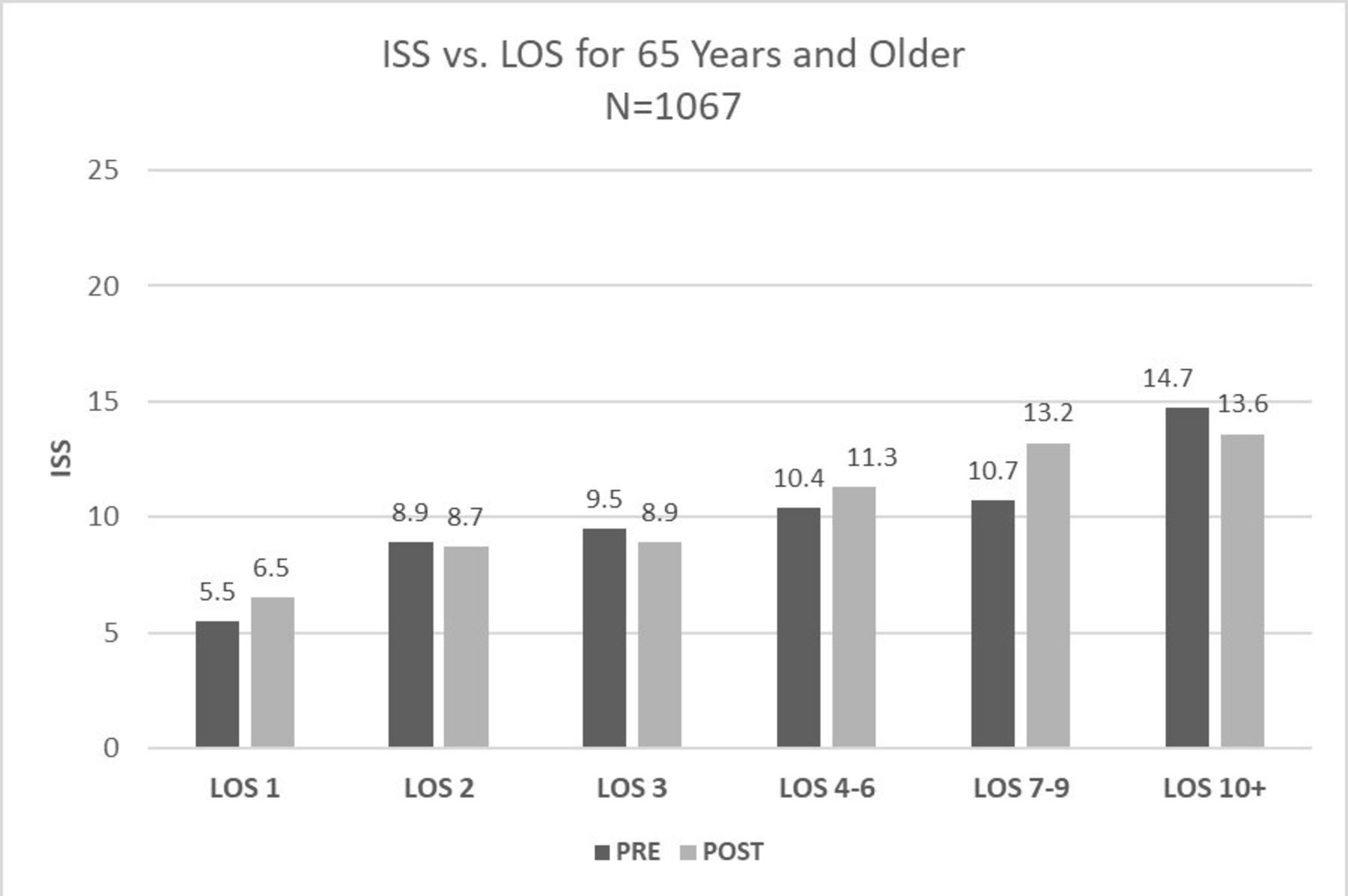
The relationship between ISS and LOS is depicted in figure 2 (Overall), 3 (YOUNGER) and 4 (OLDER). Those discharged by postinjury day 1 have a mean ISS that is significantly lower than those with longer LOS. There is, in general, a direct relationship between ISS and LOS for the group as a whole and for the YOUNGER group (figures 2 and 3). Among the OLDER subgroup, there is a flatter curve in the mid-range of LOS in the PRE period LOS 3–9 days; in contrast, in the POST period there seem to be plateaus at LOS 2–3, 4–6 and 7+ days (figure 4).
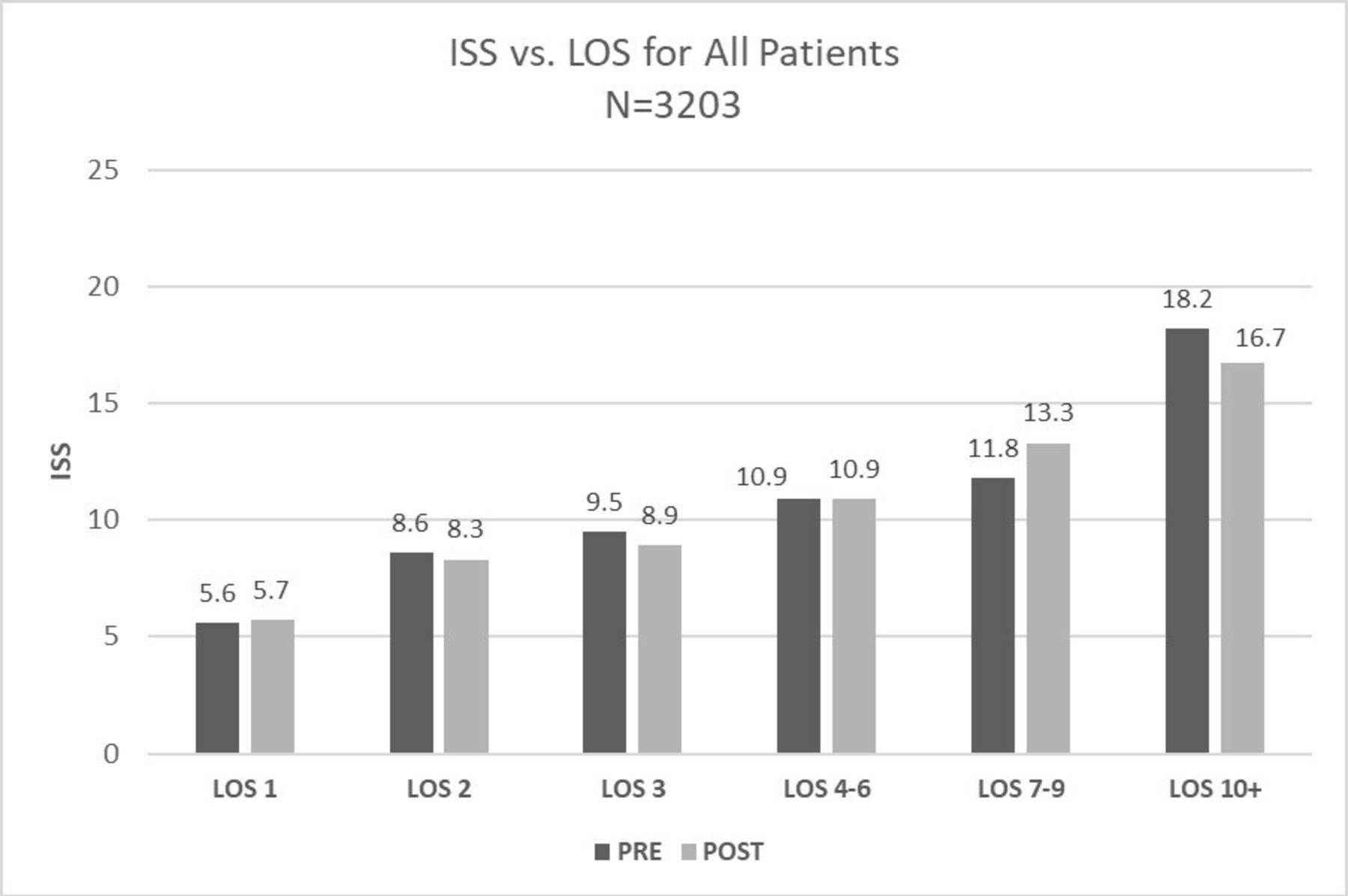
Mean Injury Severity Score (ISS) by hospital length of stay (LOS) for all patients, PRE versus POST implementation periods.
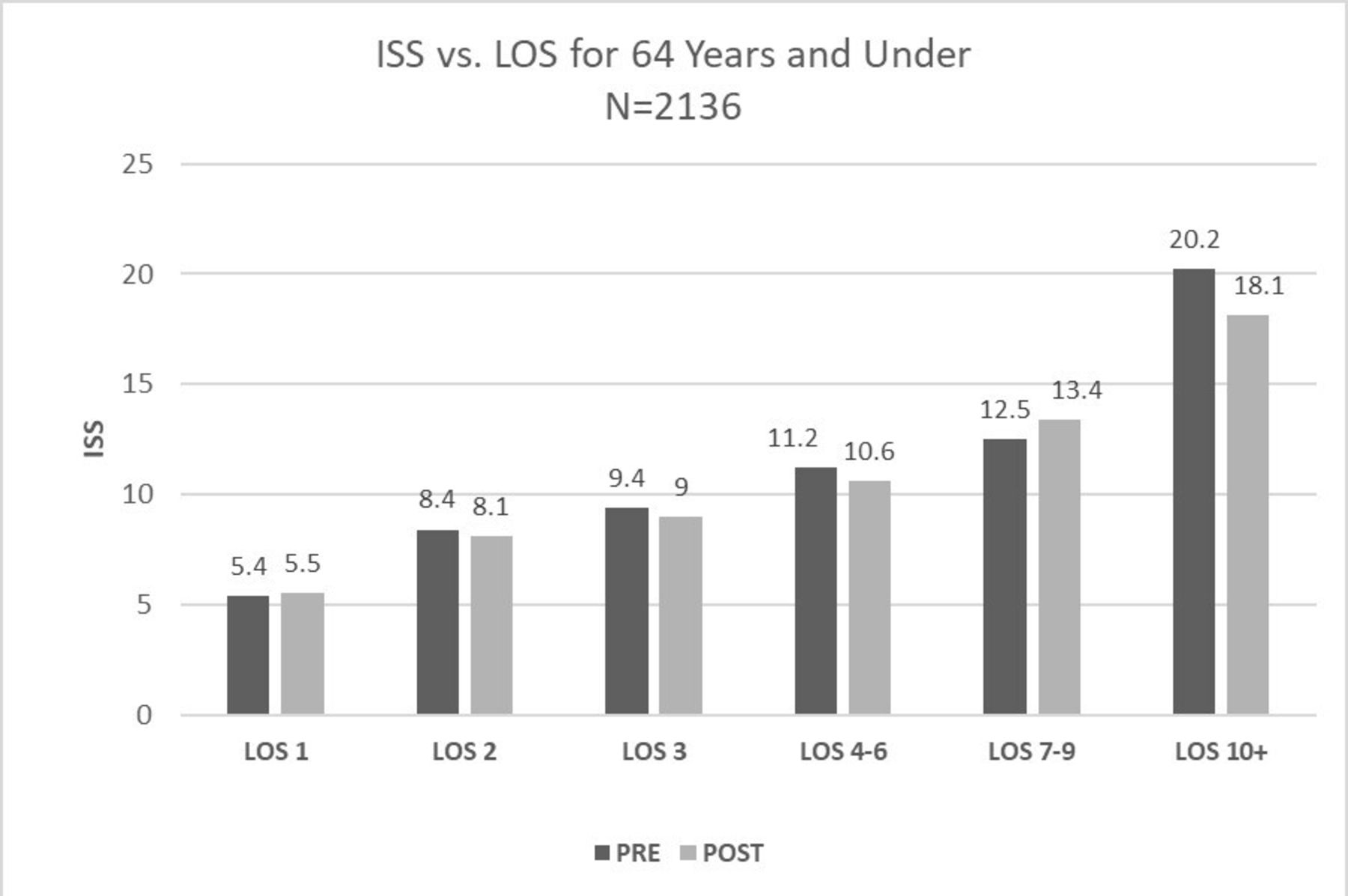
Mean Injury Severity Score (ISS) by hospital length of stay (LOS) for patients 64 years and under, PRE versus POST implementation periods.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean Injury Severity Score (ISS) by hospital length of stay (LOS) for patients 65 years and older, PRE versus POST implementation periods.
The discharge disposition among OLDER compared with YOUNGER patients was considerably less to home and more to skilled nursing facilities (table 2). Relatively few patients in either age group were discharged to rehabilitation.
In each of the time periods, 91 (6%) patients were admitted by other services with trauma service consultation. Some patients were transferred to medical services during their stay, resulting in 132 (8%) patients being discharged by a non-trauma physician in PRE and 149 (9%) in POST. Median LOS was analyzed based on whether patients were admitted to the trauma versus non-trauma service or discharged by the trauma versus non-trauma service; these comparisons were also made between the PRE and POST periods. In the PRE period, those admitted to a non-trauma service had a longer median LOS (4 days) compared with those admitted to the trauma service (3 days, p=0.0129). This was also true in the POST period (4 days vs 2 days, p=0.00017). The LOS was also longer among those discharged by a non-trauma service compared with the trauma service in the PRE period (4 days vs 3 days, p=0.0305) but not the POST period (2 days vs 2 days, p=0.3303).
Over the study period, trauma admissions varied with day of the week: Fridays and Saturdays are the busiest days, and Mondays are the slowest. However, although one-half of discharges occurred within 48 hours, the day of discharge did not have the same pattern as the day of admission. Sunday consistently had the lowest number of discharges. The OLDER patients had fewer discharges on weekends in the PRE period; in the POST period, Friday and Saturday discharges increased to the same levels as the weekdays, but Sundays still remained a bit lower. Among YOUNGER patients, discharge day was remarkably consistent in the POST period.
Discussion
We were able to achieve a 1 day reduction in median LOS in both YOUNGER and OLDER age groups with some changes in the trauma service. Taheri et al17 have questioned the economic benefit of reducing a day at the end of the hospital stay. However, their economic analysis is dated. In addition to the expense to the patient and healthcare system, there is opportunity cost to the hospital of having a bed occupied; there is one more patient to be tended to by nursing staff; and one more patient to be managed by the trauma team. When one adds up the time spent per patient per day of the trauma surgeon, APP, CM and SW, it is not a trivial burden.
The key elements of the service included a responsible, accountable surgeon providing continuity of care for a week and an expanded role for APPs including continuity from admission through discharge. The service adopted evidence-based clinical care guidelines and a multidisciplinary meeting involving trauma CMs and SWs reviewing the disposition plan for every patient, every day. There were no modifications to ancillary services (nursing, physical therapy, occupational therapy or respiratory therapy) during the two periods compared.
The reduction in LOS is difficult to specifically attribute in this retrospective analysis, as we reviewed trauma registry data but not medical records. The patient populations were similar in terms of age and mechanism of injury. While the ISS was lower in the POST group (9.4 vs 9.9), the clinical significance of this difference is marginal and does not adequately explain a full day reduction in median LOS. Moreover, the OLDER population had the same ISS in the POST period, and still had a 1 day reduction in LOS. At first glance, the admission disposition may suggest a lower-acuity population in the POST period, as there was a shift away from the ICU and intermediate care units, to the regular nursing ward and observation units (table 2). Again, while difficult to say with certainty in this type of review, we do not believe this reflects a lower-acuity population, but rather a conscious move to better resource utilization. For example, ICU admissions decreased from 28% to 21% (table 1). At the same time, unplanned ICU admissions were no higher in the POST period; in fact, they went down in both OLDER and YOUNGER subgroups (table 2). Anecdotally, the surgeons acknowledged that in the PRE period they had sometimes admitted patients to the ICU just to ‘keep a closer eye on them’. But in the POST period, the service assumed the care of the patient and so there was less need for the highest level of nursing care. There were fewer comorbid medical conditions in the POST period. Among the OLDER patients, the difference was statistically significant, but decreased only from 95% to 91%. It is unlikely that this was a factor in reducing LOS by 1 day, but it cannot be ruled out. Complications were not different between the two time periods with the exception of catheter-associated urinary tract infections (CAUTIs), which were higher in the POST period among OLDER patients. While documentation may have improved with team rounds, there was no conscious effort to improve documentation to account for the increase in CAUTIs.
The greatest increase in discharges was seen on postinjury day 1. The low ISS of this group reflects the fact that many of these patients were kept for observation. In the PRE period, the admitting surgeon would have gone home after a 24-hour on call shift and was not likely to return to the hospital again that day to discharge patients. In the POST period, there was a team to accept the patient in handoff and discharge them after a tertiary survey. Another factor was our increasing use of our ED observation unit which, as Ross et al18 demonstrated, offers increased cost savings, shorter stays and reduced inpatient admissions.
A major factor contributing to the reduction was creation of the trauma service and having a single accountable surgeon responsible for 1 week at a time. Regular presence and continuity allow a surgeon to better understand a patient’s and family’s needs, and discharges can be anticipated and planned ahead of time, rather than decided on the morning of rounds.
The role of the APP was expanded to include all aspects of patient care, from trauma resuscitation to the follow-up clinic. Involvement of the APPs in the resuscitation room and ICU led to more familiarity with the patients and better continuity of care. While we did not track the time of day that patients were discharged, workflow on the service during the POST period tried to prioritize early discharges. Others have found that APPs improved the efficiency of trauma services, reducing LOS and positively impacting discharge planning.19 20
In 2012, Gershengon et al reviewed the literature and found that APPs functioning within the ICU at adult trauma centers had a positive impact decreasing ICU LOS, improved communication and increased adherence to clinical practice guidelines. Collins et al21 22 demonstrated that APPs were able to reduce LOS in a stepdown unit by 0.35 days, and reduce overall hospital LOS by 0.55 days, independent of all other factors. For their institution, this translated into a cost savings of US$8.8 million over the course of 6 months. Holliday et al similarly demonstrated that for the trauma patient, the addition of APPs to the trauma team was associated with decreased LOS.23
An additional component of the new trauma service was a formal morning report 7 days a week, during which the entire team, including case CMs and SWs, receives handoff of new patients from the admitting trauma surgeon, and reviews the entire patient list to discuss patient care issues including disposition plans. This facilitates early discharge, as the CMs and SWs can focus on priority patients to sort out final details and barriers to discharge. This is similar to the findings of another center, which increased operational efficiency by implementing daily multidisciplinary discharge rounds led by a senior trauma physician.24 This streamlined the care of complex trauma patients, resulting in a 15% decrease in LOS.24 Another change, similar to what is emphasized in ERAS protocols, is that we have implemented more evidence-based clinical care guidelines. At our morning report, we discuss and reinforce management plans. This improves consistency as well as efficiency.
We cannot overstate the benefit of trauma service CMs and SWs to facilitate patient discharge planning as part of a multidisciplinary team.25 They navigate the non-clinical issues and interface with the skilled nursing facilities (SNFs), acute rehabilitation units (ARUs) and acute care facilities to which we transfer a large percentage of patients, and nearly half of the OLDER group. Indeed, as shown in figure 4, the LOS of the OLDER group does not relate directly to ISS, but is consistent with the many non-clinical factors known to impact their discharge disposition.10 12 16 19 20 24 The ability to discharge OLDER patients on weekends is directly related to having this process in place 7 days a week. And the fact that Sunday remained a discharge-day outlier is reflective of our inconsistency in CM/SW presence on Sundays until mid-2018. Our ability to discharge so many patients to home requires the early involvement of services like physical and occupational therapy to initiate rehabilitative therapies, and to have ongoing system support like CM and SW to help procure durable medical equipment. A literature review by Bristow et al highlights the importance of CM and SW working together in an acute setting such as the ED to decrease utilization of ED for non-emergent visits, promote the use community resources and improve discharge planning to avoid excessive costs.26 Integrating SW into an acute care setting has found to be complex, but the impact of SW support on patient care and resource use is substantial.27
The trauma literature is replete with examples of worse outcomes among geriatric trauma patients compared with younger adults.28 We treat a substantial number of geriatric trauma patients (33% of our trauma population) and were interested in that subgroup. While the age cut-off and definition vary somewhat, the Geriatric Trauma Committee of the AAST performed a survey and ‘age >65’ was the most common accepted definition of ‘geriatric’.28 Thus, we performed subgroup analysis of patients over versus under age 65 years.
Our OLDER patients averaged over 79 years old. Compared with the YOUNGER group, it was notable that the ISS was similar and that the LOS was only 1 day longer. Discharge planning in the OLDER group can be complex, as the trauma admission often signals a need to change the living situation. Indeed, our OLDER patients were not able to go home as often as the YOUNGER group. But our discharge to home rate is much higher than average. In the National Trauma Data Bank 2016 Annual Report, only 59% of patients overall were discharged to home.29 In our center, 71% of overall patients (2188 of 3078) were discharged to home, and 54% of OLDER patients in the POST group went home. As mentioned above, LOS in trauma patients is related to many factors other than the severity of injury. In both the PRE and POST groups, we did not have a high percentage of patients discharged to ARUs, and had a one-third of our population discharged to SNFs (table 2). This is a reflection of our patient population, with many older adults who do not meet criteria for ARU. It is interesting to note that, in the POST period, the YOUNGER patients had a more direct relationship between ISS and LOS. We believe the service was able to manage the extraneous factors more efficiently. The same trend occurred in the OLDER subgroup, but there is still more variability. This represents an opportunity for further prospective study.
A small percentage of the patients were admitted to (6%) or discharged from (8.8%) non-trauma services. As these patients were not being managed primarily by our service, any benefits of the trauma service change would not have been fully realized by them. When comparing admitting services of trauma versus non-trauma, there is a significant difference in LOS. When comparing the discharge services of trauma versus non-trauma, there is a significant difference, however this only holds true for the PRE group. This is likely due to having a mixed primary service (initially trauma, and later non-trauma), and partial realization of the benefits of the trauma service changes. In addition, for those whose primary service changed, it is unclear at which point in their hospital course this occurred. It should be noted, however, that those admitted to or discharged from non-trauma services were all included in the analysis and we still had the reduction in LOS. Thus, we think this is a potentially generalizable intervention.
Limitations
The reduction in LOS is difficult to specifically attribute, as this was a retrospective review-based primarily on trauma registry data and did not involve chart reviews. Consequently, we could not identify reasons for delays in discharge or specific factors that accounted for more timely discharge. We did not have case mix index or Acute Physiologic Assessment and Chronic Health Evaluation (APACHE) scores to confirm equivalence of the populations.
Conclusion
We conclude from this analysis that our LOS has improved since the implementation of the formalized trauma service. We cannot determine causality, or which factors were most beneficial. We have generated hypotheses that we will be able to study prospectively in the interest of optimizing LOS for our trauma patients.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Ethics approval
This study was reviewed and approved by the study hospital’s Institutional Review Board (IRB-19-7325). Requirement to obtain informed consent was waived under 45 CFR 46.116(d).
References
Footnotes
Presented at Presented at the 71st Annual Meeting of the Southwestern Surgical Congress Huntington Beach, California, April 2019.
Contributors Literature search: WLB, PRS, JW, KBS. Study design: WLB, PRS, KBS. Data collection: JW, KBS. Data analysis: WLB, NL, PRS, JW, KBS. Data interpretation: WLB, NL, JW, KBS. Writing: WLB, NL, PRS. Critical revision: WLB, NL, JW, KBS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.