Article Text

Abstract
Background Rib fractures and substance use are both common in trauma patients, but there is little data on how smoking and alcohol use may be associated with outcomes in these patients. We assessed the association between smoking or alcohol use disorder (AUD) and outcomes in patients with rib fractures.
Methods We used institutional databases to conduct a retrospective review of patients with rib fractures at the only American College of Surgeons-verified adult level 1 trauma center in a rural state between 2015 and 2019. The key exposure variables were smoking and AUD. The key outcome variables were mortality and pulmonary complications (pneumonia, adult respiratory distress syndrome, and pneumothorax). We used multivariable regression for analysis and directed acyclic graphs to identify variables for adjustment.
Results We identified 1880 eligible patients with rib fractures, including 693 (37%) who were smokers and 204 (11%) who had AUD. Compared with non-smokers, smokers were younger, more often male, and had lower mortality rates. Regression showed that smokers had a lower likelihood of mortality (OR 0.48; 95% CI 0.27 to 0.87; p=014). Likelihood of pneumonia, ARDS, and pneumothorax was not different between smokers and non-smokers. Compared with patients without AUD, patients with AUD were older, more often male, and had higher likelihood of pneumonia and lower likelihood of pneumothorax. Regression showed that patients with AUD had higher likelihood of pneumonia (OR 1.82; 95% CI 1.24 to 2.68; p=0.002) and lower likelihood of pneumothorax (OR 0.51; 95% CI 0.33 to 0.75; p=0.002).
Discussion In trauma patients with rib fractures treated at a level 1 trauma center over 5 years, smoking was associated with decreased risk of mortality. These findings have implications for risk stratification and clinical decision-making for patients with rib fractures.
Level of evidence III
- rib fractures
- mortality
- pneumonia
- pneumothorax
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Rib fractures are diagnosed in approximately 10% of patients with traumatic injuries.1 These injuries are associated with variable rates of mortality (4% to 25%) and pulmonary complications (13% to 35%).1–5 Many studies have identified risk factors and developed scores and protocols to predict and improve outcomes for these patients because of the potential benefit of accurate risk stratification, given the high frequency and severity of these injuries.6–13
Although variables such as age, number of ribs fractured, and comorbidities have been identified as risk factors,14–19 smoking and alcohol use disorder (AUD) have not been studied as thoroughly. A recent Trauma Quality Improvement Program (TQIP) study showed that patients with rib fractures who are smokers have lower rates of mortality than non-smokers (2.3% vs 4.6%; p<0.001),20 which substantiated previous reports of a ‘smoker’s paradox’, in which smoking appeared to be associated with improved outcomes in trauma patients.21 22 Other recent studies showed that alcohol use is associated with higher rates of pneumonia in patients with rib fractures.23 24 Many of these studies use data from national or urban populations with limited generalizability; our state has unique characteristics compared with the rest of the USA, including a higher percentage of smokers (23% vs 14%).25 26 Certain subgroups of patients with rib fractures have variable outcomes,2 so data from specific populations may be helpful in understanding the associations between smoking and AUD and outcomes.
In this study, we evaluated patients with traumatic rib fractures to determine how smoking and AUD were associated with mortality and pulmonary complications. This study contributes to the need for more data on the smoker’s paradox in trauma patients and explores the relationship of AUD and outcomes in patients with rib fractures. Our hypotheses were that smoking would be associated with lower rates of mortality and higher rates of pulmonary complications,2 20 and that AUD would be associated with higher rates of mortality and pulmonary complications.24 27 Our goal was to provide insight for risk stratification and clinical decision-making for blunt trauma patients with rib fractures who are smokers or have AUD.
Methods
We queried our institutional trauma database at the only American College of Surgeons (ACS)-verified level 1 adult trauma center in the state to identify patients with rib fractures. We cross-referenced these data with our Clinical Data Repository (CDR) to obtain information on pulmonary complications and number of rib fractures.
Patients with rib fractures were identified by Abbreviated Injury Scale (AIS) predot codes. Smoking status and AUD were determined by comorbidity codes from our institution’s trauma registry. This registry’s data dictionary defines ‘smoker’ as one who reports smoking cigarettes every day or some days within the last 12 months and defines ‘AUD’ as a patient who has ‘AUD’ documented in the medical record.28 This documentation is generally made by a provider who has taken a complete history and determined that the patient met criteria for the diagnosis based on the reported history of chronic alcohol use. Pulmonary complications and number of ribs fractured were determined by International Classification of Diseases version 10 codes in the CDR. Some patients had a clinical diagnosis of rib fracture(s) without a specified number of fractures, and they were categorized as ‘unspecified’ for the number of ribs fractured. Patients were included who met the following criteria: clinical diagnosis of one or more ribs fractured, age greater than 17 years, blunt mechanism of injury, year of arrival 2015–2019, and records contained in both the trauma registry and CDR databases. Patients were excluded if they died within 24 hours of admission or had a non-blunt mechanism of injury.
Descriptive analyses were conducted by smoking status or AUD diagnosis for patient characteristics (age, sex, race, smoking status, and AUD diagnosis), injury characteristics (number of ribs fractured, AIS for thorax body region, and Injury Severity Score (ISS)), and outcomes (total hospital days, total intensive care unit (ICU) days, total ventilator days, pulmonary complications, and in-hospital mortality). The pulmonary complications evaluated were pneumonia or ventilator-associated pneumonia (VAP), adult respiratory distress syndrome (ARDS), and pneumothorax. Χ2 test or Fisher’s exact test was used for categorical variables. Student’s t-test or Wilcoxon-Mann-Whitney test was used for continuous variables. All categorical variables were described as numbers and percentages. All continuous variables were described as means with SD or medians with IQR.
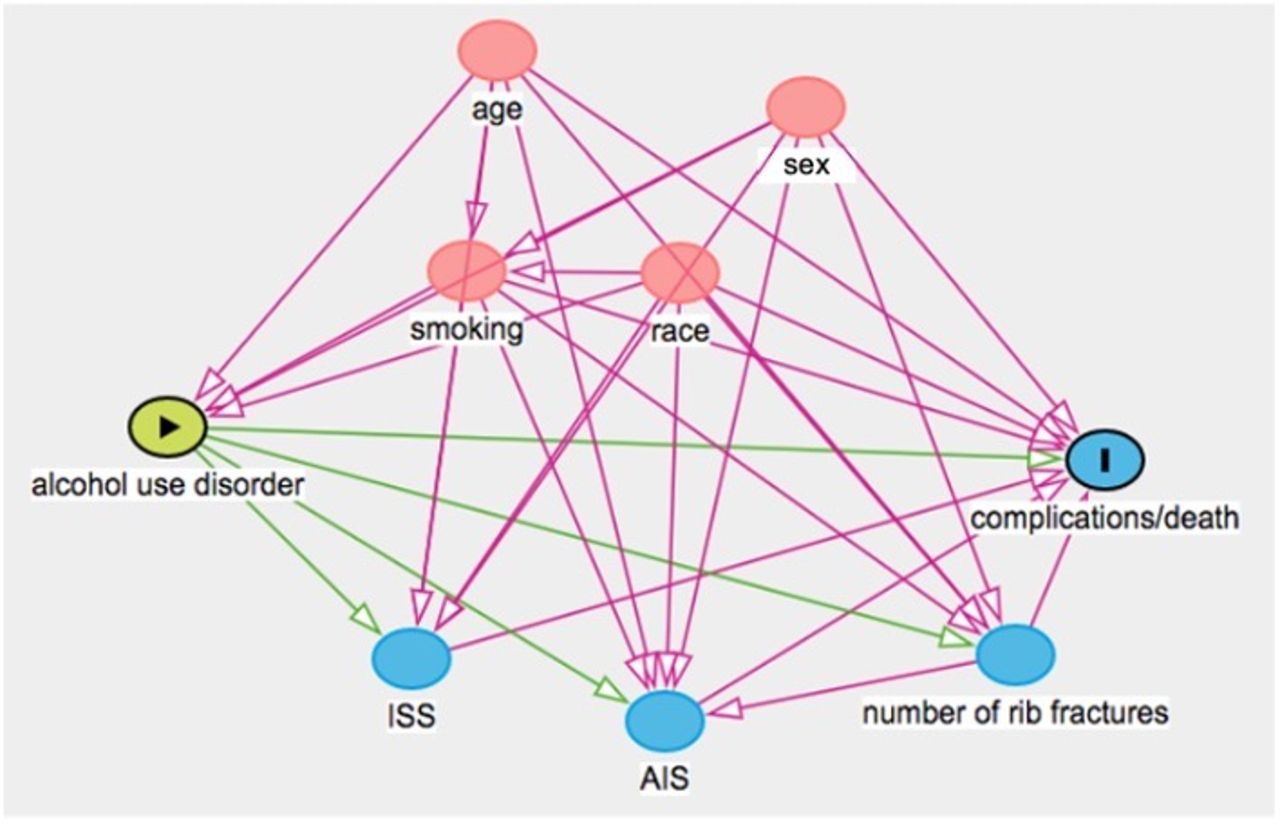
Multivariable logistic regressions were conducted to assess the association between smoking status or AUD and the risk of pulmonary complications or mortality. Control variables were chosen based on directed acyclic graphs (DAGs).29 A DAG is a validated method to identify potential confounders for multivariable regressions that is based on relationships between variables (figures 1 and 2). This method has been increasingly used in health sciences research and is more effective for reducing bias compared with traditional approaches that consider all covariates to be potential confounders and automatically adjust for them.30 31 To study the association between smoking and outcomes, we controlled for age, sex, race, and AUD. For the association between AUD and outcomes, we controlled for age, sex, race, and smoking status. Based on previous literature, age, race, and sex were associated with both smoking status and AUD32 and each outcome.33 Smoking status was associated with AUD.34 Number of ribs fractured, ISS, and AIS body region score were intermediates that were not considered as confounders in the association between smoking status or AUD and pulmonary complications or mortality outcomes. Statistical significance was assumed at α<0.05. All analyses were performed on SAS V.9.4 (SAS Institute).

Directed acyclic graph for smoking. Minimal sufficient adjustment sets for estimating the total effect of smoking on complications or death: age, sex, race, and alcohol use. AIS, Abbreviated Injury Scale; ISS, Injury Severity Score.
{kind=link}
{kind=link}
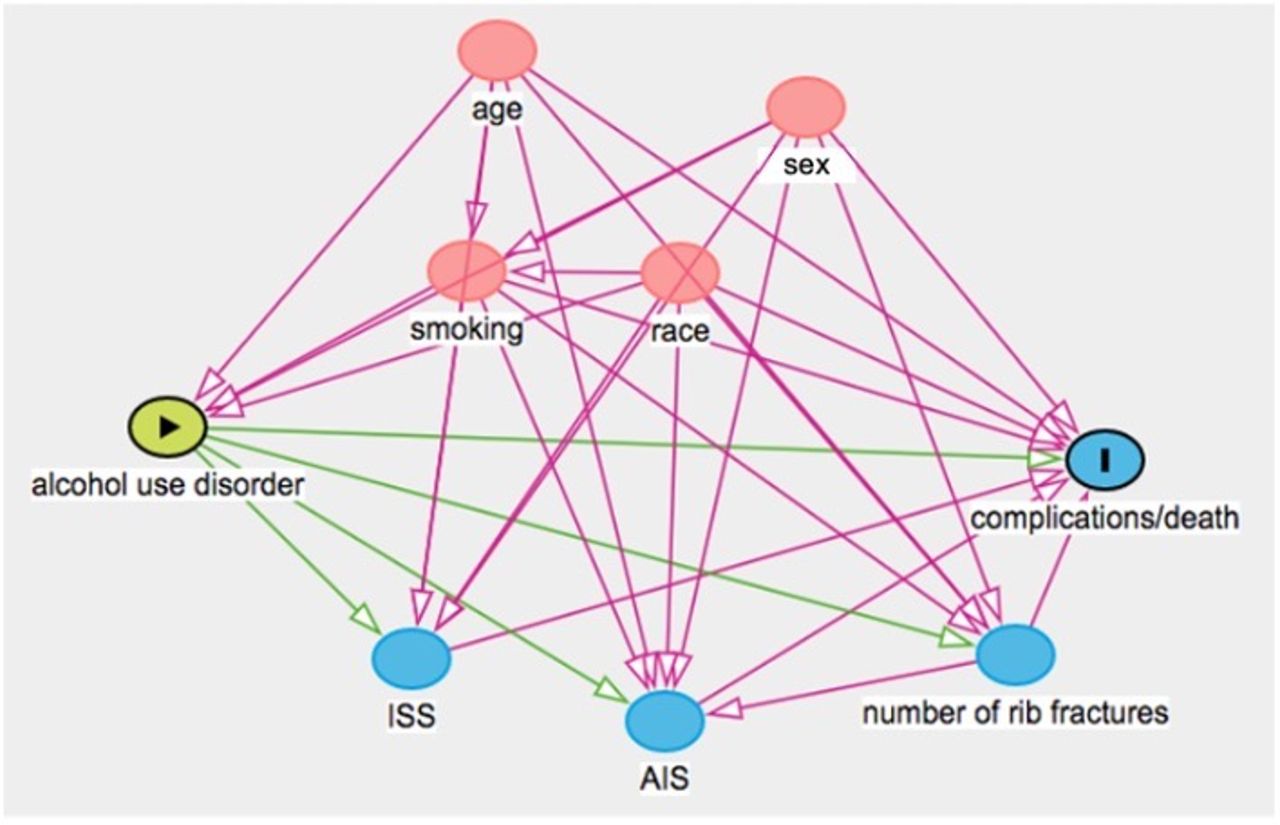
Directed acyclic graph for alcohol use disorder. Minimal sufficient adjustment sets for estimating the total effect of alcohol use disorder on complications or death: age, sex, race, and smoking. AIS, Abbreviated Injury Scale; ISS, Injury Severity Score.
Results
The initial query of our trauma database identified 2112 patients with one or more ribs fractured who were admitted to our ACS-verified level 1 adult trauma center from 2015 through 2019. After exclusions, the final cohort was composed of 1880 patients: 693 (36.9%) were smokers and 204 (10.9%) had AUD. No data were missing from the key exposure variables and minimal data were missing from demographic variables. Missing data were excluded from tables 1 and 2. The variable with the highest amount of missing data was age, which was missing in 1.3% of patients.
Descriptive analysis for demographics and outcomes in patients with traumatic rib fractures based on smoking status
Multivariable logistic regression for the risk of pulmonary complications and mortality based on smoking status in patients with traumatic rib fractures
Smoking status
In a comparison of smokers and non-smokers using bivariate analysis, smokers were younger, more often male, and more likely to have AUD (table 1). Smokers had a lower rate of in-hospital mortality (2.2% vs 4.8%; p=0.004) (table 1). In a multivariable regression comparing smokers with non-smokers, the likelihood of pneumonia or VAP, ARDS, or pneumothorax was not significantly different after adjusting for age, sex, race, and AUD (table 2). Mortality was 52% less likely among smokers compared with non-smokers (OR 0.48; 95% CI 0.27 to 0.87; p=0.014) in an adjusted model (table 2).
Alcohol use disorder
In comparing patients with AUD with those without AUD using bivariate analysis, patients with AUD were older, more often male, and more likely to be smokers (table 3). Patients with AUD also had different numbers of ribs fractured; different AIS thorax body region scores and spent more days in the hospital, in the ICU, and on the ventilator. Patients with AUD had higher rates of pneumonia (19.6% vs 11.8%; p=0.002) and lower rates of pneumothorax (12.7% vs 22.3%; p=0.002) (table 3). In a multivariable regression comparing patients with and without AUD for the likelihood of pulmonary complications with adjustment for age, sex, race, and smoking status, patients with AUD had a higher likelihood of pneumonia or VAP (OR 1.82; 95% CI 1.24 to 2.68; p=0.002) and a lower likelihood of pneumothorax (OR 0.51; 95% CI 0.33 to 0.75; p=0.002). AUD diagnosis was not significantly associated with likelihood of ARDS (table 4). The likelihood of mortality was not significantly different among patients with and without AUD in an adjusted model (table 4).
Descriptive analysis for demographics and outcomes in patients with traumatic rib fractures based on alcohol use disorder diagnosis
Multivariable logistic regression for the risk of pulmonary complications and mortality based on alcohol use disorder diagnosis in patients with traumatic rib fractures
Discussion
Our findings from a retrospective, single-institution database study over 5 years confirmed previous studies that in patients with rib fractures caused by blunt trauma, smoking was associated with a decreased risk of mortality and AUD was associated with an increased risk of pneumonia. We also found that AUD was associated with a decreased risk of pneumothorax. These results were based on regression analyses controlling for demographic variables of age, sex, race, and smoking or AUD. Previous studies have shown that pulmonary complications and mortality are associated with ISS and number of ribs fractured.1 35 We did not control for these variables because we only controlled for covariates that were known confounders, not intermediates.
Grigorian et al performed a retrospective analysis of the TQIP database and found that smokers with rib fractures experienced nearly a 40% decreased risk of in-hospital mortality compared with non-smokers (p<0.05), despite having higher rates of pneumonia.20 Our findings reinforce that smoking is associated with a decreased risk of in-hospital mortality (p<0.05). Our results differed from Grigorian et al when examining pneumonia rates between these two groups; we found that patients who smoked were no more likely to get pneumonia than non-smoking patients. This result supports the conclusions of a single-center retrospective study by Marco et al, which determined that smoking was not associated with increased risk of pneumonia in patients with traumatic rib fractures.23
Previous research has demonstrated a ‘smoker’s paradox’: smokers with cardiovascular disease have improved outcomes compared with non-smokers with similar disease.36–38 Studies examining trauma patients who smoke demonstrated that smoking did not increase risk of pneumonia, ARDS, or mortality.21 22 39 Our study provides additional support that the smoker’s paradox may exist in patients hospitalized with rib fractures. Hypothesized pathophysiologic mechanisms to explain these findings have focused on the demonstrated effects of cigarette smoke or its individual components, including nicotine and carbon monoxide (CO). Nicotine acts as a vasoconstrictor in the peripheral vasculature by direct action and by promoting release of epinephrine and norepinephrine,40–42 which could be responsible for maintaining blood pressure and limiting blood loss.43–45 CO may also have contributory vasoactive effects.41 42 The hemostatic effects of cigarette smoking could also contribute to the smoker’s paradox in trauma patients.22 Cigarette smoke promotes coagulation through platelet activation,46–48 effects on blood cells and components,41 49 and endothelial changes.50–52 Finally, the anti-inflammatory effects of nicotine could contribute to the paradox.53 54 When considered together, these mechanisms provide a plausible explanation for the physiologic and biochemical mechanisms of the reduction of in-hospital mortality in this population.
Chronic alcohol exposure is associated with pneumonia and other adverse outcomes in trauma patients.27 Recent studies of trauma patients with rib fractures have shown an association between AUD and higher rates of pneumonia.23 24 Vartan et al also found an association with AUD and higher rates of ARDS and mortality.24 Our results support previous findings of an association between AUD and higher rates of pneumonia; however, we did not observe a higher rate of ARDS, potentially due to low incidence. Our results showed that patients with AUD had a trend toward increased risk of in-hospital mortality, but the association was not statistically significant. Marco et al found no association of pneumothorax in patients with AUD,23 but we found a lower rate of pneumothorax in patients with AUD. Possible explanations for the discrepancy are that their sample size was smaller (n=152) or that the two populations were different in terms of risk factors for pneumothorax that were not measured. Our results add to another recent study that found a surprising inverse relationship between pneumothorax and mortality in patients with rib fractures.2 These findings could be associated with statistical limitations of retrospective design.
There are established associations between AUD and pneumonia or pulmonary inflammation.55 Proposed pathophysiologic mechanisms for this association are multifaceted: increased risk of aspiration,56 decreased upper-airway mucociliary clearance of bacterial pathogens,57 and impaired pulmonary host defenses.58–60 Inflammation can be further exacerbated in this demographic because of a diminished ability to manage oxidative stress and reduced ability to tolerate the fluid accumulation associated with trauma or pneumonia.61 62
A limitation of our study is the possibility of uncontrolled covariates acting as confounders. We made a concerted effort to mitigate this limitation by using DAGs to identify relationships between variables (figures 1 and 2). We chose to control for confounders and not to control for mediators (ie, ISS). Controlling for covariates that are not confounders increases the risk of collider bias or switchover effects, which we hoped to avoid.63 64 The limitation caused by control variable selection has been discussed specifically in the context of the smoker’s paradox.65 As with any retrospective study, unmeasured covariates could have affected the results. These could include certain comorbidities (eg, chronic obstructive pulmonary disease), vital signs (eg, heart rate and blood pressure), and Glasgow Coma Scale. Another limitation associated with the retrospective design is that missing data or inaccurate documentation or coding may have affected the results. We identified patients as smokers or AUD based on patient charts, which are subject to missing or inaccurate data. We did not evaluate the quantity of smoking or alcohol use for each patient, which is an important consideration for future research. Additionally, analysis of some less common complications may have been limited by sample size. Finally, this study was conducted at a single institution in a rural state and results may not be generalizable to other settings.
The results of the primary objective of this study fit within existing literature. We isolated a unique patient population because the study site is the only ACS-verified level 1 trauma center in a rural state. This population has distinct characteristics and is relatively under-represented in national databases, but our results were similar to previous studies. This replication establishes a strong basis for the external validity of our analysis and the generalizability of these findings to other similarly situated trauma centers. To maintain internal validity, multivariate analysis controlling for confounders identified by DAGs was used.
Future research should continue to isolate demographics that are under-represented in national trauma databases to further improve the generalizability of current rib fracture analyses. There is also a need to examine more patient characteristics and injury factors to establish reliable predictors for outcomes. Finally, basic science research is needed to evaluate the mechanisms of unexpected findings in recent retrospective studies, including the associations between smoking and mortality.
Conclusions
Our study found that in patients with rib fractures caused by blunt trauma, smoking was associated with decreased mortality and AUD was associated with increased risk of pneumonia. Additional studies are needed to further investigate the relationship between these exposures and outcomes in patients with rib fractures.
Data availability statement
No data are available.
Ethics statements
Ethics approval
Ethics approval was obtained from the Institutional Review Board at the University of Arkansas for Medical Sciences (IRB 260130). Informed consent was not required, as this was a retrospective analysis of a deidentified dataset.
Acknowledgments
The authors would like to acknowledge the contributions of Ms Judy Bennett, Ms Monica Kimbrell with UAMS Trauma Registry database, and the UAMS Translational Research Institute.
References
Footnotes
Contributors AG and JCB performed the literature search, conceptualization, and writing of the manuscript. JJ performed statistical analysis and writing. HKJ, AB, JM, KWS, and RR contributed to study design, conceptualization, and editing. KJK oversaw the project, including study design, conceptualization, methodology, and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.