Article Text

Abstract
Background Recent studies suggest a large proportion of musculoskeletal injuries are simple stable injuries (SSIs). The aim of this study was to evaluate whether direct discharge (DD) from the emergency department (ED) of SSIs is non-inferior to ‘traditional care’ regarding treatment satisfaction and functional outcome, and to compare other patient-reported outcomes (PROMs), patient-reported experiences (PREMs), resource utilization, and adverse outcomes before and after DD.
Methods This trial compared outcomes for 11 SSIs 6 months before and after the implementation of DD protocols. Pre-DD, patients were treated according to local protocols. Post-DD, patients were discharged directly using removable orthoses, discharge leaflets, smartphone application, and telephone helpline. Participants received a 3-month postinjury PROM/PREM survey to assess treatment satisfaction (Visual Analog Scale, VAS), pain (VAS), functional outcome (four validated questionnaires), and health-related quality of life (HR-QoL; EuroQol-5D). Resource utilization included general practitioner (GP) visit (yes/no), physiotherapist visit (yes/no), return to work/school/sports (days), work/school absenteeism to visit hospital (yes/no), number of hospital visits, and follow-up X-rays. Other outcomes included missed injuries (additionally to SSI) and adverse outcomes (delayed union, non-union). Between-group differences were assessed using propensity score-adjusted regression analyses. Non-inferiority was assessed for satisfaction and functional outcome using predefined margins.
Results 348 (pre-DD) and 371 (post-DD) patients participated; 144 (41.4%) and 153 (41.2%) patients completed the survey. Satisfaction and functional outcome post-DD were non-inferior to traditional care. Mean satisfaction was 8.13 pre-DD and 7.95 post-DD (mean difference: −0.16, p=0.408). Pain, HR-QoL, GP/physiotherapist visits, and return to work/school/sports were comparable before and after DD. Work absenteeism was higher pre-DD (OR 0.110, p<0.001), as well as school absenteeism (OR 0.084, p<0.001). Post-DD, the mean number of hospital visits and X-rays reduced: −1.68 (p<0.001) and −0.26 (p<0.001). Missed injuries occurred once pre-DD versus twice post-DD. There were no adverse outcomes.
Discussion The results of this study confirm several SSIs can be discharged directly from the ED without compromising patient outcome/experience. Future injury-specific trials are needed to conclusively assess non-inferiority of DD.
Level of evidence II.
- fractures
- bone
- orthopaedics
- patient outcome assessment
- patient satisfaction
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
In the Netherlands, 656 000 of 2 million annual emergency department (ED) visits concern injuries, 40% of which are fractures.1 Traditionally, patients with fractures are reviewed in a fracture clinic approximately 1 week after their initial assessment in the ED. Consequently, fracture clinics are often characterized by referrals of large numbers of unselected patients with minor injuries that do not (necessarily) require intervention.2 This frequently leads to recurrent unnecessary reviews and a high workload, which inevitably have consequences for patient experience, staff morale, training, and quality of care. Therefore, recently, a Virtual Fracture Clinic (VFC) model was introduced in several hospitals in the UK to optimize and streamline outpatient trauma care.2–6
The VFC model consists of two main components.2 4 The first component is direct discharge (DD) from the ED of patients with simple stable injuries (SSIs). DD is based on the idea that most patients with SSI require reassurance and information, but not routine review, as it is highly likely their injuries have excellent outcome with early mobilization.4 The second component is a ‘virtual’ review of all other ED patients with musculoskeletal injuries (ie, not discharged directly).2–6 During this consultant-led VFC review, patients are triaged to an appropriate patient-centered pathway, aiming to reduce unnecessary and untimely follow-up appointments. Typically, DD of SSIs is implemented prior to the implementation of a VFC review.7
DD has been studied for several SSIs within the United Kingdom (UK), including, among others, Mason type 1 radial head fractures,8 9 fifth metacarpal neck fractures,8 10 11 base of fifth metatarsal fractures,8 12 13 buckle-type fractures of the distal radius, and pediatric clavicle fractures.14–18 These studies indicate that DD reduces follow-up appointments, imaging, no-shows, and costs without compromising outcome and experience. To our knowledge, however, no studies have been performed outside the UK, whereas it is important to externally validate and evaluate effects in other settings, such as a different country.
The aim of this study was to evaluate whether DD of SSIs in a large urban district teaching hospital in the Netherlands was non-inferior to traditional care in terms of satisfaction with treatment and functional outcome, as well as to compare other patient-reported outcomes (PROMs), patient-reported experiences (PREMs), adverse outcomes, and resource utilization before and after the implementation of DD.
Methods
Design
This was a prospective, non-inferiority before-and-after study performed in the OLVG West Hospital, a level 2 trauma center in Amsterdam, the Netherlands, between November 15, 2019 and November 15, 2020, comparing DD versus ‘traditional’ fracture care. DD protocols were implemented at the midpoint of this study (May 20, 2019), dividing patients into a pre-DD cohort and a DD cohort.19
Direct discharge of simple stable injuries
Prior to the start of this study (October 2018), consensus was reached by our team of (orthopedic) trauma surgeons regarding the eligibility of injuries for DD and their corresponding treatment (table 1). For most injuries this was based on previous studies.2–6 8–17 20–22 Isolated ‘greenstick-type’ distal radius fracture, avulsion fracture of the ankle, and bicycle spoke injury were deemed eligible for DD based on expert opinion.
Simple and stable injuries, criteria and immobilization
Treatment
Traditional care
Before implementation of DD (pre-DD cohort), all patients with SSIs were treated in the ED according to local protocols. This often involved casting or splinting in the ED and at least one follow-up appointment in the fracture clinic after approximately 1 week.
Direct discharge
After implementation of DD (DD cohort), all patients with SSIs were treated in the ED using removable immobilization such as a bandage or brace (table 1). In the ED, physicians provided extensive verbal instructions and information relating to the injury and the expected recovery. This information was also summarized in a discharge leaflet. A smartphone application was available for iOS and Android containing digital versions of the discharge leaflets, videos of physical exercises to improve recovery, and videos explaining how to reapply immobilization after removal. A telephone helpline was available during mornings of weekdays in the event of questions and concerns or if the patient requested a review. Eligibility for DD was reassessed the next morning by a (orthopedic) trauma surgeon and radiologist during a routine daily review of cases and X-rays of all ED patients. This daily assessment was already part of our treatment process prior to the implementation of DD and acts as safety netting to identify missed injuries or patients treated incorrectly. In case patients were discharged directly incorrectly (ie, the injury was not an SSI), further face-to-face follow-up was scheduled by telephone. In case a patient with an SSI was not discharged directly, the patient was treated according to previous standards.
Recruitment and consent
During the study period all consecutive patients who presented to our ED with an isolated SSI were asked to participate. Patients were included only after obtaining written informed consent. Exclusion criteria were inability to understand/complete a Dutch survey, initial treatment in the ED of a different hospital, multiple injuries, reason for follow-up other than the SSI (eg, social care reasons), eye/motor/verbal score <15 at presentation, high-energy trauma, treatment continued in different hospital (eg, closer to home), and alcohol/drug intoxication.
Outcomes
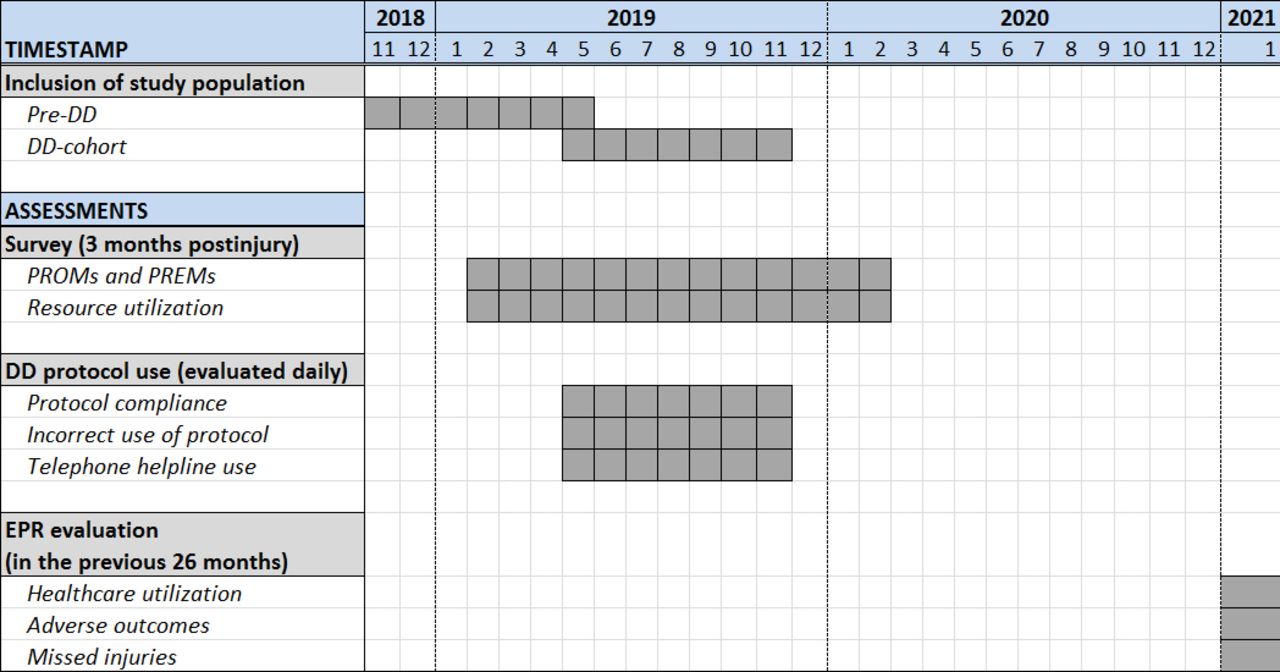
The primary outcomes of interest were satisfaction with treatment and functional outcome. For these outcomes, non-inferiority of DD versus traditional care was assessed using predefined non-inferiority margins (minimal clinically important difference, MCID; table 2).23–26 All outcomes were categorized into ‘PROMs and PREMs’, ‘Resource utilization’, and ‘Safety and use of DD protocols’ (figure 1).

Timeline depicting patient inclusion and assessments of outcomes. DD, direct discharge; EPR, electronic patient record; PREM, patient-reported experience measure; PROM, patient-reported outcome measure.
Different questionnaires used to assess satisfaction, functional outcome, and quality of life
PROMs and PREMs
All PROMs and PREMs were assessed using a 3-month postinjury survey, administered either online through Castor Electronic Data Capture27 or by postal mail. In case of non-response, two reminders were sent, followed by one telephone reminder. Satisfaction with treatment was assessed using Visual Analog Scale (VAS), ranging from 0 (very dissatisfied) to 100 (very satisfied), and using a 5-point Likert scale. Pain was assessed on a VAS from 0 (no pain) to 100 (extremely painful). The VAS satisfaction and VAS pain scores were converted from a scale of 0 to 100, to a scale of 0 to 10. The 5-point Likert satisfaction scale was dichotomized into ‘dissatisfied’ (‘very dissatisfied’, ‘dissatisfied’) and ‘not-dissatisfied’. Functional outcome was assessed using four different validated questionnaires: Shortened Version of the Disabilities of the Arm, Shoulder and Hand (QuickDASH),28 Lower Extremity Functional Scale,29 Short Form of the Patient-Reported Outcomes Measurement Information System (PROMIS) Upper Extremity, and Short Form of the PROMIS Mobility.30 The specific type of functional outcome questionnaire per patient was based on the region of injury and age (table 2). These separate functional status scores were also converted to one 0 to 100 scale to allow analysis of this outcome for the whole study population. Health-related quality of life (HR-QoL) was assessed using the EuroQol-5D (EQ-5D) questionnaire and the EQ-VAS.31 Proxy versions of the questionnaires were used for children aged 4 to 7, and children aged 8 to 17 received either a self-complete version or a proxy version based on their preference. More detailed information about the administered questionnaires, outcome ranges, and non-inferiority margins can be found in table 2. Treatment preference was assessed by providing a text explaining the principles of traditional care versus DD and asking which treatment the patient would prefer.
Resource utilization
The 3-month postinjury survey was also used to assess the number of times patients visited their general practitioner (GP) and physiotherapist for the treatment of their injury (during the previous 3 months), and if applicable the number of days after which they returned to work (return-to-work), school (return-to-school), and sports (return-to-sports), as well as work and school absenteeism (ie, the number of missed workdays or schooldays to attend follow-up appointments). All these outcomes were dichotomized into ‘yes’ and ‘no’.
Participants’ electronic patient records (EPRs) were accessed by THG during the second and third week of January 2021, that is, the follow-up for these data differed per patient, ranging from 14 months for patients included in November 2019 to 26 months for patients included in November 2018. Data were extracted on patients’ healthcare utilization, including total number of hospital visits (categorized into ‘with physician’ or ‘with plaster technician for cast/brace issues’) and imaging (number of X-rays, CT scans, MRI scans).
Safety and use of DD protocols
The EPR evaluation was also used to assess if adverse outcomes of treatment of the SSI had occurred, including delayed union and non-union, and if this was the case: treatment outcome and whether secondary surgery was performed (yes/no). Furthermore, it was assessed whether any missed injuries were identified during follow-up (ie, in addition to the SSI).
During the first 6 months after which DD protocols were implemented (ie, May 20, 2019–November 15, 2019), a researcher (either THG or SA) was present during the daily review of all ED X-rays to assess protocol compliance, which was defined as the proportion of patients with an SSI who were actually discharged directly. Incorrect use of DD protocols was assessed as well, defined as the number of patients who were discharged directly by the ED but recalled based on the daily X-ray review. Additionally, the total number of telephone helpline contacts was recorded during this period using a simple paper registration sheet.
Using EPRs and the aforementioned survey, various baseline characteristics were assessed, including age (years), gender, type of SSI (see table 1), and employment status (work/school/none).
Statistical analysis
Statistical analysis was performed using SPSS V.27.0 and STATA V.16.32 33 Analyses were performed for two groups separately. That is, healthcare utilization, missed injuries, and adverse outcomes were assessed for all patients who provided informed consent to access their EPR; survey outcome measures were analyzed only for patients who completed the survey. Baseline characteristics were reported using descriptive statistics for both groups separately, using mean with SD or median with IQR as appropriate.
Differences between pre-DD cohort and DD cohort were assessed using regression models, adjusted for patients’ propensity scores to deal with the non-randomized nature of this study. A propensity score indicates the probability of a patient being assigned to an intervention group, given a set of baseline characteristics.34 In our study, the propensity score was estimated using cohort (pre-DD cohort/DD cohort), age, gender, and injury type, using the pscore package in STATA. For continuous data, linear regression was performed using patients’ cohort and propensity score as independent variables and outcome as dependent variable, resulting in a mean-adjusted between-group difference, corresponding 95% CI, and p value. In case of non-normally distributed continuous data, bias corrected and accelerated bootstrapping was performed using 5000 replications to estimate uncertainty. For dichotomous or categorical data, binary logistic regression was performed in a similar manner. For DD to be considered non-inferior to ‘traditional’ care in terms of satisfaction and functional outcome, the predefined non-inferiority margins (table 2) should not be included in the corresponding 95% CIs. For all other comparisons, a p value of <0.05 was considered statistically significant.
Patient and public involvement
Patients were not involved in the design, intervention, research question, or outcome measures of the current study.
Results
Before implementation of DD, 676 patients presented to our ED with an SSI and were treated according to local protocols (pre-DD cohort). After implementation of DD, 784 patients were discharged directly from our ED with an SSI (DD cohort). Of these patients, 348 and 371 agreed to participate in the pre-DD cohort and DD cohort, respectively (figure 2). The 3-month postinjury survey was completed by 144 and 153 patients in the pre-DD cohort and DD cohort, respectively (response rates 41.4% and 41.2%). Table 3 provides the patients’ baseline characteristics.
Baseline characteristics of participating patients
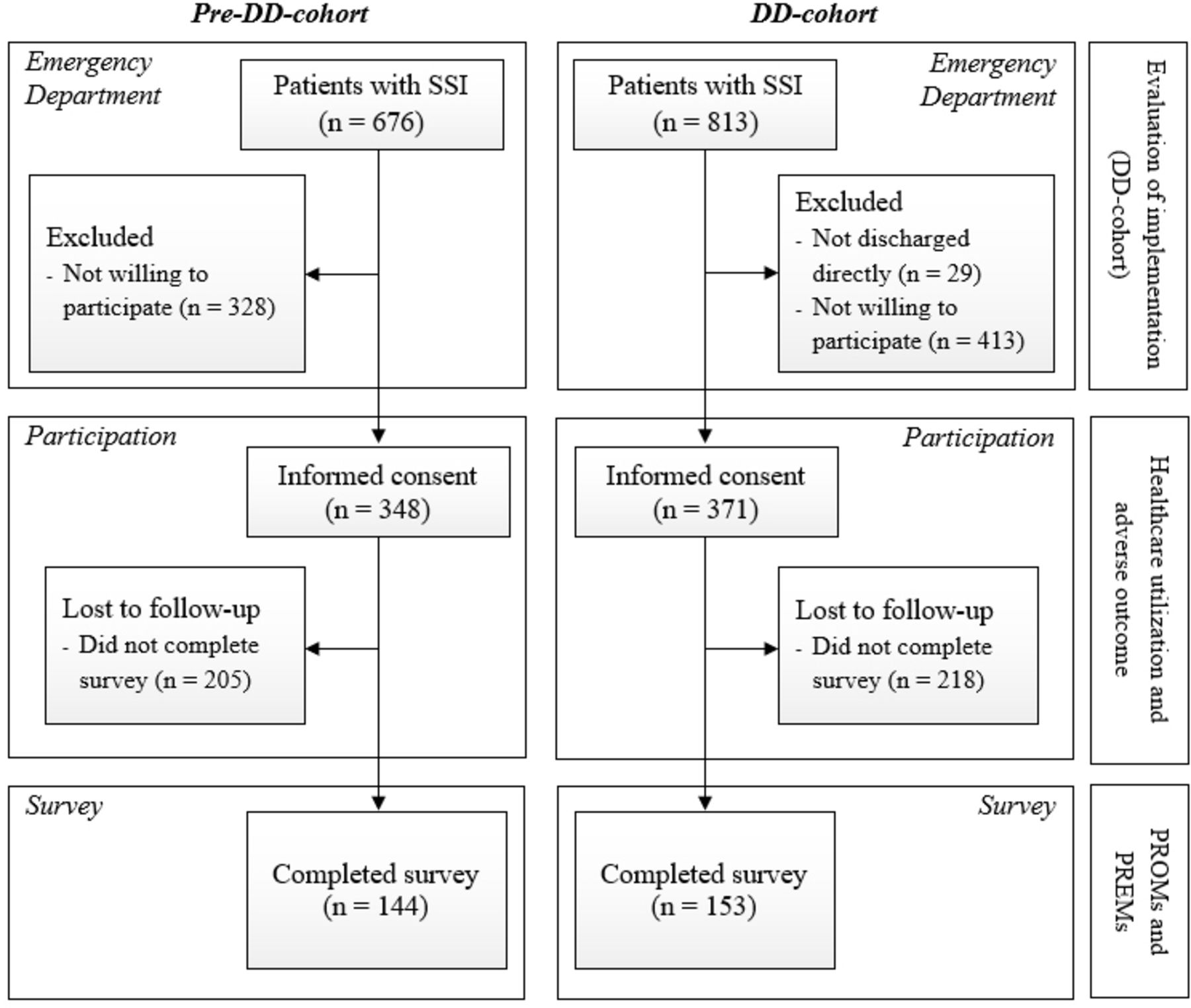
Flow chart depicting the inclusion of patients. In the DD cohort, patients in the emergency department with SSI were used to assess implementation. Patients who provided informed consent were used to assess healthcare utilization, and patients who completed the survey were used to assess patient-reported outcomes and experiences. DD, direct discharge; PREM, patient-reported experience measure; PROM, patient-reported outcome measure; SSI, simple stable injury.
PROMs and PREMs
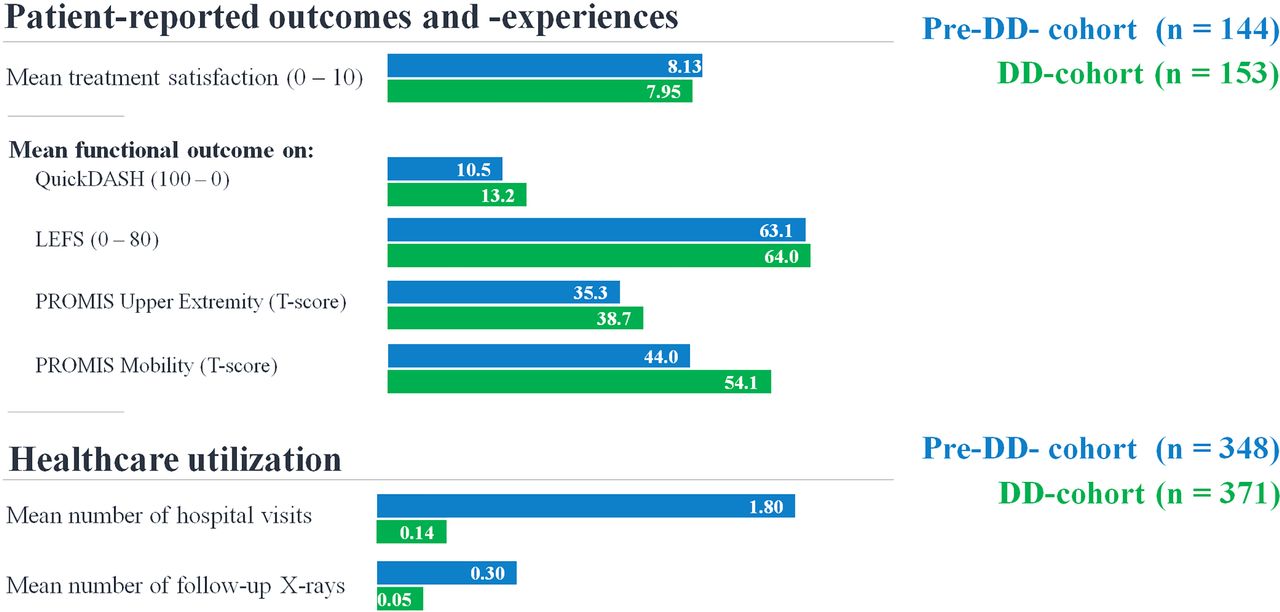
The predefined non-inferiority margins (see table 2) for satisfaction and functional outcome were not included in the 95% CIs surrounding the point estimates of these outcomes and hence non-inferiority was met. To illustrate, the predefined non-inferiority margin for satisfaction (−0.70) was not included in the 95% CI, which ranges from −0.53 to 0.21. The mean satisfaction with treatment on a VAS was 8.13 in the pre-DD cohort and 7.95 in the DD cohort (figure 3).

{kind=link}
{kind=link}
{kind=link}
Depiction of differences in satisfaction with treatment, functional outcome, and healthcare utilization before and after direct discharge. DD, direct discharge; LEFS, Lower Extremity Functional Scale; PROMIS, Patient-Reported Outcomes Measurement Information System; QuickDASH, Shortened Version of the Disabilities of the Arm, Shoulder and Hand.
Pre-DD, 5 patients (3.5%) were dissatisfied with treatment on the 5-point Likert scale versus 11 patients post-DD (7.2%; OR 2.05, p=0.197). There were no statistically significant differences in VAS pain scores (mean score 1.4 vs. 1.5, mean difference 0.078, p=0.727) or EQ-5D index and VAS scores. In the DD cohort, 81.7% of patients indicated to prefer DD over ‘traditional’ care versus 39.6% pre-DD. The mean differences in the functional outcome scores as well as all other PROMs/PREMs can be found in table 4.
Patient-reported outcomes and experiences at 3 months
Resource utilization
Return-to-sports, return-to-work and return-to-school were comparable before and after DD, as well as the proportion of patients who visited their GP or physiotherapist for treatment of their injury (table 5). Of the patients going to school, 57.6% missed one or more schooldays to attend a follow-up appointment in the pre-DD cohort versus 11.4% in the DD cohort (OR 0.084, 95% CI 0.023 to 0.253, p<0.001). Of the patients going to work, 44.8% missed one or more workdays to attend a follow-up appointment in the pre-DD cohort versus 8.2% in the DD cohort (OR 0.110, 95% CI 0.041 to 0.295, p<0.001).
Resource utilization
The mean number of hospital visits was 1.80 in the pre-DD cohort versus 0.14 in the DD cohort (mean difference −1.68, p<0.001). This included a mean reduction of 0.13 in plaster technician visits, for example, due to issues with a cast/brace/sling (p<0.001). The mean number of X-rays during follow-up was 0.30 in the pre-DD cohort versus 0.05 in the DD cohort (mean difference −0.26, p<0.001). A CT scan was performed once in the DD cohort to assess if there were any missed injuries in a patient with a fifth metatarsal fracture. No MRI scans were performed. There were 9 no-shows in the pre-DD cohort (2.6%) versus 0 in the DD cohort.
Safety and use of DD protocols
Delayed unions/non-unions and secondary surgeries of SSIs did not occur based on the EPR evaluation of all 719 participants. However, a ‘missed injury’ (in addition to the SSI) was diagnosed during follow-up in three cases: one in the pre-DD cohort and two in the DD cohort. In the pre-DD cohort, a patient with an avulsion-type fracture of the medial malleolus and navicular bone had further imaging 8 weeks after the ED visit (during regular follow-up). This revealed a proximal fracture of the fibula (ie, Weber C-type ankle fracture), which was treated surgically. In the DD cohort, one patient contacted the telephone helpline 1 week after a Weber A fracture due to persisting high levels of pain and was scheduled for review the next morning. Despite our daily X-ray review, radiographic imaging revealed a Weber B-type ankle fracture supination-external rotation stage 4. This was treated surgically. The other patient in the DD cohort was treated with an ankle brace after a Weber A fracture and contacted the telephone helpline twice, complaining of pain after starting weight-bearing. Further imaging revealed an additional fifth metatarsal base fracture that was treated conservatively by switching immobilization from an ankle brace to a walker boot.
During the 6 months after implementation of DD, there were 813 patients in our ED with an SSI, 784 of whom were discharged directly (protocol compliance 94.6%). During the same period, the telephone helpline was contacted 84 times. Furthermore, an additional 15 patients were initially discharged directly by the ED, but were recalled based on the daily screening of all X-rays by a (orthopedic) trauma surgeon and radiologist. This included 12 children treated as per adult DD protocols, 1 patient with a dislocated zone 2 fifth metatarsal fracture that exceeded our limit of 4 mm, and 2 patients with a zone 3 fifth metatarsal fracture.
Discussion
This first study on DD from the ED of patients with SSIs performed outside the UK shows that, in terms of satisfaction with treatment and functional outcome, DD is non-inferior to ‘traditional’ care with routine follow-up. Other patient outcomes including pain and HR-QoL, return-to-sports, return-to-work, and return-to-school all were comparable before and after DD. Furthermore, there were no adverse outcomes before and after implementation of DD. Hence, our findings support the idea that the SSIs included in this study can be discharged directly from the ED safely, that is, without compromising patient outcome and experience.
In previous studies on DD assessing satisfaction, it was often unclear whether this was related to the injury treatment or the DD/VFC process.35 In our study, patients were asked specifically to rate satisfaction with our treatment of their injury. We were of the opinion that this is a key parameter: that is, patients should retain comparable satisfaction levels with our services, in addition to a comparable functional outcome and regardless of the reduction of healthcare utilization.
The methods used to assess satisfaction in previous studies ranged from using either Likert scales,5 11 14 22 simple yes/no questions,8 to 1 to 10 VAS.10 15 All have advantages and disadvantages. For instance, the chances of acquiescence bias and ceiling effects are smaller using VAS,36 37 and children might prefer Likert scales.38 In the current study parents/caregivers were allowed to (help their child to) complete the survey. For these reasons, we used VAS as well as Likert scales to assess (dis)satisfaction. Both before and after DD, satisfaction with treatment was high, as is shown by the high mean satisfaction rate (VAS) as well as the low rate of dissatisfied patients (Likert). Moreover, a large proportion of patients who were discharged directly indicated they prefer DD over traditional care (81.7%), which is more or less comparable with Mackenzie et al8 studying DD of three SSIs (75%).
Although the aim of this study was to assess non-inferiority, it is noteworthy that the mean PROMIS Mobility T-score was 10 points higher in the DD cohort (indicating better outcome), whereas the MCID for this questionnaire is 2 to 3 points.26 It must be noted that the sample size for this questionnaire was small. Future studies are therefore needed to reassess this. As this was a remarkable finding we also performed a post-hoc analysis assessing treatment satisfaction of this particular subgroup and found that all patients rated their treatment ≥8.0 (VAS) and none indicated to be dissatisfied (Likert). The three other functional outcome scores were non-inferior after DD, and the mean summary scores of each individual questionnaire indicate that majority of patients with these SSIs have good functional outcome 3 months after injury.
Furthermore, our study indicates that adverse outcome rates are low, as was also shown in previous studies.8 9 12 13 20 However, it also emphasizes the importance of safety netting to include an available telephone helpline for questions and concerns, as well as the reassessment of X-rays of all DD patients by a (orthopedic) trauma surgeon before definitive treatment. One DD patient had surgery after a misdiagnosis (Weber B-type ankle fracture) 1 week after injury. In the Netherlands this is within the normal window for this procedure to be performed.
The reduced work/school absenteeism to attend a follow-up appointment indicates DD is also likely to be beneficial from a societal perspective. Furthermore, in our hospital, DD has drastically reduced healthcare utilization, and it is worth emphasizing that this study found no shift toward primary care (ie, GP or physiotherapist). In the Netherlands, approximately 256 000 fractures are diagnosed annually in EDs,1 85 000 of which are estimated to be SSIs (33%).4 Our mean reduction of 1.68 hospital visits per patient after DD is in line with previous comparative studies on DD of, for example, fifth metacarpal neck fractures (−1.78),10 fifth metatarsal fractures (−1.46),12 and the study by Mackenzie et al (−1.26).8 Based on our results, if DD would become standard of care for these SSIs in the Netherlands, the national reduction of hospital visits is estimated at 142 800 visits per year. Therefore, DD provides an excellent opportunity to reduce fracture clinic workload and healthcare costs.
Unfortunately, in many previous studies on DD, the classification of an SSI was limited to ‘minor’, ‘stable’, or ‘self-limiting’, or even unclassified.35 This complicates comparison with our results, as well as implementation and external validation of DD in other settings. Roughly speaking, however, studies on DD can be divided into two groups: (1) studies at the institutional level and (2) patient-level follow-up studies. The majority of the studies at an institutional level are non-comparative process evaluations of implementing (parts of) the VFC model.2–6 These studies typically include relatively large numbers of patients and provide information on the distribution of patients across the VFC model. Data regarding patients’ outcomes and experiences typically are limited, and therefore conclusions regarding the safety, effectiveness, and efficacy of DD for each individual injury cannot be drawn.
An important strength of this study is that a wide range of outcomes were evaluated in a before-and-after design, including hospital visits, imaging, satisfaction, functional outcome using validated questionnaires, and adverse outcomes. Consequently, our study provides both institutional-level information (eg, number of patients, protocol compliance, and telephone helpline use), as well as patient-level data of DD regarding patients’ healthcare utilization, PROMs, and PREMs. Apart from the study by Mackenzie et al8 on DD of radial head, fifth metacarpal and fifth metatarsal fractures, patient-level follow-up studies typically include only some of these outcomes. Furthermore, many of these studies did not directly compare DD with traditional care,9 11 13 20–22 and often patient outcome was not measured using validated questionnaires. Furthermore, although randomization at an individual patient level for treatment redesigns like DD might not always be feasible, to our knowledge no previous studies on DD have attempted to reduce the chances of ‘selection bias’ due to the non-randomized nature of their studies using methods such as the propensity score adjustment, which was used in the current study. To our knowledge, this is also the first study on DD to specifically assess non-inferiority of DD versus traditional care using predefined margins.
This study has several limitations. First, we studied the concept of DD, including multiple SSIs, and consequently subgroups of the included injuries were too small to analyze outcomes per injury. Second, numbers of patients far exceeding our numbers would have been needed to adequately assess differences in adverse outcomes like non-union. Third, as this was a before-and-after study, we did not include a priori non-inferiority sample size calculations of a predefined primary outcome. Fourth, PROMs and PREMs were assessed only once: at 3 months. Fifth, although part of DD, the patients discharged directly were not contacted routinely after a few weeks or months to assess their outcome and experience. This is a limitation especially for patients who did not complete the survey. We have evaluated all participants’ EPRs and found no adverse outcomes. This assumes patients experiencing any problems during their recovery would have returned to our hospital. However, we cannot be certain patients did not visit a different hospital for any issues. Furthermore, however, in keeping with what might be expected, the survey response rate in this study was fairly low, despite sending multiple reminders. Last, we asked patients after how many days they returned to work, school, or sports. Although based on our results we expect no between-group differences, we did not assess if patients had not yet returned to work/school or sports, at all.
Future studies on this topic should also assess the cost-effectiveness of DD versus traditional care. Although some relatively large injury-specific cohorts have been studied before, it is likely necessary to perform adequately powered studies for some of the other SSIs included in the current study before non-inferiority of DD can be assessed conclusively. Our smartphone application is now increasingly used by other hospitals in the Netherlands, and this might offer an opportunity to gather data in a collective and standardized way, allowing us to perform studies in much larger cohorts. Furthermore, these data can then be used to perform stratified analyses of outcomes per injury, allowing more fine-tuning of the DD protocols, for example, if these results would indicate certain patient characteristics (eg, higher age, cognitive impairment, language barrier) predict worse outcome. In the current study, 18% of DD patients indicated they would prefer traditional care. Future studies should further explore these patients’ motives. Last, future studies should evaluate if DD is suitable for other injuries, including pediatric injuries.
In conclusion, the results of this study on DD of SSIs confirm DD is an effective and safe alternative to traditional care with routine follow-up which does not compromise patient outcome and experience. This first study on this topic performed outside the UK indicates that DD is likely to produce satisfactory results in other countries as well. A large number of SSIs are diagnosed each year and consequently DD offers an opportunity to reduce healthcare costs and fracture clinic workload. The results of our study should be confirmed and strengthened by future larger injury-specific cohort studies. A collective (national) data registry could be established to accelerate this process, which should also encourage uniform data collection across multiple hospitals using validated and standardized outcome measures to improve comparability and strengthen findings.
Ethics statements
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the local ethical committee of OLVG Hospital (ref no 18.071) and by its board of directors.
References
Footnotes
Contributors THG was responsible for the conduct of this study, methodology, draft of the article, collection of data, and analysis of all data. SA supported the implementation of direct discharge and contributed to the writing of the article as well as collecting parts of the data. JJG supported the implementation of direct discharge as well as collecting parts of the data. JMvD contributed to the writing of the article and analysis of all data. RH, RNvV and JCG all contributed to the methodology of this study, implementation of direct discharge as well as writing of the article. JCG was the guarantor.
Funding This project was supported by an unrestricted grant from the health insurance company Zilveren Kruis Achmea (Leiden, The Netherlands). The funding source was not involved in the study design, data collection, analysis and interpretation, nor in the writing of the report or the decision to submit the article for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.