Article Text

Abstract
Background Von Willebrand factor (VWF) is an acute phase reactant synthesized in the megakaryocytes and endothelial cells. VWF forms ultra-large multimers (ULVWF) which are cleaved by the metalloprotease ADAMTS-13, preventing spontaneous VWF–platelet interaction. After trauma, ULVWF is released into circulation as part of the acute phase reaction. We hypothesized that trauma patients would have increased levels of VWF and decreased levels of ADAMTS-13 and that these patients would have accelerated thrombin generation.
Methods We assessed plasma concentrations of VWF antigen and ADAMTS-13 antigen, the Rapid Enzyme Assays for Autoimmune Diseases (REAADS) activity of VWF, which measure exposure of the platelet-binding A1 domain, and thrombin generation kinetics in 50 samples from 30 trauma patients and an additional 21 samples from volunteers. Samples were analyzed at 0 to 2 hours and at 6 hours from the time of injury. Data are presented as median (IQR) and Kruskal-Wallis test was performed between trauma patients and volunteers at both time points.
Results REAADS activity was greater in trauma patients than volunteers both at 0 to 2 hours (190.0 (132.0–264.0) vs. 92.0 (71.0–114.0), p<0.002) and at 6 hours (167.5 (108.0–312.5.0) vs. 92.0 (71.0–114.0), p<0.001). ADAMTS-13 antigen levels were also decreased in trauma patients both at 0 to 2 hours (0.84 (0.51–0.94) vs. 1.00 (0.89–1.09), p=0.010) and at 6 hours (0.653 (0.531–0.821) vs. 1.00 (0.89–1.09), p<0.001). Trauma patients had accelerated thrombin generation kinetics, with greater peak height and shorter time to peak than healthy volunteers at both time points.
Discussion Trauma patients have increased exposure of the VWF A1 domain and decreased levels of ADAMTS-13 compared with healthy volunteers. This suggests that the VWF burst after trauma may exceed the proteolytic capacity of ADAMTS-13, allowing circulating ULVWF multimers to bind platelets, potentially contributing to trauma-induced coagulopathy.
Level of evidence Prospective case cohort study.
- coagulopathy
- venous thromboembolism
- thromboembolism
- multiple trauma
Data availability statement
Data are available upon reasonable request. De-identified data used in this study are summarized in this article. Raw data or further de-identified information can be obtained via inquiry to the corresponding author: MP, Division of Trauma, Critical Care and General Surgery, Mayo Clinic, 200 First Street SW, Rochester, MN 55905; Tel: (507) 255-6960, Fax: (507) 255-9872, Park.Myung@mayo.edu.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The physiological response to trauma causes vascular damage directly through physical injury and indirectly through the acute phase response. Von Willebrand factor (VWF) is an important acute phase reactant synthesized in the megakaryocytes and endothelial cells (EC) as a single-chain propolypeptide of 2813 amino acids with repeat domains of D1-D2-D’-D3-A1-A2-A3-D4-C(1-6)-CK.1 2 Pro-VWF monomers form dimers through the CK domain, a variable number of dimers, then multimerize through the N-terminal disulfide bonds. This gives VWF a multidomain structure accessible to multiple cellular receptors.3–8 After synthesis, VWF multimers are either constitutively released into circulation or stored in the Weibel-Palade bodies of ECs and the alpha granules of platelets and megakaryocytes, where they form ultra-large VWF (ULVWF) multimers.9–11 In addition to their increased weight, these ULVWF multimers are intrinsically active and able to form high strength bonds with the GP1bα subunit of the GPIb-IX-V complex on platelets and trigger platelet aggregation.7 9 12
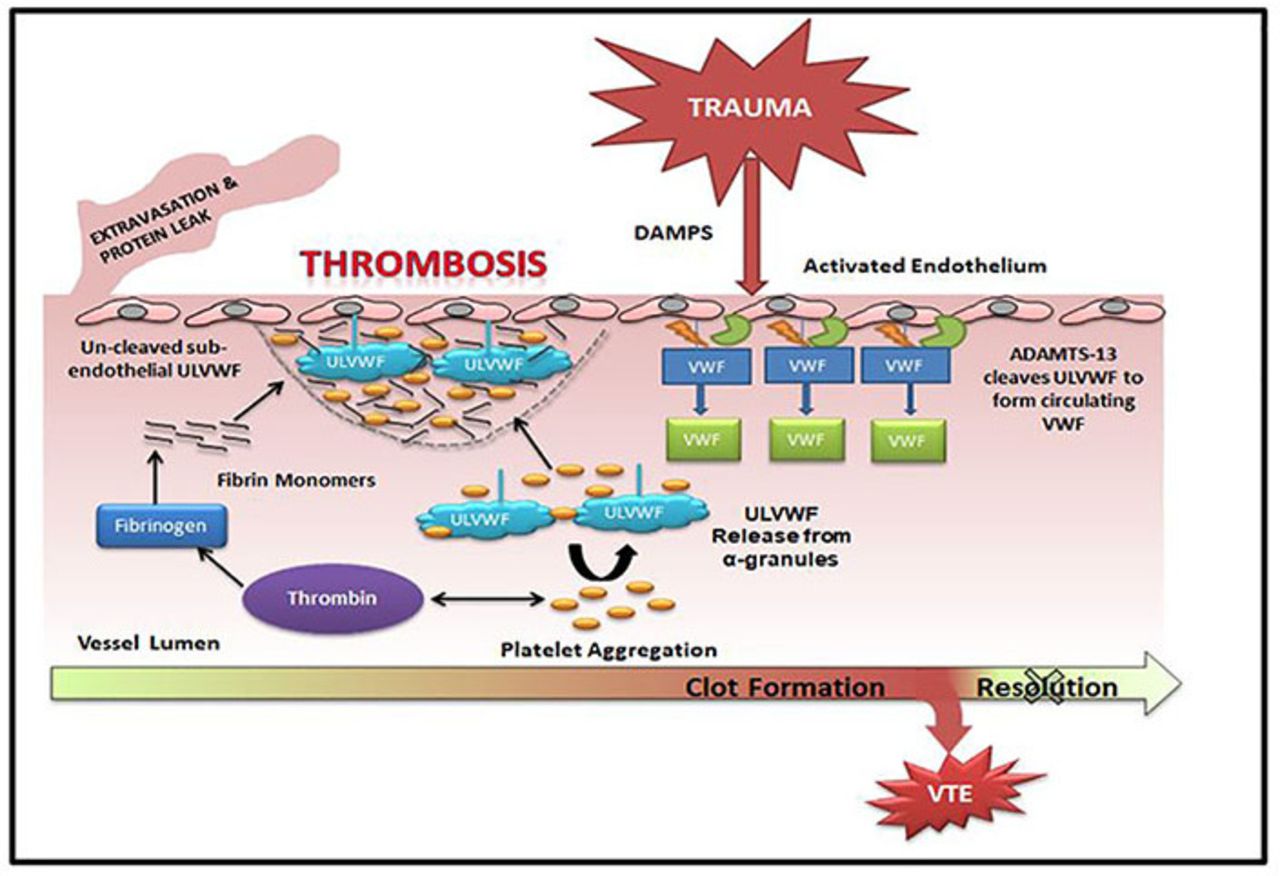
On release from activated ECs, ULVWF multimers are anchored to the EC surface, elongated by the fluidic shear stress, and rapidly but partially cleaved by the metalloprotease ADAMTS-13 to generate VWF multimers found in circulation. Under physiological conditions, these cleaved circulating VWF multimers adopt globular structures that bury the GPIbα-binding A1 domain so that they cannot spontaneously bind platelets.13–19 During acute injury, however, ULVWF multimers are released from activated or injured ECs as part of the acute phase reaction.20–24 When their release overwhelms the proteolytic capacity of ADAMTS-13, ULVWF multimers cannot be quickly cleaved to the circulating form, resulting in the accumulation of ULVWF multimers in plasma and on platelet and EC surfaces, contributing to thrombosis (figure 1).9 ,12 18 25

Mechanistic description of VWF release after trauma. This schematic describes VWF synthesis and release under physiological circumstances and after trauma, as well as the potential role of VWF in clot formation after trauma. ULVWF, ultra-large von Willebrand factor; VTE, venous thromboembolism; VWF, von Willebrand factor.
The role of VWF in trauma and trauma-induced coagulopathy (TIC) is incompletely understood. TIC describes a state of dysregulated coagulation after trauma with both hypocoagulable and hypercoagulable states.26 In addition to hemorrhagic complications, trauma patients are at high risk of venous thromboembolism (VTE), including deep vein thrombosis and/or pulmonary embolism, and accelerated thrombin generation kinetics have been shown to be predictive of VTE development after trauma.27–29 Prior in vitro studies have also shown that thrombin generation in platelet-rich plasma is decreased by neutralization of VWF, suggesting that VWF activates thrombin generation through a platelet-mediated and fibrin-mediated pathway30–32 (figure 1). Increased plasma VWF levels have been associated with poor outcomes after trauma, specifically after traumatic brain injury (TBI).33 34 Additionally, low ADAMTS-13 activity is associated with endothelial damage and mortality in patients with severe trauma.35 36 A recent murine model of TBI has demonstrated that administration of exogenous ADAMTS-13 either before or after injury improves neurological function, protects against TBI-induced vascular leakage and consumptive coagulopathy, and reduces mortality without impairment of baseline hemostasis.37
In this pilot study, we hypothesized that trauma patients would have greater levels of VWF and decreased levels of ADAMTS-13 compared with healthy volunteers and that trauma patients would have accelerated thrombin generation kinetics.
Patients and methods
Study design and sample source
Patient samples used in this pilot study were collected from a parent prospective case cohort study.32 Adult patients presenting to the Mayo Clinic Emergency Department as trauma activations were considered for inclusion. Exclusion criteria included age <18 years, refusal of consent or inability to obtain informed consent, ongoing systemic anticoagulation (eg, heparin, warfarin, or novel oral anticoagulants) other than antiplatelet agents (eg, aspirin, clopidogrel, non-steroidal anti-inflammatory drugs), known pre-existing coagulopathy, cirrhosis, active malignancy, sepsis, renal failure requiring dialysis, burn injuries, major surgery or another significant trauma within the last year, pregnant women, or prisoners. The time of injury (TOI) was determined by the prehospital medical providers based on information at the injury scene. Trauma patients or their legal authorized representative (LAR) were consented for this study after the collection of one or more blood samples. If the patient or LAR could not be consented for study participation or declined consent, the sample was destroyed and the patient was excluded. We collected demographic and clinical characteristics for each patient from the electronic medical record. Healthy volunteers were recruited specifically for this study from the local community. Volunteers provided full written informed consent prior to sample collection.
Sample collection, processing, and storage
Blood samples were collected at 0 to 2 hours and at 6 hours after the documented TOI. The collection of samples at 0 to 2 hours was done in the trauma bay, as close to the TOI as possible, but within 2 hours of injury. If a 6-hour sample was unable to be obtained, the baseline sample was still used. A total of 18 mL of whole blood was collected by venipuncture or from existing indwelling catheters into 4.5 mL citrated Vacutainer tubes (0.105 M buffered sodium citrate, 3.2%; Becton Dickinson, Plymouth, UK), processed to platelet-free plasma by double centrifugation (3000 g, 15 minutes) at room temperature (20°C–24°C), as recommended by the International Society on Thrombosis and Haemostasis (ISTH) Vascular Biology Scientific and Standardization Committee (SSC) Collaborative Workshop,38 and stored in multiple aliquots at −80°C until analysis. All samples were processed into platelet-free plasma within 1 hour of collection.
Calibrated automated thrombogram analyses
Thrombin generation was measured with the calibrated automated thrombogram (Thrombinoscope, Maastricht, The Netherlands), using a Fluoroskan Ascent plate reader (390 nm excitation, 460 nm emission; Thermo Electron, Vantaa, Finland), as previously described by Hemker et al.39 40 Assays of trauma patient samples were performed in triplicate. Corn trypsin inhibitor (50 µg/mL final concentration) was added to each plasma sample prior to analysis. Thrombin generation was initiated with addition of 20 µL of PPP (5 pM tissue factor and 4 µM phospholipid; Diagnostica Stago, Parsippany, NJ) reagent. Then, 80 µL of citrated platelet-poor plasma was added to each well of U-bottom 96-well microtiter plates (Nunc, Thermo Fisher Scientific, Rochester, NY) using a single channel pipette. After an incubation period (10 minutes at 37°C), 20 µL of warmed FluCa reagent (FluCa Kit, TS50, Thrombinoscope), which contains the fluorogenic substrate and CaCl2, was added to each well via an automated dispenser. Thrombin generation curves were recorded continuously for 90 minutes at a rate of three readings per minute. Separate wells containing the thrombin calibrator, which corrects for inner filter effects and quenching variation among individual plasmas, were also measured in parallel. A dedicated software program, Thrombinoscope (Diagnostica Stago, Maastricht, The Netherlands), was used to calculate thrombin activity over time. The parameters derived were lagtime (LT, minutes), time to peak (ttPeak, minutes), and peak height (PH, nM).
VWF and ADAMTS-13 analyses
The Rapid Enzyme Assays for Autoimmune Diseases (REAADS) Activity Kit (Corgenix, Broomfield, CO, USA), a sandwich ELISA that measures a monoclonal antibody specific for the platelet-binding A1 region of VWF, was performed per the manufacturer’s instructions using a 1:21 dilution of patient plasma. VWF antigen (VWF:Ag) levels were measured using quantitative sandwich ELISA (Thermo Scientific, Frederick, MD), according to the manufacturer’s instructions, with an 8000-fold dilution of patient plasma. ADAMTS-13 antigen (ADAMTS-13:Ag) levels were measured with sandwich ELISA (R&D Systems, Minneapolis, MN), performed according to the manufacturer’s instructions, using a 100-fold dilution of patient plasma. The ADAMTS-13:Ag to VWF:Ag ratio was also calculated to gauge the relative or kinetic deficiencies of ADAMTS-13.
Statistical analysis
Data analysis was performed using SAS V.9.4 (SAS Institute, Cary, NC). Statistics are presented as median values with IQR. Kruskal-Wallis test was used to detect differences in values between trauma and control patients. A p value <0.05 was considered significant. Analysis was performed on all trauma patient samples collected at 0 to 2 hours (n=22) and all samples collected at 6 hours (n=28) separately.
Results
Patient characteristics
A total of 50 plasma samples were collected from 30 trauma patients early after injury (samples collected at 0 to 2 hours from TOI, 6 hours from TOI, or both) and compared with plasma samples from 21 healthy volunteers, collected at a single time point. The median age of the trauma patients was 56 years (31–67), the Injury Severity Score (ISS) was 25.5 (18–32), and 18 of 30 (60%) were male. No patients in this study developed VTE within 90 days of injury. Four (13.3%) of the trauma patients died as a result of their injuries during the index hospital admission. Eleven (36.7%) of the trauma patients received blood transfusions within 24 hours of injury. Of these patients, six underwent massive transfusion per Mayo Clinic Trauma Center Protocol (damage control resuscitation with the goal of 1:1:1 packed red blood cells:plasma:platelets). A total of 20 samples were obtained from the 11 transfused patients, and 6 of these were obtained prior to initiation of any blood products. No patients underwent surgery prior to the collection of samples at 0 to 2 hours, and 14 of 30 (46.7%) underwent surgery prior to the collection of the 6-hour sample. With regard to race, 26 of 30 (86.67%) trauma patients were white, 2 identified as Asian and 1 identified as other. Detailed clinical information on each trauma patient, including ABO blood type, which is known to impact VWF levels, can be found in table 1.
Detailed clinical characteristics of all 30 trauma patients
Among the healthy volunteers, the median age was 43 years (34–56) and 9 of 21 (43%) were male. There was no statistically significant difference in age or sex between trauma patients and volunteers. Among the female volunteers, 7 of 12 (58.3%) were premenopausal, 6 of whom were taking a hormonal contraceptive, 3 of 12 were perimenopausal, and 2 of 12 were postmenopausal. Regarding race, 20 of 21 volunteers were white (95.2%) and 1 identified as Asian. Blood type was not available for 16 of 21 volunteers, 3 were O+, 1 was A+, and 1 was AB+.
VWF and ADAMTS-13 levels: trauma patients versus healthy volunteers
As described in table 2, VWF:Ag levels tended to be greater in trauma patients compared with healthy volunteers both at 0 to 2 hours and at 6 hours; however, this difference did not reach statistical significance.
VWF activity and thrombin generation kinetics in trauma patients versus healthy volunteers*
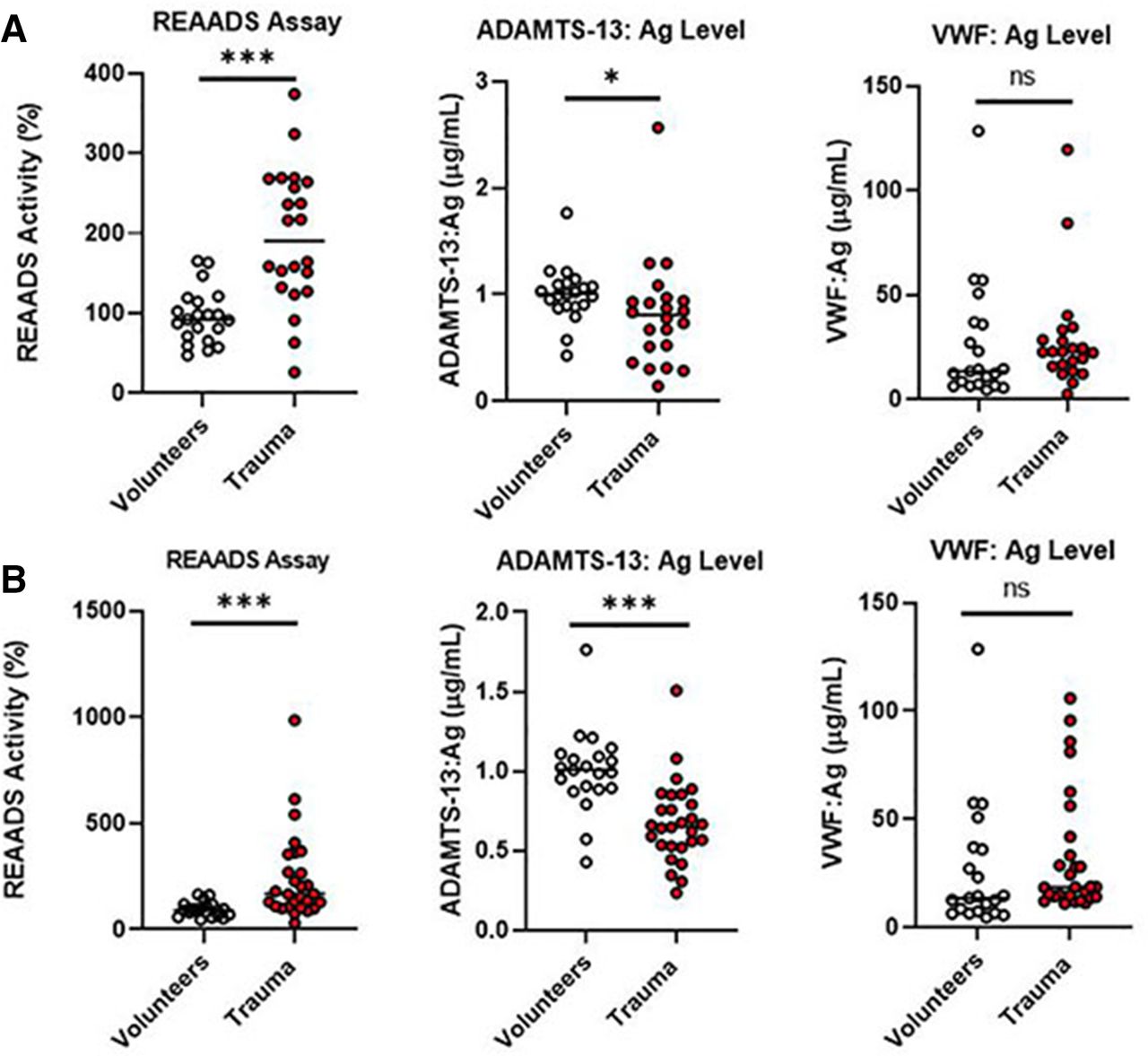
Healthy volunteers had a broad range of VWF:Ag levels (4.46−128.6 µg/mL), with the greatest value of 128.6 µg/mL in a volunteer exceeding the greatest value in trauma patients of 119.5 µg/mL (range 2.59−119 µg/mL), as can be seen in figure 2. This particular volunteer was an otherwise healthy individual in their 30s with no significant medical or surgical history and met our inclusion criteria based on our standard screening protocol. REAADS activity (exposure of the VWF A1 platelet-binding domain) was significantly greater in trauma patients compared with healthy volunteers at both time points (table 2). However, there was no significant difference in the ratio of REAADS activity to VWF:Ag level at either time point (table 2). ADAMTS-13:Ag levels were significantly decreased in trauma patients at both time points, and ADAMTS-13:Ag to VWF:Ag ratio was significantly lower in trauma patients at 6 hours, as described in table 2.
{kind=link}
{kind=link}
Individual values for trauma patients and healthy volunteers. Individual values plotted for (A) 22 samples from trauma patients at 0–2 hours from TOI vs. 21 healthy volunteers and (B) 28 samples from trauma patients at 6 hours from TOI vs. 21 healthy volunteers. Values for the REAADS assay (%), VWF:Ag level (µg/mL), and ADAMTS-13:Ag level (µg/mL) are shown. Solid lines represent median. Kruskal-Wallis test for significance: *p<0.05, **p<0.01, ***p<0.001. ADAMTS-3:Ag, ADAMTS-3 antigen; REAADS, Rapid Enzyme Assays for Autoimmune Diseases; TOI, time of injury; VWF:Ag, von Willebrand factor antigen.
Patients who received any blood transfusion prior to collection of their 6-hour sample (n=11) were compared with those who did not receive any transfusion (n=17). There was no significant difference found in VWF:Ag level (15.35 µg/mL (14.01–18.6) vs. 27.88 µg/mL (14.28–52.20), p=0.285), ADAMTS-13:Ag level (665 µg/mL (536–854) vs. 643 µg/mL (482–821), p=0.517), or REAADS activity (2706% (2100–7455) vs. 3780% (2762–6636), p=0.329) based on transfusion status.
Thrombin generation kinetics
Compared with the healthy volunteers, trauma patients showed accelerated thrombin generation kinetics with significantly decreased ttPeak and increased PH at both time points (table 2). Additionally, patients who received any blood transfusion prior to collection of their 6-hour sample (n=11) were compared with those who did not receive any transfusion (n=17). There were no significant differences in LT (4.00 minutes (3.33–4.74) vs. 4.67 minutes (3.62–5.28), p=0.221), PH (223.7 nM (199.7–237.7) vs. 228.6 nM (183.6–268.0), p=0.547), or ttPeak (7.30 minutes (6.00–8.33) vs. 7.50 minutes (6.28–8.95), p=0.397) between those who were transfused and those who were not.
Discussion
We are the first to demonstrate increased exposure of the VWF A1-binding domain in trauma patients using the REAADS assay. This is likely due to the quantitative increase in VWF:Ag level in trauma patients, rather than a conformational change that increases in the intrinsic activity of VWF, as there was no significant difference in the ratio of REAADS activity to VWF:Ag level between trauma patients and healthy volunteers at either time point in this study. However, we cannot make conclusions regarding conformational changes in VWF with these data alone.
Trauma patients in this study also had significantly decreased ADAMTS-13:Ag levels and ADAMTS-13:Ag to VWF:Ag ratios than healthy volunteers. This indicates a relative deficiency of ADAMTS-13 in trauma patients, potentially due to increased release of ULVWF multimers after trauma, as previously described by Dyer et al.41 This is also consistent with the findings of Wu et al,37 who showed improvement in neurological outcomes and reduced mortality in mice that were administered exogenous ADAMTS-13 before or after severe TBI, likely due to increased ULVWF release after injury overwhelming the proteolytic capacity of endogenous ADAMTS-13. Low ADAMTS-13 activity has also been associated with poor outcomes after pediatric trauma.35
Trauma patients tended to have increased VWF:Ag levels compared with healthy volunteers at both time points, but this difference was not statistically significant. This differs from other publications,35 including the recently published study by Dyer et al,41 who demonstrated a significant increase in the normalized VWF:Ag percentage in trauma patients. This difference is likely due in part to our small sample size, as well as an outlier with a higher than normal VWF:Ag level42 within our healthy volunteers. As such, individual variation impacted our results.
We also found an accelerated thrombin generation pattern among trauma patients, suggesting that the increased release of VWF after trauma could also be promoting thrombin generation, based on the platelet-driven and fibrin-driven mechanism that has been described in vitro.30–32 However, we are unable to draw conclusions about how VWF may influence thrombin generation after trauma based on these data alone.
This study has several limitations. First, this is a small single-center pilot study with primarily blunt trauma and may not be generalizable to other populations. None of the patients in this study developed VTE within 90 days of injury, so we also cannot draw conclusions about the association of VWF with VTE development after trauma, or with other clinical outcomes based on these data alone. Additionally, plasma VWF:Ag level is impacted by a number of factors, including age, race and ABO blood type,43–46 and these have can have inter-related effects. Type O blood has been associated with lower plasma VWF:Ag levels than other blood types, which may have impacted our results.43 45 46 Among the trauma group, 12 of 30 patients had type O+ blood (table 1). In the volunteer group, three patients had O+ blood; however, blood type was not available for 16 of 21 healthy volunteers. As such, it may be that these groups were not well matched for blood type, which can influence the plasma VWF:Ag level. Additionally, 12 of 21 (57.1%) healthy controls were female, with 6 patients on hormonal contraceptive and 5 patients in varying stages of menopause. Prior work has also suggested some variation in VWF:Ag level based on hormonal shifts,47 and although data in this area are limited this also may have influenced our results.
Ultimately, prevention of VTE remains a challenge in the trauma population. It is possible that targeted inhibitors that block prothrombotic activity of VWF with minimal impact on hemostasis may represent a future avenue to improve clinical outcomes for patients with severe trauma.48
Conclusion
In this pilot study, we showed that trauma patients have significantly increased exposure of the VWF A1 domain and significantly decreased levels of ADAMTS-13 relative to healthy controls. These early findings suggest that the VWF burst after trauma may exceed the proteolytic capacity of ADAMTS-13, allowing circulating ULVWF multimers to bind platelets, potentially contributing to TIC.
Data availability statement
Data are available upon reasonable request. De-identified data used in this study are summarized in this article. Raw data or further de-identified information can be obtained via inquiry to the corresponding author: MP, Division of Trauma, Critical Care and General Surgery, Mayo Clinic, 200 First Street SW, Rochester, MN 55905; Tel: (507) 255-6960, Fax: (507) 255-9872, Park.Myung@mayo.edu.
Ethics statements
Ethics approval
The study was approved by the Mayo Clinic Institutional Review Board (IRB #14-008481).
Acknowledgments
We would like to thank Timothy Halling, Joseph Immermann, Michael J Ferrara, Andrew Kirmse, and Joel Anderson for their essential contributions to this project in research support, coordination, and data generation. We would also like to thank the Mayo Clinic Center for Translational Science Activities (CTSA) and Clinical Research Unit (CRU) for their ongoing support in specimen collection and processing.
References
Footnotes
Contributors TAM, JG: data analysis and interpretation, article writing and critical revision. LMT: sample analysis, data acquisition, analysis and interpretation, critical revision of article. AT: study design and conduct, data analysis and interpretation, critical revision of article. KRB, GMS, J-FD: study planning, conception and design, data analysis and interpretation, critical revision of article. MA: study planning, conception and design, study conduct, data acquisition, analysis and interpretation, critical revision of article. RK: study planning, conception and design, data interpretation, critical revision of article. MP: study planning, conception and design, study conduct, sample and data acquisition, data interpretation, critical revision of article.
Funding This project was supported by R38HL150086 Stimulating Access to Research in Residency (TAM) from the National Heart, Lung, and Blood Institute (NHLBI), HL146508 from the NHLBI (MA), T32 AG049672 from the National Institute on Aging (NIA) and Robert and Arlene Kogod Center on Aging, Mayo Clinic (JG), R01 GM 1 26 086–03 (MP) from the National Institute of General Medical Sciences (NIGMS), UM1 HL120877-06 (MP) by the Trans-Agency Consortium for Trauma-Induced Coagulopathy (TACTIC), 1 UL1 RR024150 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), the NIH Roadmap for Medical Research, and by Grant Number UL1 TR000135 from the National Center for Advancing Translational Sciences (NCATS).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.