Article Text

Statistics from Altmetric.com
History
A 33-year-old female presented to the trauma center with multiple gunshot wounds to her left posterior axilla, right of midline in the upper back, and left lateral thigh. She complained that she did not have sensation in or an ability to move her left upper extremity.
Examination
The patient was screaming and uncooperative during the examination. Her systolic blood pressure was 110 mm Hg, heart rate was 138 beats per minute, and respiratory rate was 33 breaths per minute with audible breath sounds bilaterally. There was significant bleeding from her left posterior axillary wound, and this was packed with gauze. Her left upper extremity was cool with no palpable radial pulse nor Doppler signal, and she had no strength or sensation in this extremity. Palpable pulses were present in all other extremities.
Management
After blood was drawn for type and cross-match, two large bore intravenous catheters were inserted. Given her agitation and inability to cooperate with an examination, she was intubated using rapid sequence induction with 100 mg lidocaine, 150 mg propofol, and 100 mg rocuronium. With induction, she became hypotensive to a systolic blood pressure of 70 mm Hg.
Question
With the rapid decline in the patient’s systolic blood pressure, your choice for the next step in management would be:
Focused abdominal sonography for trauma (FAST) examination
Transfusion of blood products
Infusion of 1 liter lactated Ringer’s solution
Stat CT aortogram with contrast
Management
A Cordis central venous catheter was placed in her right femoral vein under ultrasound guidance, and she was transfused 1 unit of whole blood with a rise in her systolic blood pressure to 140 mm Hg. An extended FAST examination was performed and was negative for any blood in the pericardium, bilateral pleural spaces, or abdomen. An X-ray of her chest showed bullet fragments over her right clavicle and no evidence of an intrathoracic injury, while an X-ray of her abdomen and pelvis showed no evidence of injury or retained missiles. An X-ray of her left thigh showed a bullet in the superficial medial soft tissue.
The patient then underwent a CT arteriogram of her neck, torso, and left upper extremity. This showed that the bullet that entered the left posterior axilla had caused a complete transection of the third portion of the left subclavian artery with extravasation of contrast (figure 1). The left axillary, brachial, ulnar, and radial arteries did reconstitute distally, but with severely diminished caliber. The bullet tract was noted to extend across the retropharyngeal space into the right lobe of the thyroid raising a concern for an injury to the esophagus or trachea not detected on the CT scan. The carotid artery system and vertebral arteries were intact bilaterally.
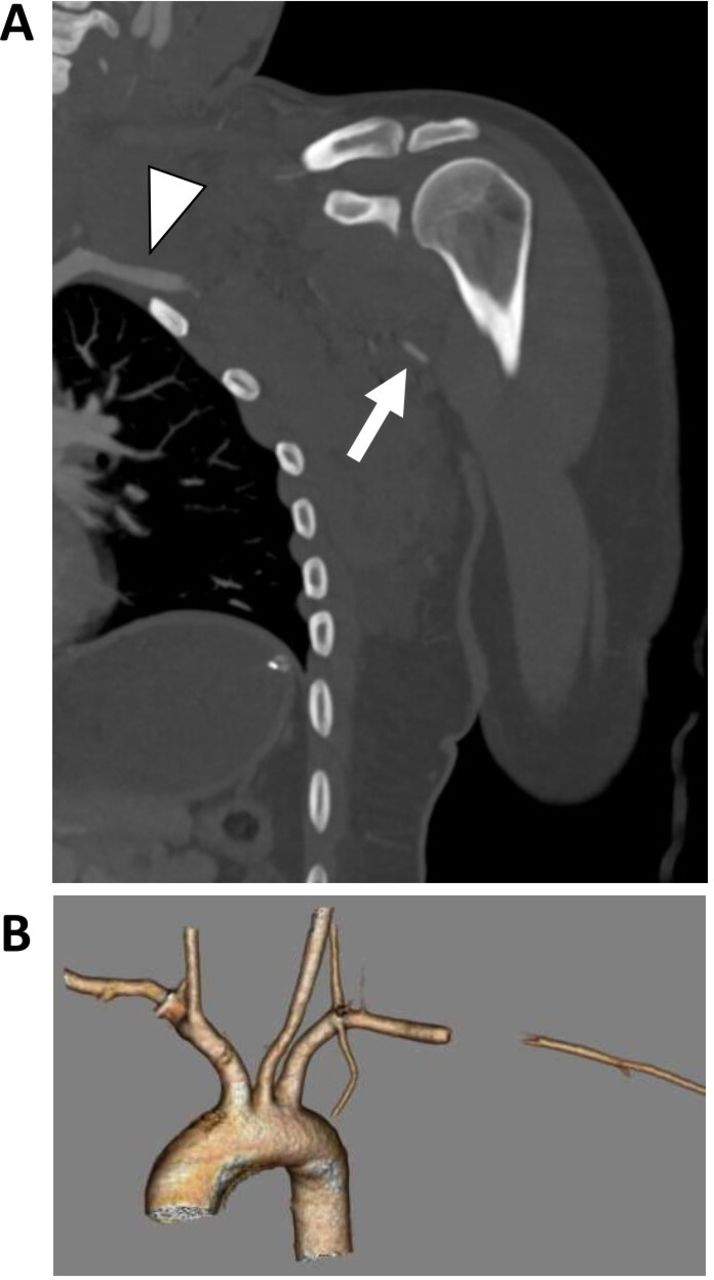
(A) CT arteriogram showing transection of left subclavian artery (arrow head) with distal reconstitution of the axillary artery (arrow). (B) 3-dimensional reconstruction of CT arteriogram.
The bullet that entered the upper back to the right of the midline fractured the medial right scapula, while there was no vascular nor bony injury related to the missile in the left thigh.
Question
Which approach would you use for an open repair of the left subclavian artery?
Median sternotomy with left supraclavicular extension
Left posterolateral thoracotomy
Left supraclavicular incision
Left infraclavicular incision
Management
The trauma-vascular team was consulted and took the patient to a hybrid operating room for an endovascular repair with a fallback plan of performing a left supraclavicular incision with division of the clavicle and repairing the artery with an interposition graft. The patient’s neck, chest, left upper extremity, and bilateral groins and upper legs were prepared and draped. Ultrasound-guided access with a micropuncture needle was obtained in the left common femoral artery. A Glide Advantage wire (Terumo Medical Corporation, Somerset, NJ, USA) was inserted into the descending aorta and the puncture site was upsized to an 8-Fr 90 cm length sheath. Using a wire and catheter, the sheath was advanced into the proximal left subclavian artery. An arteriogram was obtained, which demonstrated, once again, transection of the left subclavian artery with extravasation approximately 3 cm from the origins of the left vertebral and left internal mammary arteries (IMAs) (figure 2).
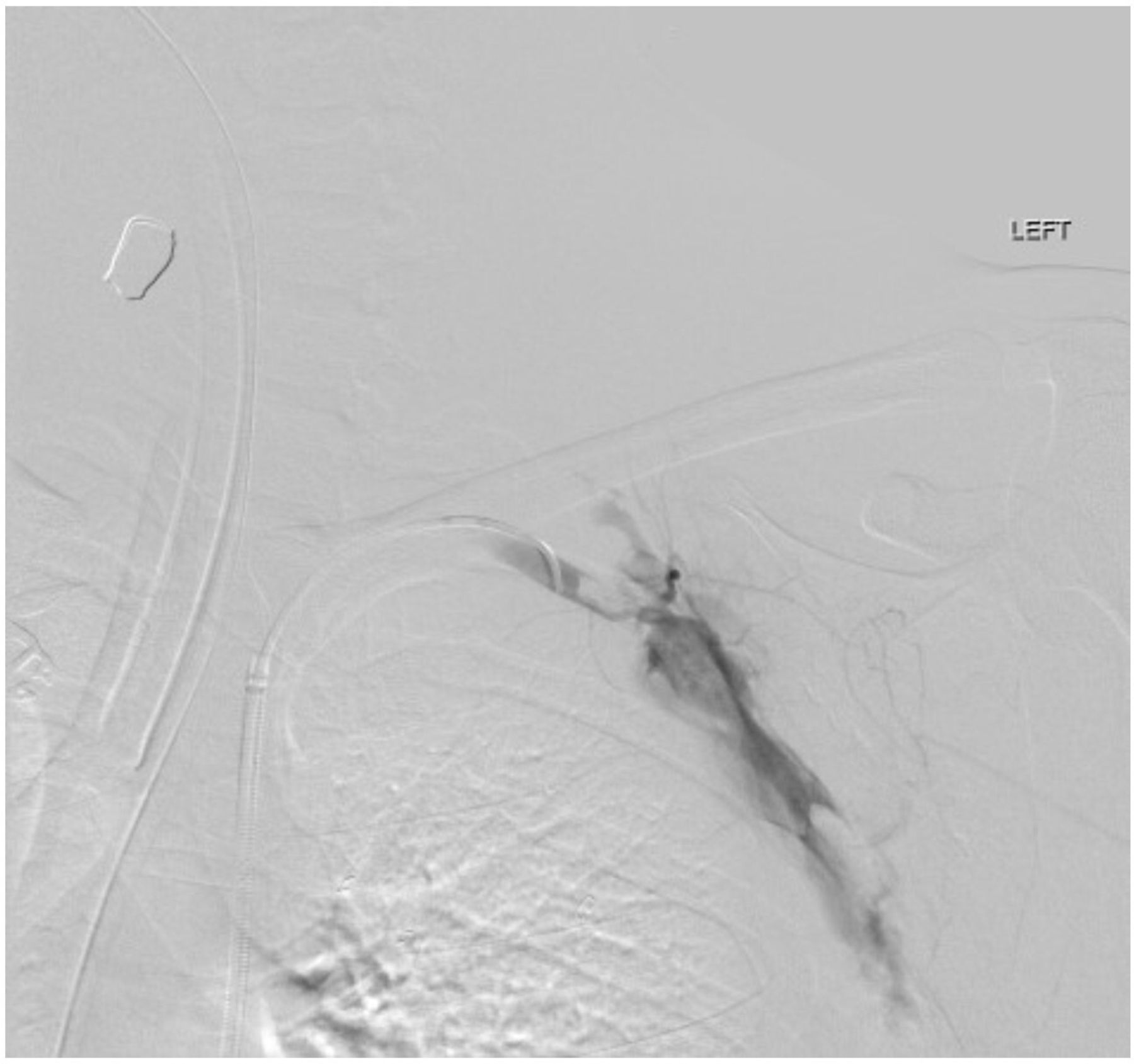
Intraoperative arteriogram showing transection of the left subclavian artery with extravasation.
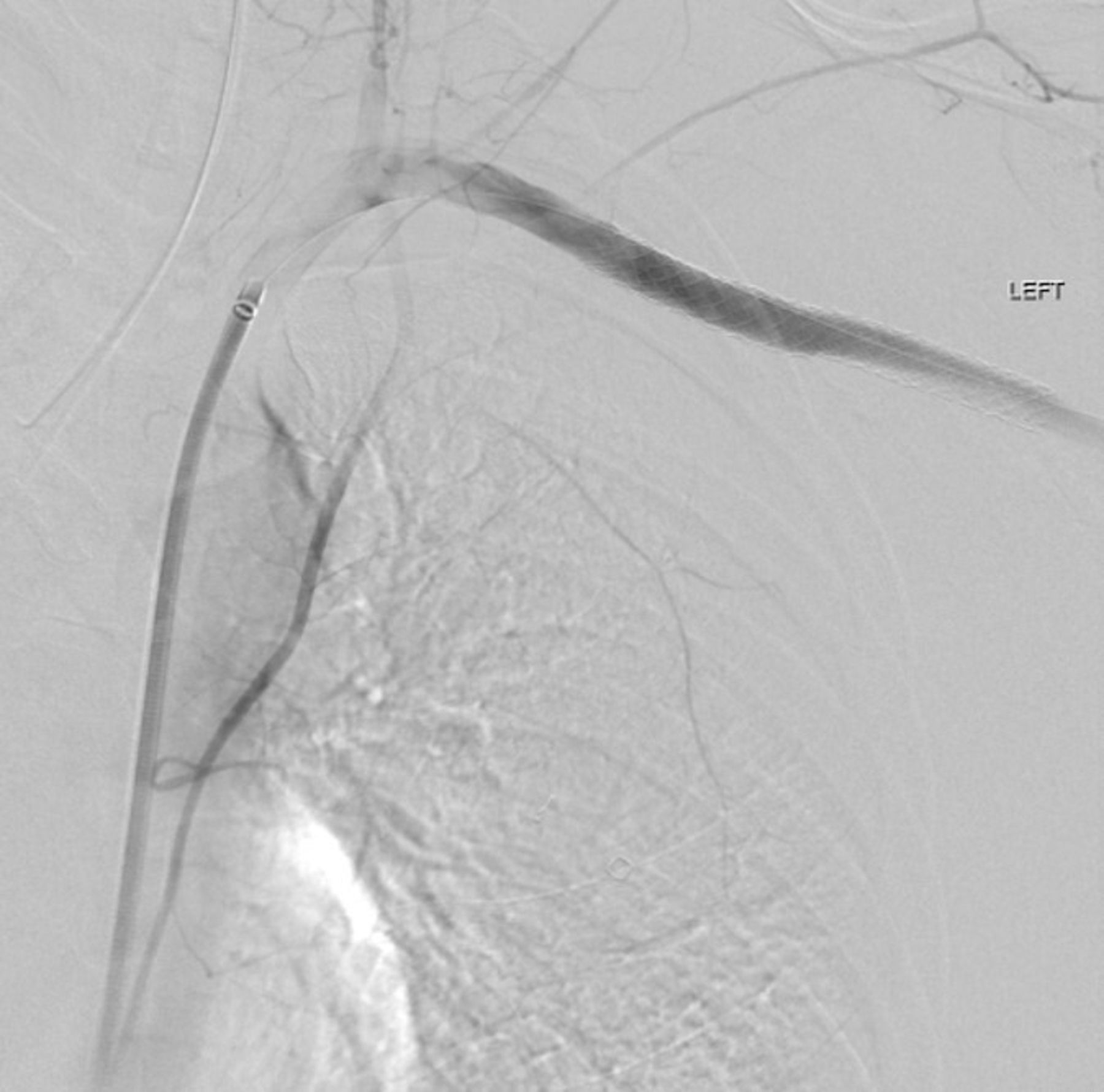
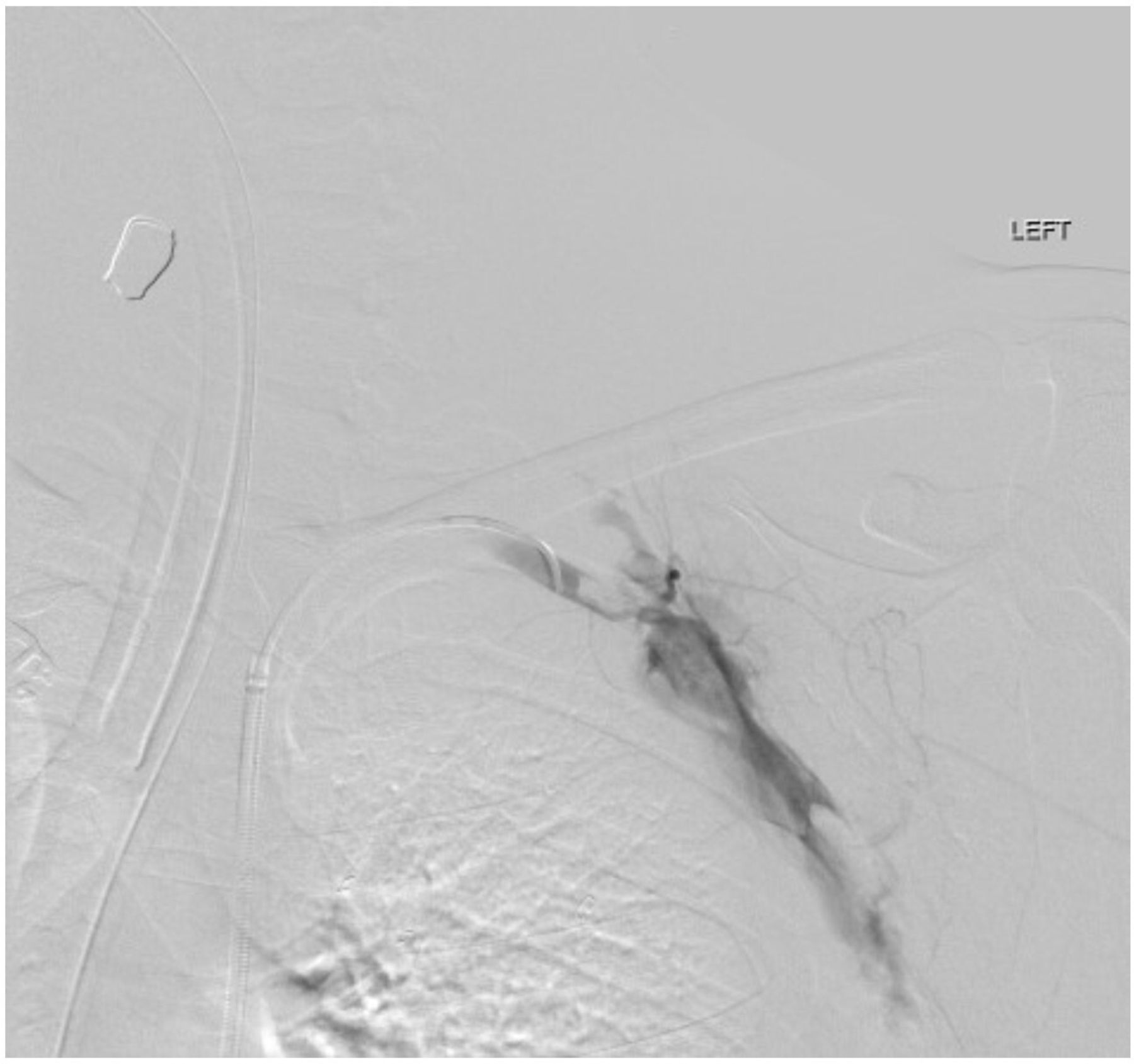
Attempts were made to cross the area of transection antegrade into the left axillary artery with multiple wire and catheter combinations without success. Thus, it was decided to perform a modified version of Gilani’s approach to subclavian-axillary artery injury.1 Ultrasound-guided retrograde access to the left radial artery was obtained, and a 5-Fr sheath was placed. A .018 wire was placed into the radial sheath and passed in a retrograde fashion across the left axillary artery and subsequently snared from the left subclavian artery such that through-and-through access between the two ends of the transected artery was established (figure 3). Next, the femoral sheath was advanced over the .018 wire to the proximal left brachial artery. An arteriogram confirmed intraluminal sheath access in the axillary artery indicating successful crossing of the injury (figure 4). An 8 mm × 79 mm GORE Viabahn VBX Balloon Expandable Endoprosthetic stent-graft (W. L. Gore & Associates, Flagstaff, AZ, USA) was positioned to cover the injury with approximately 20 mm of normal artery sealed on both ends. Completion left subclavian and left upper extremity arteriograms demonstrated inline flow down to the hand with no further contrast extravasation (figure 5). The left radial sheath was connected to a transducer that demonstrated pulsatile flow and then was left in place to be used as an arterial line for blood pressure monitoring. A biphasic Doppler signal of the left palmar arch was audible at the end of the procedure. The left common femoral artery access was then closed with a Perclose ProGlide device (Abbott Vascular Devices, Redwood City, CA, USA). The estimated blood loss was 50 mL.

.018 wire placed retrograde through left radial artery through the axillary artery into the left subclavian artery (arrow head). The snare was deployed through the left subclavian artery sheath (arrow). The radial artery wire was snared and pulled through the subclavian artery sheath.

Sheath traversing transection of left subclavian artery with arteriogram demonstrating intraluminal access to the proximal brachial artery from the femoral access.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Completion left subclavian arteriogram showing inline flow to the axillary artery with no contrast extravasation.
Given the transmediastinal trajectory of one of the bullets and concern for an injury to the esophagus or trachea, an upper gastrointestinal endoscopy, bronchoscopy, and laryngoscopy were performed and were normal.
Postoperatively, the patient was started on 81 mg of aspirin daily to maintain patency of the stent-graft. She had significant neuropathic pain which prompted the administration of 150 mg pregabalin three times a day. On postoperative day 2, she had increased left upper extremity edema and pain. A duplex ultrasound showed an acute thrombosis of the left axillary and brachial veins which was treated with 3 months of therapeutic anticoagulation. The patient was discharged from the hospital on postoperative day 4. On postoperative day 14, a duplex ultrasound of the stent-graft showed that it was patent with no evidence of stenosis; however, the distal left radial artery was occluded with some recanalization.
Discussion
Injuries to the subclavian and axillary arteries account for 5% to 10% of vascular injuries in civilian trauma centers, mostly from penetrating trauma.2 3 The subclavian artery is located in the transition zone between the thorax, neck, and upper extremity, and, as such, it is protected by the thoracic outlet comprised of the clavicle, first rib, subclavius muscle, deep cervical fascia, costocoracoid ligament, and clavi-coraco-axillary fascia. Because of this protection, stab injuries do not lead to injury as commonly as gunshot wounds.1 2 The most common associated injuries include those to the subclavian vein, vertebral artery, carotid artery, brachial plexus, aerodigestive tract in the neck, lung, spinal cord, and sympathetic nerve chain.2 3 In the modern era, deaths are usually due to associated injuries.4
Open approach
Prior to the endovascular era, open surgical exploration and repair was the standard approach for subclavian artery injuries. Because the subclavian artery is so well protected, it is challenging to gain access to the artery in an open operation, occasionally requiring multiple incisions. In one older but large review of 61 injuries to the subclavian artery and 50 injuries to the subclavian vein, 11 deaths (11.8%) occurred after open repair or ligation. If the seven patients requiring an emergency center thoracotomy are excluded, actual operative mortality was only 4.7%.5
The incision that best gives access to the first portion (intrathoracic) of the left subclavian artery is a high left anterolateral thoracotomy, while access to the first portion of the right subclavian artery is through a sternotomy, sometimes requiring a right supraclavicular extension. To approach the second portion of the left or right subclavian artery posterior to the scalenus anticus muscle, a supraclavicular incision is best with inclusion of a mid-claviculotomy or resection of the middle one third of the clavicle.
To approach the junction of the first and second portions of the left subclavian artery at the medial border of the left scalenus anticus muscle, a “trap door” or “book” thoracotomy—a high left anterolateral thoracotomy in addition to a left supraclavicular incision and a connecting partial upper median sternotomy—may be needed. Exposure of the junction of the first and second portions of the right subclavian artery is obtained with a median sternotomy and an extension of the incision to include a right supraclavicular incision as noted previously.
Finally, to gain access to the third portion of either subclavian artery beyond the scalenus anticus muscle, a supraclavicular incision with possible extension to an infraclavicular incision with division of the clavicle is used.4 6
Endovascular approach
The endovascular approach to repair of the subclavian artery in hemodynamically stable patients was first described in the literature in the 1990s.7–9 It has emerged as a safe and efficacious method of managing subclavian injuries as it eliminates the need for using complex incisions, the need for dissection in a bleeding and often distorted field, and risk of injury to important surrounding structures. In addition, endovascular balloon occlusion can provide proximal and distal control of hemorrhage in a rapid fashion. To use the endovascular approach requires trauma surgeons with vascular training or the availability of a vascular surgeon. While it is ideal to use a hybrid endovascular-surgical operating room, all that is needed in a regular operating room are a C-arm, C-arm compatible bed, and the appropriate endovascular equipment.
Other benefits of using the endovascular approach include less blood loss (most patients chosen for this approach do not have external or intrapleural bleeding) and less operative time.3 Success rates with endovascular repair have exceeded 95% with few intraoperative failures due to problems with stent deployment, inability to pass the guidewire beyond the lesion, or inability to cover the lesion. In a small retrospective study comparing endovascular versus open repair of subclavian or axillary artery injuries, endovascular repair was associated with lower in-hospital mortality and surgical site infections with a trend toward lower rates of sepsis, as expected.10
A drawback of the endovascular approach is the lack of in-hospital trained surgeons when patients with active bleeding present in the emergency room. Another is that the injured vessel and the surrounding damaged structures cannot be visualized.2 Postoperative complications include stent thrombosis and migration, endoleaks, access site injuries, and embolic events. Overall, because subclavian artery injuries are so uncommon, there is a paucity of data on the long-term outcomes of endovascular repair.6
Most commonly, endovascular techniques related to subclavian artery injuries are used for the treatment of traumatic false aneurysms, flow-limiting dissections, or focal occlusions. In the recent era, complete transection and thrombosis, formerly considered to be contraindications to endovascular therapy, can now be managed with endovascular repair.1 11 12 As noted earlier, hypotension and hemodynamic instability were also previously considered contraindications to endovascular therapy, but this restriction is also being overcome in institutions with in-house surgeons capable of rapidly passing a proximal occluding balloon.11 Of course, this does not apply to patients who present in extremis and require resuscitative thoracotomy and standard vascular control.6
The landing zone for an endovascular stent or stent-graft requires at least 1 cm of normal artery on the proximal and distal sides of the injury.13 Thus, an endovascular approach to repair may be limited by the proximity of the injury to the origins of either the vertebral artery in patients who have cerebrovascular disease or the IMA in patients who are status post-coronary artery bypass grafting with this vessel.
After stent placement, patients are generally placed on antithrombotic therapy using aspirin, clopidogrel, and/or anticoagulants. The need for early antithrombotic therapy may pose a threat to injured patients who have continued bleeding from other injuries. The data for use of antithrombotic therapy are derived largely from studies of patients with peripheral vascular disease who have undergone endovascular stenting.14 15 Therefore, further studies are necessary to clarify the need and duration of antithrombotic therapy in injured patients who have undergone endovascular stent-grafting procedures.
Conclusion
Endovascular repair of traumatic subclavian artery injuries has many benefits over the traditional open approach in properly selected patients. Despite this, a Western Trauma Association multi-center study in 2017 showed that use of endovascular approaches did not increase and was only used in a relatively small number of patients over a 10-year period.11 With such potential for improved patient outcomes, this calls for increased use of endovascular approaches by trained surgeons.
References
Footnotes
Editor's note All data relevant to the study are included in the article.
Twitter @JinadasaS
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.