Article Text

Abstract
Background Acute kidney injury (AKI) is common after severe trauma. AKI incidence and AKI stage have previously been shown to be associated with poor outcomes after trauma. However, AKI duration may also be important for outcomes after trauma, given that it is associated with long-term morbidity and mortality in general intensive care unit (ICU) and hospitalized patients. We hypothesized that duration of AKI is independently associated with poor outcomes after trauma.
Methods A cohort study was conducted at a single, level 1 trauma center. Patients admitted to the ICU between 2009 and 2018 were included. Data were extracted from the trauma registry and electronic medical records. AKI within 7 days from presentation was defined according to the Kidney Disease Improving Global Outcomes guidelines. Multivariable analyses were performed to assess the association between AKI incidence, AKI stage, and AKI duration with outcomes including prolonged ICU and hospital length of stay, discharge to home, and mortality.
Results Of 7049 patients included, 72% were male, the median age was 41 years (IQR 27–58), and 10% died. The AKI incidence was 45%, with 69% of these patients presenting with AKI on arrival. The majority (73%) of patients who suffered AKI recovered within 2 days. After adjustment in separate models, AKI incidence, AKI stage and AKI duration were each associated with prolonged hospitalization, an unfavorable discharge disposition, and mortality. AKI stage and duration were not used in the same model due to collinearity.
Conclusions Post-traumatic AKI was common on arrival and frequently short lasting. Duration correlated with highest AKI stage, and both were separately associated with prolonged hospitalization, discharge destination other than home, and mortality on adjusted analyses. Given the high incidence of AKI on arrival, stage or duration may be better targets for future interventions and quality improvement initiatives to improve outcomes after post-traumatic AKI.
Level of evidence III. Prognostic.
- acute kidney injury
- multiple trauma
- critical illness
- critical care
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Acute kidney injury (AKI) occurs in up to half of critically injured patients and is one of the most common manifestations of organ failure after severe trauma.1 2 Post-traumatic AKI is associated with prolonged length of stay, discharge to a destination other than home, and increased mortality.1 3–8 Despite the known consequences of AKI, little progress has been made in the treatment and prevention of AKI after trauma. Interventions that would be expected to have a positive impact on AKI have not demonstrated the predicted effects. For example, damage control resuscitation strategies that have been shown to improve the clinical course of trauma patients have repeatedly failed to show improvement in traditional AKI metrics such as incidence and need for renal replacement therapy.9–11 One reason may be that reporting of AKI incidence has been plagued by changing definitions and lack of standardization of reference creatinine estimates for diagnoses. Another reason may be that there is a spectrum of severity of AKI that is not captured by these traditional metrics. AKI stage and duration are more granular metrics than incidence that may be more useful for testing interventions to improve outcomes.12 Stage of AKI has previously been shown to be associated with poor outcomes after severe trauma.2 However, the prognostic significance of AKI duration has not been evaluated after trauma.
Given the impact of post-traumatic AKI on patient outcomes and resource utilization, quality improvement efforts have focused on AKI prevention including bundles that incorporate judicious fluid management and avoidance of nephrotoxins.13 14 However, the success of these initiatives is predicated on the goal of preventing post-traumatic AKI. Given that many patients arrive with AKI at admission, rapid treatment to shorten the duration and severity of AKI may be a worthy alternative goal of quality improvement efforts.15 It has been previously proposed that physicians should be using AKI duration to measure the effectiveness of an intervention instead of the binary outcome of AKI incidence.16 However, in patients who have suffered severe trauma, the most important metric to capture the burden of AKI remains unknown. In addition to the previously established relationship between AKI incidence and stage with poor outcome, we hypothesized that AKI duration is independently associated with mortality, discharge destination other than home, and prolonged hospitalization.
Methods
A retrospective cohort study was conducted at the Red Duke Trauma Institute at Memorial Hermann Hospital, Texas Medical Center, a high-volume, level 1 trauma center in Houston, Texas, USA. Adult (≥16 years) trauma patients requiring intensive care unit (ICU) admission during a 10-year period from January 2009 to October 2018 were included. Patients with pre-existing end-stage renal disease (ESRD), admitted to the burns service, directly transferred to the ICU, or without a creatinine measurement on arrival were excluded. The primary reasons for missing creatinine was due to primary use of point-of-care creatinine measurement and outside hospital creatinine measurements which were not integrated into the electronic medical records. Demographic characteristics, injury details, and outcomes were obtained from the institution’s prospectively maintained trauma registry. Laboratory results were extracted from the medical record. Discharge destination of home was defined as those who were discharged to a location requiring no advanced care including home, a psychiatric facility, or to jail. The Strengthening the Reporting of Observational Studies in Epidemiology guidelines for observational studies were followed.17
Outcome measures
AKI diagnosis was made based on the current creatinine-based guidelines published by the Kidney Disease Improving Global Outcomes (KDIGO) group.2 18 Since the baseline kidney function is unknown for most trauma patients, the Modified Diet of Renal Diseases (MDRD) was used to estimate reference creatinine for each patient. Use of the MDRD resulted in AKI diagnoses that were more informative than other reference estimates in prior works.2 The MDRD uses race, age, and sex3 19 20 and is calibrated to an assumed creatinine clearance of 75 mL/min.2 21 AKI incidence was defined as the proportion of patients who met AKI criteria at any point in the first 7 days to total included patients. This study was limited to the first 7 days to focus on AKI related to the traumatic injury. Highest AKI stage was defined as the stage met by the highest creatinine during the 7 days after admission, following the KDIGO guidelines. Stage 1 was assigned if there was an increase in serum creatinine by ≥0.3 mg/dL within 48 hours or an increase in serum creatinine to ≥1.5 times reference within 7 days. Stage 2 was assigned if there was an increase in serum creatinine by ≥2 times reference and stage 3 if there was an increase in serum creatinine by ≥3 times reference or was over 4.0 mg/dL. Patients without a creatinine measurement on a given hospital day were assigned the creatinine from the previous day.
Hospital-free days were defined by subtracting the length of stay from 30 days. Patients with a length of stay greater than 30 days and in-hospital deaths were assigned zero hospital-free day. Prolonged hospitalization was defined as below the 25th percentile of hospital-free days. Short-duration AKI was defined as ≤2 days and long-duration AKI was defined as >2 days to remain consistent with prior studies.22
Statistical analysis
The cohort was split into three groups for univariate analysis: no AKI, short-duration AKI (≤2 days), and long-duration AKI (>2 days). Demographics and outcomes with continuous variables were presented as medians and IQRs. Χ2, Wilcoxon rank-sum, and Kruskal-Wallis tests were used to compare categorical and continuous demographic data and outcomes, respectively. The calculated probability (p value) comparing the data observed in all three groups was listed in table 1. Multivariable Poisson regression with robust error variance was used to assess the relationship between AKI and in-hospital mortality for each of the reference estimates due to non-convergence of log-binomial models.23 24 All associations were reported as incidence rate ratios with robust CIs. Age, sex, arrival systolic blood pressure, and Injury Severity Score (ISS) were chosen a priori as covariables due to known or suspected association of these variables with AKI development and poor outcome. These three covariables were used along with each AKI metric to build models for the three outcomes of interest. Models were limited to survivors in prediction of prolonged ICU stay or hospitalization to account for death as a competing outcome. Additionally, AKI duration was offset for first week hospital days in the assessment of the relationship between AKI duration and mortality.25 AKI duration was assessed as both a continuous covariable and as a binary covariable (short or long). Patients with missing data were excluded from the multivariable analyses. Collinearity was assessed using computation of a variance inflation factor. All data analyses were completed using R V.3.53 (R Core Team. 2013. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria).
Characteristics of study participants
Results
During the study period, 8106 patients were admitted to the ICU after traumatic injury. Patients were excluded for ESRD (n=23), direct to ICU transfer (n=223), primary burn injury (n=25), and no creatinine drawn within 24 hours of arrival (n=786), leaving 7049 patients in the final analysis. After exclusions, less than 1% of data were missing. The median age was 41 (IQR 26–58) years. Male sex was predominant, accounting for 72% of the cohort. Participants were severely injured with a median ISS of 20 (IQR 13–29) (table 1). Patients with AKI, either long or short duration, were older and presented with higher arrival creatinine than patients without AKI. Additionally, they presented with lower hemoglobin and lower base excess values than patients without AKI. Patients with long-duration AKI had similar characteristics as those with short-duration AKI, except patients with long-duration AKI were older.
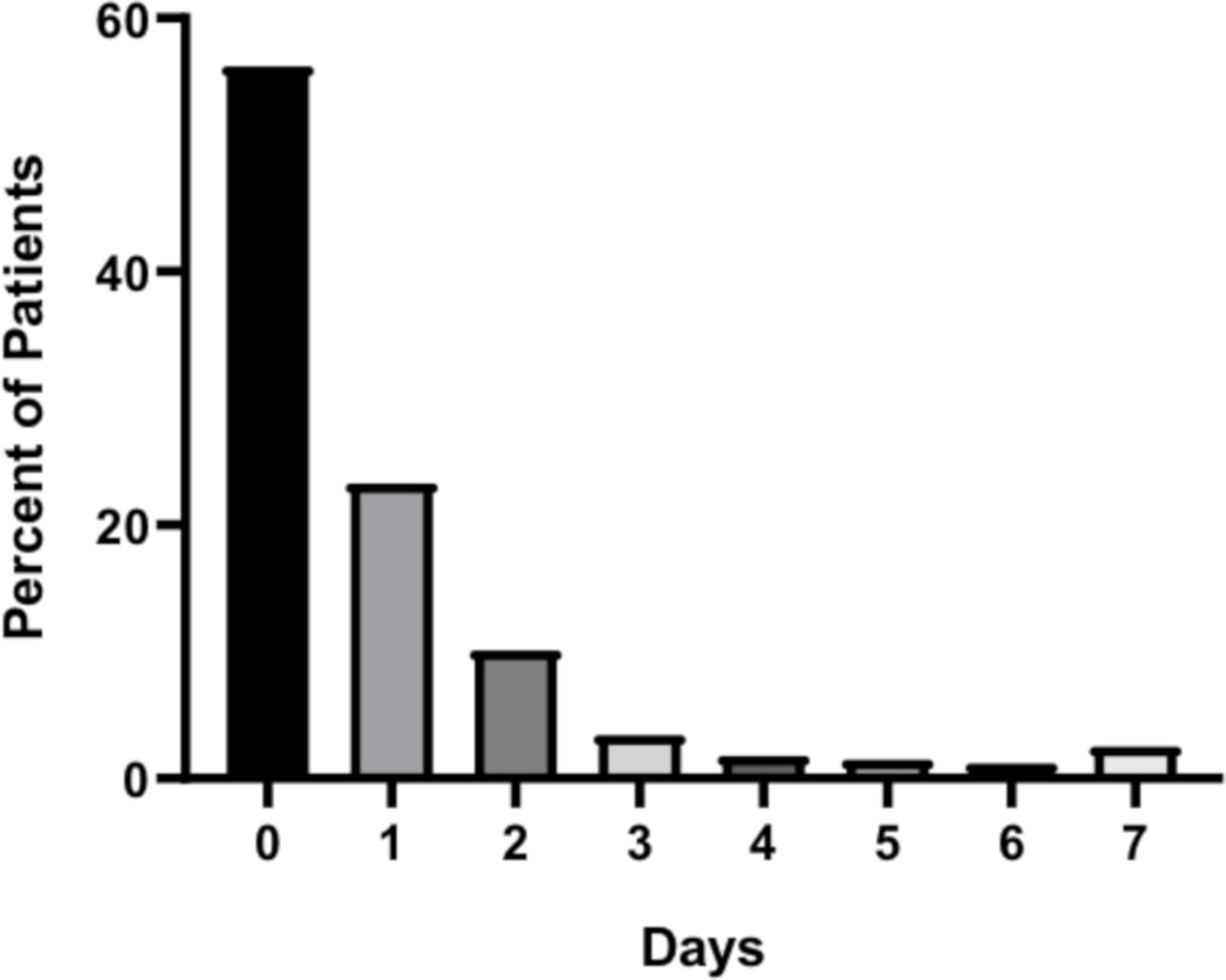
A total of 3153 (45%) patients suffered AKI during the first 7 days after arrival. Sixty-nine percent of these patients (31% of all patients) had AKI on arrival. The majority of patients with AKI suffered stage 1 (67%). The duration of AKI spanned from 0 to 7 days, with the majority of patients suffering either no AKI days or a short duration of AKI (figure 1). Among patients with AKI, the median duration was 1 day (IQR 1–1). Short-duration AKI was most common in this cohort, with 2303 patients (73%) recovering from AKI within 2 days of onset.
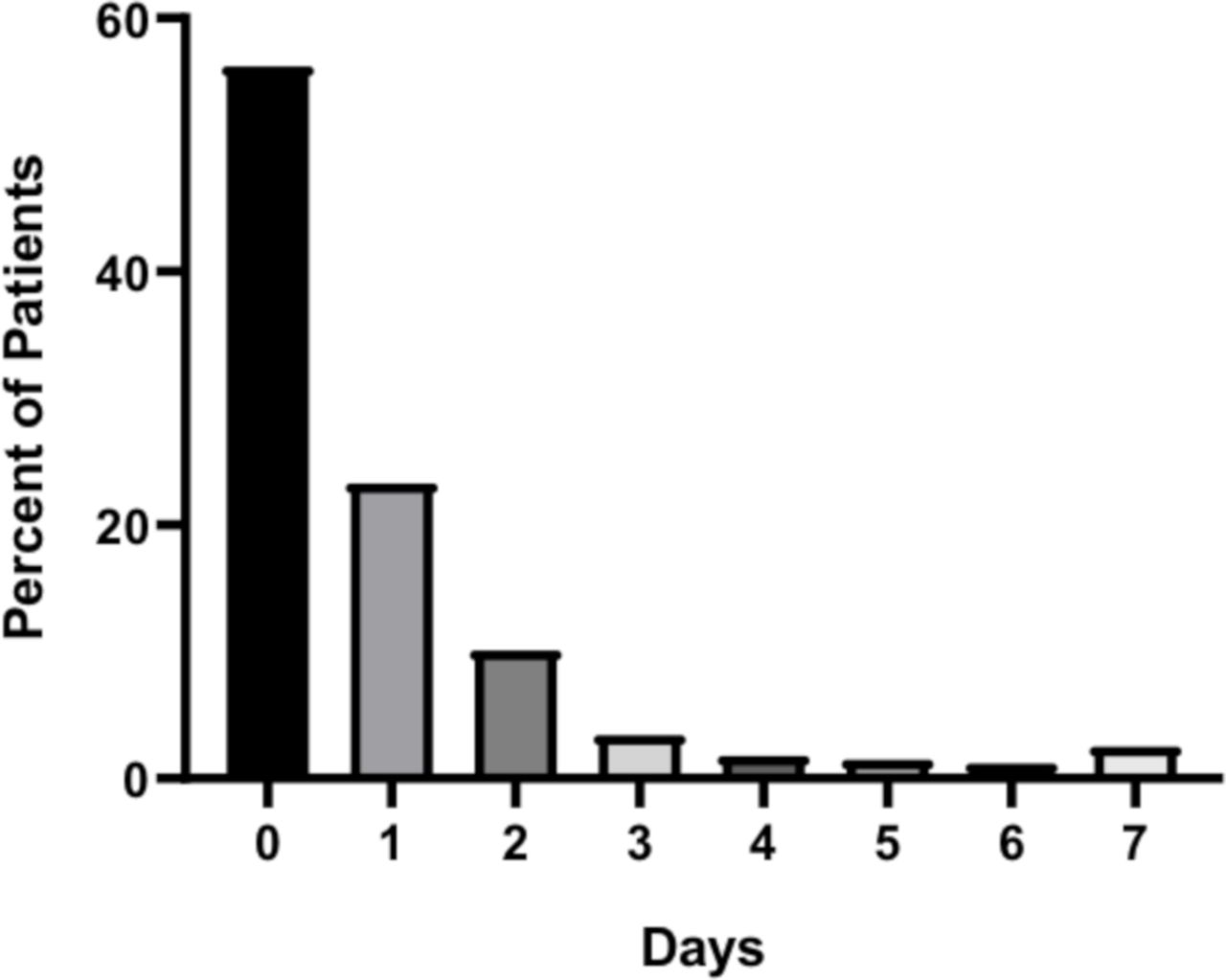
Duration of acute kidney injury (AKI), raw data.
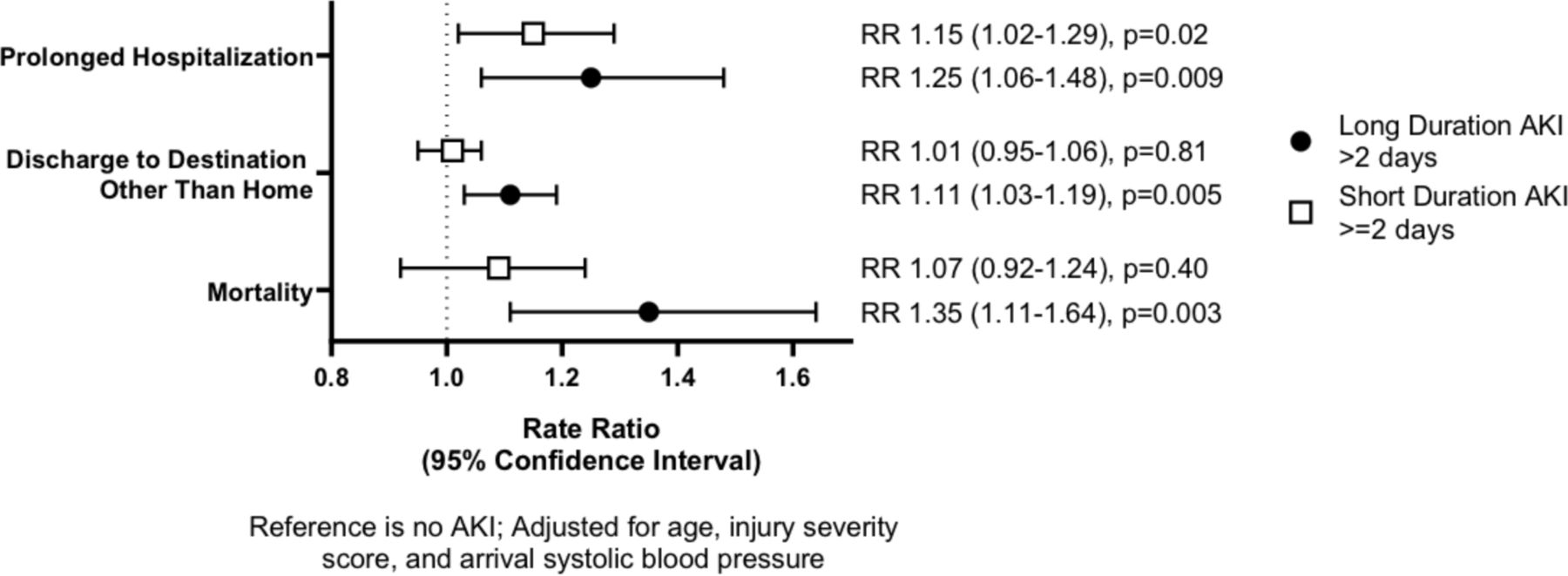
On multivariable analysis, incidence of AKI was associated with prolonged hospitalization, discharge destination other than home, and mortality (table 2). Incremental increases in AKI stage and AKI duration (per day) were also associated with prolonged hospitalization, discharge destination other than home, and mortality (table 2). Both long (>2 days) and short durations of AKI were positively associated with prolonged hospitalization, discharge destination other than home, and mortality (figure 2). There was a larger and more precise effect of long duration of AKI on poor outcomes than short duration. AKI stage and duration were collinear and were therefore not assessed against each other in one model.

{kind=link}
{kind=link}
Acute kidney injury (AKI) duration and outcomes.
Association between AKI metrics and outcomes on multivariable analyses
Discussion
AKI was common during the first week of hospitalization after severe trauma, occurring in almost half of a large population of critically injured patients presenting to a busy urban trauma center. Consistent with prior reports, AKI incidence and stage were associated with prolonged hospitalization, discharge destination other than home, and increased mortality. Additionally, AKI duration was independently and incrementally associated with the same poor outcomes. Due to collinearity, the importance of stage and duration was not directly compared.
Although the relationship between duration and outcomes after trauma has not been previously described, duration of AKI has been noted to be associated with clinical outcomes in other patient populations including medical critical care, cardiac surgery, general hospitalization, and postmyocardial infarction.12 26 Authors have previously distinguished ‘short’ or ‘transient’ duration AKI of ≤2 days from longer durations of AKI. In non-trauma patients, both short-duration and long-duration of AKI have been found to be independently associated with poor long-term outcomes, with a greater magnitude of association with longer duration of AKI. Short-duration AKI was found to be independently associated with mortality, congestive heart failure, and myocardial infarction when compared with patients without AKI.12 27 Long-duration AKI was also associated with increased mortality, myocardial infarction, and development of chronic kidney disease (CKD).12 26 The present study confirms an association between AKI duration and subsequent outcomes in trauma patients.
In non-trauma patients, longer AKI duration was independently associated with poor outcomes after adjusting for stage.12 28 However, in this study of trauma patients, duration and stage were collinear, indicating that duration and stage were not independent. One reason for this difference may be that this study only evaluated relatively short-term outcomes, whereas studies in non-trauma populations measured longer term outcomes such as development of CKD, long-term mortality, or rare events in the generally young and previously healthy population such as congestive heart failure exacerbation and myocardial infarction.12 26 Another reason may be the difference in AKI etiology and time to reversal of the underlying pathophysiology. Over 50% of trauma ICU patients at the study center present with either shock or occult hypoperfusion due to hemorrhage.29 Hemostasis is achieved by a median of 120 minutes from hospital arrival if emergent hemorrhage control is required.30 In contrast, patients with AKI related to sepsis or cardiogenic shock more commonly found in the general ICU literature likely have prolonged renal insults. Finally, the duration that is considered ‘long’ and ‘short’ varies between the trauma literature and the general ICU literature. The impact of long duration on poor outcomes is greatest in patients with an AKI duration of 7 or more days.12 Duration of AKI longer than 7 days was rare in our population, and therefore the distinction between ‘long’ and ‘short’ was made at 2 days (figure 1). A larger multicenter study may determine if AKI in trauma patients is truly different from that in other critically ill patients.
Progress in development of effective therapeutic strategies for the prevention or treatment of AKI has been poor. Supportive care remains the cornerstone of AKI prevention and treatment, regardless of the underlying etiology. According to the KDIGO Clinical Practice Guideline, AKI prevention efforts should include decreasing nephrotoxic exposure, ensuring adequate volume status and perfusion, close monitoring of serum creatinine and urine output, and avoiding hyperglycemia.18 Once AKI has already developed, efforts to mitigate the impact of AKI are limited to avoidance of exacerbating factors and supportive care such as renal replacement therapy. Specific risk factors for post-traumatic AKI include rhabdomyolysis, massive hemorrhage and resuscitation, systemic inflammatory response to trauma, and direct kidney trauma.31 High-quality evidence is lacking regarding the treatment of these underlying conditions to optimize renal recovery.
AKI metrics are used in clinical trials to evaluate the effectiveness of strategies to mitigate or prevent AKI, and to benchmark performance across centers. In trauma, the Trauma Quality Improvement Project (TQIP) provides risk-adjusted outcome metrics to centers for quality improvement purposes. Currently, TQIP only assigns a diagnosis of AKI to those patients who meet criteria for KDIGO AKI stage III. While progression to AKI stage III and need for renal replacement therapy are important outcomes, they only represent a minority of trauma patients with AKI.2 5 6 Thus, interventions to reduce AKI, using this definition, will only potentially benefit a small number of patients. Additionally, this study demonstrated that one-third of severely injured patients admitted to the ICU present with AKI at admission. Thus, incidence of AKI may be just as much a measure of injury severity and prehospital care than trauma center care. Our study suggests that highest stage or duration of AKI would be more granular, clinically relevant metrics to collect than AKI incidence. Additionally, tracking AKI present on arrival would also better inform quality improvement initiatives and clinical trials.
Limitations
Several limitations existed in this study. First, hourly urine output was not considered for AKI diagnosis and staging.4 6 7 There are significant limitations in the accuracy of urine output data retrospectively collected. The effect of this exclusion likely resulted in an underestimation of AKI incidence. Prospective studies of AKI after trauma should incorporate hourly urine output into AKI diagnostic criteria to optimize the value of the diagnosis. Furthermore, mortality and discharge are competing outcomes with AKI duration. A metric such as AKI-Free Days may be used in practice to adjust for these outcomes while evaluating the long-term prognosis of trauma patients who suffer AKI. Third, patients with CKD were not excluded from this study due to absence of accurate data regarding medical history, which is often incomplete among trauma patients requiring immediate ICU care. Furthermore, it is estimated that only 20% of patients with CKD are aware of their illness.32 It will be important to assess the burden of CKD on this patient population and its impact on duration of AKI in future studies. It is expected that patients with underlying CKD will be more prone to AKI and to prolonged AKI after traumatic injury. Finally, the traditional MDRD equation using race as a cofactor was used for estimation of baseline glomerular filtration rate (GFR) given its diagnostic superiority on prior studies.2 However, inclusion of race is problematic as it is not a biologic designation and, in some situations, may worsen disparities.33 Alternate methods of accurate GFR estimations are needed for this patient population.
Conclusions
The majority of patients suffered mild severity AKI for a short duration after hospital arrival for severe trauma. Prolonged AKI duration was independently and incrementally associated with worsened outcomes including prolonged hospitalization, discharge destination other than home, and mortality. Additionally, increased AKI stage was associated with poor outcomes. Either or both should be considered additional metrics to incidence in informing quality improvement efforts as well as in benchmarking trauma center quality.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Ethics approval
This study was approved by the Institutional Review Board of the McGovern Medical School at UTHealth under number HSC-GEN-13-0325 and a waiver of individual informed consent was granted due to the retrospective nature of the study.
Acknowledgments
The authors thank Dr Shuyan Wei, MD, MS, for her contribution to study conception and Dr Peter Killoran, MD, for his assistance with data acquisition.
References
Footnotes
Contributors GEH designed the study, obtained the data, analyzed the data, interpreted the findings, and wrote the article. JH, CEW, and LSK were major contributors to study design, findings interpretation, and article revisions. All authors read and approved the final article.
Funding CEW receives funding from the William Stamps Farish Fund, the Howell Family Foundation, the James H ‘Red’ Duke Professorship. GEH was supported by the National Institute of General Medical Sciences of the National Institutes of Health (5T32GM008792).
Disclaimer The role of the funding body was not involved in the design of the study, collection of data, analysis, interpretation of findings, or writing the article.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.