Article Text

Abstract
Background Overtriage of trauma patients is unavoidable and requires effective use of hospital resources. A ‘pit stop’ (PS) was added to our lowest tier trauma resource (TR) triage protocol where the patient stops in the trauma bay for immediate evaluation by the emergency department (ED) physician and trauma nursing. We hypothesized this would allow for faster diagnostic testing and disposition while decreasing cost.
Methods We performed a before/after retrospective comparison after PS implementation. Patients not meeting trauma activation (TA) criteria but requiring trauma center evaluation were assigned as a TR for an expedited PS evaluation. A board-certified ED physician and trauma/ED nurse performed an immediate assessment in the trauma bay followed by performance of diagnostic studies. Trauma surgeons were readily available in case of upgrade to TA. We compared patient demographics, Injury Severity Score, time to physician evaluation, time to CT scan, hospital length of stay, and in-hospital mortality. Comparisons were made using 95% CI for variance and SD and unpaired t-tests for two-tailed p values, with statistical difference, p<0.05.
Results There were 994 TAs and 474 TRs in the first 9 months after implementation. TR’s preanalysis versus postanalysis of the TR group shows similar mean door to physician evaluation times (6.9 vs. 8.6 minutes, p=0.1084). Mean door to CT time significantly decreased (67.7 vs. 50 minutes, p<0.001). 346 (73%) TR patients were discharged from ED; 2 (0.4%) were upgraded on arrival. When admitted, TR patients were older (61.4 vs. 47.2 years, p<0.0001) and more often involved in a same-level fall (59.5% vs. 20.1%, p<0.0001). Undertriage was calculated using the Cribari matrix at 3.2%.
Discussion PS implementation allowed for faster door to CT time for trauma patients not meeting activation criteria without mobilizing trauma team resources. This approach is safe, feasible, and simultaneously decreases hospital cost while improving allocation of trauma team resources.
Level of evidence Level II, economic/decision therapeutic/care management study.
- trauma triage
- field triage
- trauma activation
- resource
Data availability statement
No data are available. Data are not in a repository state. Data sets will not be shared due to institutional restrictions in data use agreement but aggregate deidentified data supporting the findings of this study are available from authors upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The creation of regionalized trauma centers has significantly decreased the morbidity and mortality of acutely injured patients by enabling a rapid resuscitation response.1–3 However, providing quality care while maintaining cost-effectiveness is labor intensive. It requires the continual development and assessment of various protocols and quality indicators to ensure the efficacy of care delivery.4 Effective triage protocols are the first part of an efficient trauma system. They must accurately reflect the needs of the injured patient to mobilize appropriate care resources. Overtriage results in unnecessary personnel and financial utilization whereas undertriage delays necessary care for the injured patient.5 6 To maximize field and in-hospital triage efficiency, physiological and anatomic criteria must be considered in conjunction with injury mechanisms, comorbidities, and age-related issues.7
Field triage guidelines were established in 1986 by the American College of Surgeons Committee on Trauma and most recently modified in 2011.8 Their purpose is to maintain the triage balance based on a 5% undertriage rate and 30% to 50% overtriage rate.9 However, such a high overtriage rate may not be sustainable nor desirable10 and decreasing overtriage will reduce cost.11 In the USA, treatment of traumatic injury is the second leading healthcare expenditure behind heart disease.12 Measures to reduce overtriage are complicated by the growing geriatric population with a higher prevalence of anticoagulant and antiplatelet usage. When combined with a reduced physiological reserve and increased comorbid conditions, these patients risk more adverse outcomes.13 14 While a full trauma team activation has been associated with shorter emergency department (ED) length of stay (LOS) and decreased in-hospital mortality in geriatric trauma patients, it is also cost intensive and places burdens on human and material resource utilization. It should only be used selectively and avoided altogether in less severely injured patients.10 15
Moreover, the San Diego County trauma system only designates level I and II trauma centers. There are no level III or lower centers with the resources committed to trauma care, and thus patients with significant injuries generally require secondary transfer to a trauma center. This creates a situation with potentially more overtriage than other inclusive trauma systems.
To decrease cost and resource utilization associated with overtriage, our trauma center previously devised a separate tier of triage designation named trauma resource (TR). Patients triaged to this tier were initially brought to an ED examination room rather than the trauma resuscitation bay. The full trauma team was not activated on arrival. Instead, the trauma nurse/ED nurse and ED physician performed the initial evaluation. Our initial study16 found that this designation decreased the utilization of resources without increasing LOS or in-hospital mortality. The TR patients also incurred an activation fee worth one-quarter of the trauma activation (TA) charge. Despite these benefits, we also observed increased duration from door to CT scans in this population. To further streamline the evaluation of these patients we modified our TR evaluation protocol by adding a rapid ‘Pit Stop’ (PS) evaluation. This rapid assessment would occur in the trauma resuscitation bay rather than go to an ED bed for their initial evaluation. This would allow for faster decision-making and transit to appropriate imaging studies. We hypothesized that we would further improve efficiency of care delivery without compromising safety.
Methods
All trauma patients evaluated at one American College of Surgeons (ACS)-certified level II trauma center from October 1, 2016 through June 30, 2017 were included in this study. Patients meeting ACS trauma and county criteria were designated TAs by prehospital and base station personnel (table 1).
Institutional major and minor trauma team activation and TR criteria
Patients not meeting criteria for trauma team activation but were thought to require trauma center evaluation were triaged as TRs. This designation was based on prehospital information given to the registered nurse (RN) at the hospital base station, and generally included ‘Special Considerations’ criteria (table 1). Base station RNs discussed equivocal triage decisions with the ED physician, and then designated a TA, a TR, or evaluation as a routine ED patient.
Pit stop
A ‘pit stop’ was created in the trauma bay where TR patients underwent expedited evaluation by a board-certified ED physician, dedicated Trauma Nursing Core Course (TNCC)-certified trauma nurse or TNCC-certified ED nurse. During the PS, if criteria were discovered which increased the trauma severity, the TR would be updated immediately to TA. The trauma surgeon was immediately available in case of an upgrade to a TA. Additionally, the CT technician, respiratory therapist and laboratory technician were notified on patient’s arrival to the ED. CT scans for TR patients were prioritized. A comparison of tiered resource utilization can be seen in table 2.
Resource utilization by level of trauma activation*
ED consultations
There are two categories of ED consultations: (1) routine ED (non-TR) patients who were found to have injuries that require further evaluation and inpatient care and (2) TR patients who require further evaluation and inpatient care. These two groups were separated for analysis given the differences in TRs used.
Data and statistics
Demographic and outcome data including age, LOS, mortality, time to physician evaluation, and time to CT scan were analyzed for the post-PS implementation period and compared with the pre-PS period. Analyses also included comparisons between the TA group versus TR group after PS. Injury Severity Score (ISS) was compared for applicable groups. The discharge disposition for the TR patients was also noted. Comparisons were made using 95% CI for variance and SD calculations, χ2 tests, two-proportion z-tests, analysis of variance and unpaired t-tests for two-tailed p values, with statistical difference, p<0.05.
The Cribari matrix was used to determine the overtriage and undertriage rates for TAs and TRs. Overtriage was defined as a major/full trauma team activation in patients with ISS ≤15. Undertriage was defined as patient with ISS >15 who did not receive a major/full trauma team activation. With regard to undertriage, minor/partial trauma team activation and TR activation were considered in the same manner. ED activation charges were used as a surrogate for cost. Information on hospital personnel activated and charges for each trauma triage level was derived from established hospital charge levels and noted in table 2.
Results
During the 9-month post-PS implementation study period a total of 1685 patients were received by our hospital requiring trauma center evaluation. Nine hundred and ninety-four patients were triaged to the TA group and 474 patients were triaged to the TR group (table 3).
Patient characteristics of TA vs. TR vs. non-TR consults after pit stop implementation
Two patients (0.4%) initially triaged to the TR group were immediately upgraded to TA status by the ED physician. Eighty-two patients (17%) required trauma consultation of which 76 (16%) were admitted to the trauma service (TS), 3 (0.6%) were admitted to a non-TS, 2 (0.4%) were discharged and one patient left against medical advice. The remaining 392 patients (83%) designated as TR underwent ED physician directed care without trauma team involvement. Forty-nine patients (10%) were admitted to a non-TS. Overall, 346 (73%) patients in the TR group were discharged from the ED (figure 1).
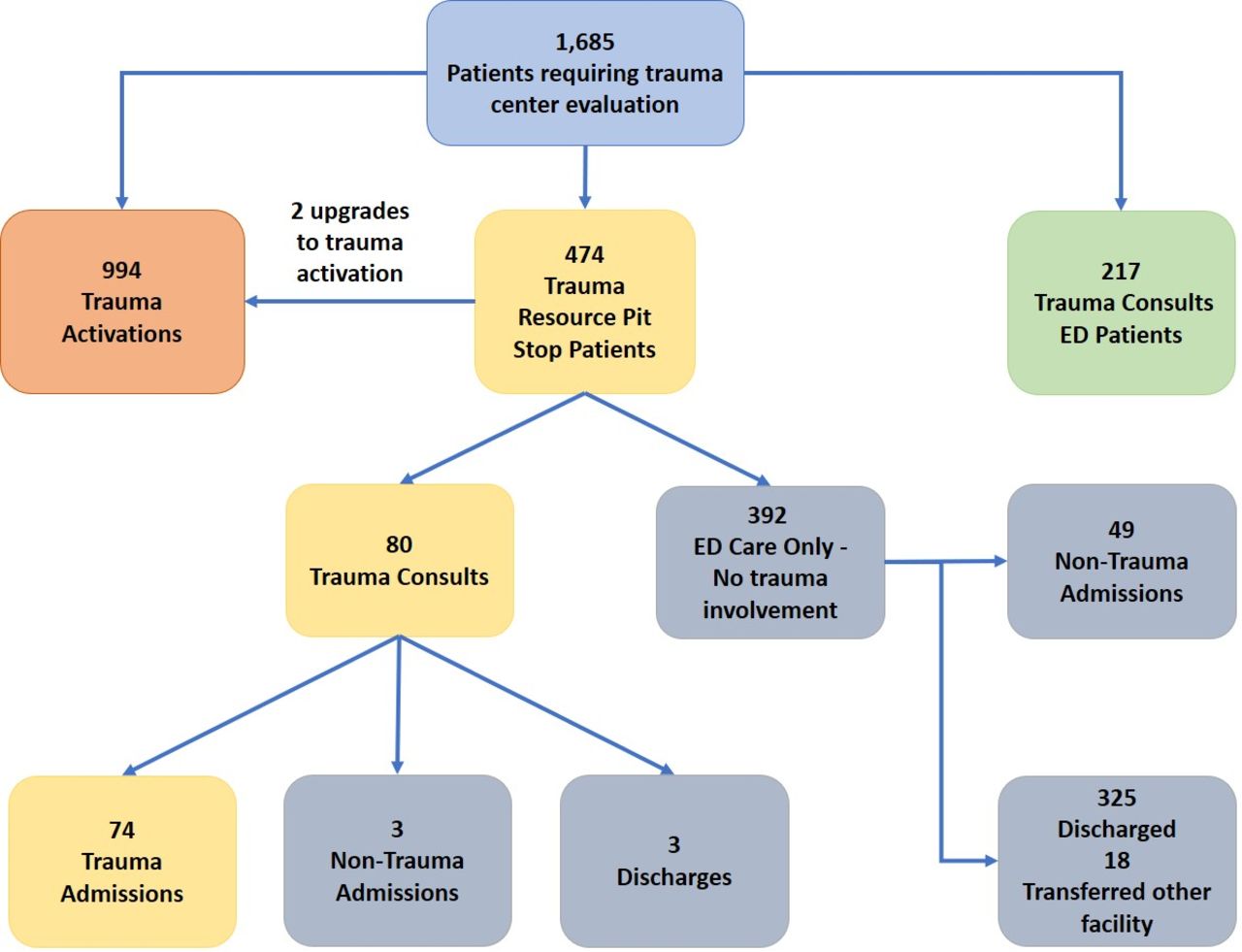
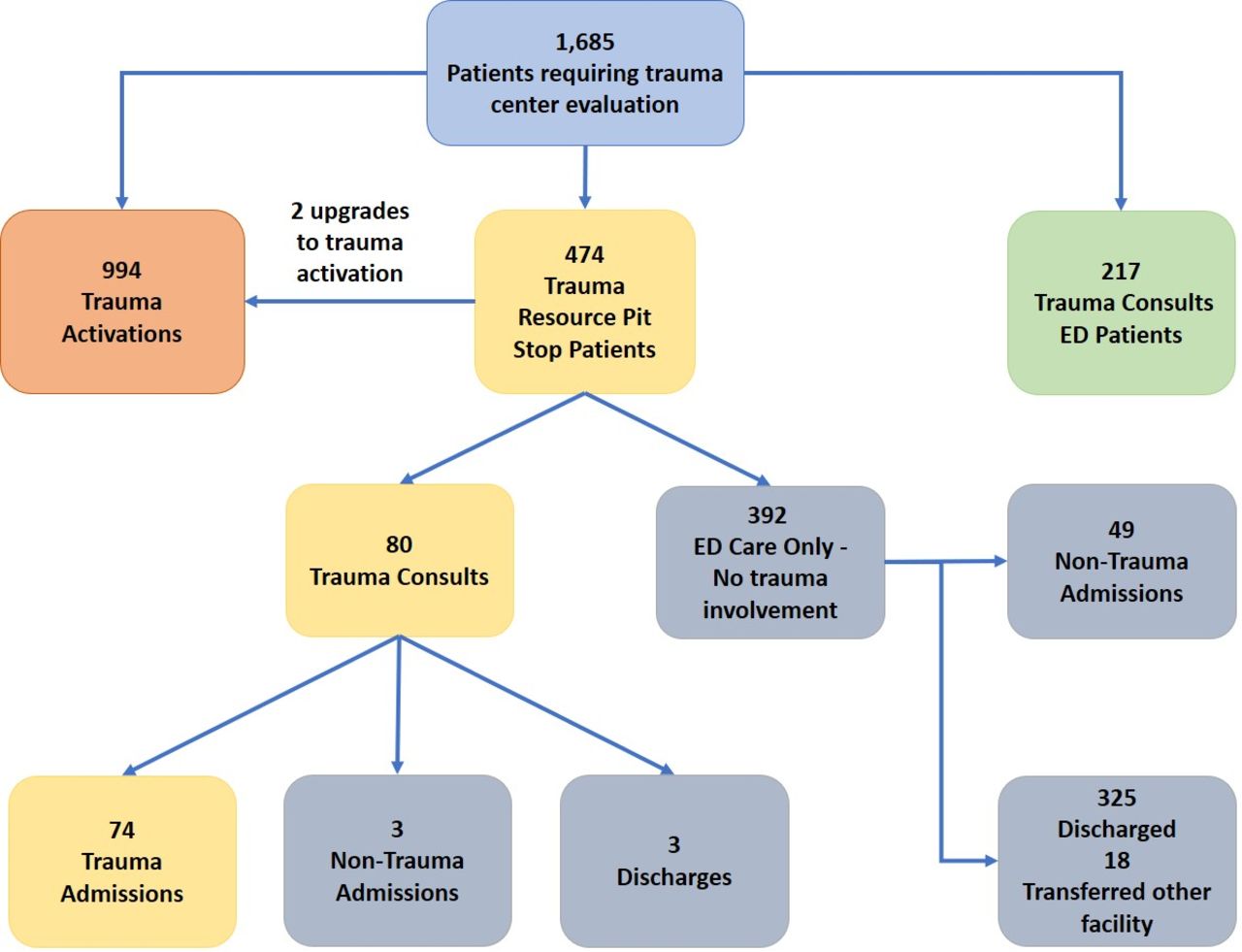{kind=link}
Patient flow during pit stop (PS) implementation. ED, emergency department.
When evaluating only patients admitted to the TS, TR patients (n=76) differed than TA patients (n=591) in that they were older (61.4 vs. 52.1 years, p<0.0001), had shorter LOS (4.7 vs. 7.6 days, p<0.0001) and more likely to fall as a mechanism of injury (60% vs. 32%, p<0.0001). TR patients also had increased door to physician evaluation times (8.3 vs. 0.2 minutes, p<0.0001) and increased door to CT times (48.3 vs. 27.4 minutes, p<0.0001). There was no difference evident between TR and TA for in-hospital mortality, but these groups were small in size for sound statistical comparisons.
The TR patients admitted to TS (n=76) were similar to admitted trauma consultations from the ED (n=213) in age, gender, fall mechanism, ISS, LOS and in-hospital mortality. TR patients upgraded to TA status by the ED physician had longer times to CT compared with patients initially triaged as a TA (table 3).
Analysis of before/after ‘pit stop’ implementation periods showed significant decreases in mean door to CT times (67.7 vs. 50 minutes, p<0.0001) for TR patients(table 4). Personnel and hospital charges were significantly less in the TR group compared with the TA group (table 2). There were four deaths in the TR group (4 of 74) admitted to TS.
TR patient characteristics before and after pit stop implementation
Based on Cribari matrix calculations, the overtriage rate was 81% for TR patients, and undertriage rate was 3.6%. The overtriage for the admitted TR patients using the Cribari matrix is expected since these were not TAs. The non-TR ED consults had an undertriage rate of 18%.
There was no difference in the mean ISS for TR patients admitted to the TS before and after PS intervention. (The ISS for admitted pre-PS TR patients was 9.7±5.3 and the ISS for admitted post-PS TR patients was 10.9±5.5 with a p value of 0.22.)
Discussion
We have shown that the TR triage designation provides for prompt evaluation of patients with potential injuries, and that incorporation of a PS in the patient flow has improved the efficiency of the process.
The San Diego County trauma system only designates level I and II trauma centers. There are no level III or lower centers with the resources committed to trauma care, and thus patients with significant injuries generally require secondary transfer to a trauma center. This creates a situation with potentially more overtriage than other inclusive trauma systems.
In the past 20 years, ED visits have increased over 50%, with 39 million injury-related ED visits in the USA in 2015.17 As such, it is increasingly important for patients to be conveyed to the appropriate facility.18 The key to effective triage depends on identifying patients with severe injuries who will benefit from the resources available at ACS-verified trauma centers.19 Overtriage (transporting patients with minor injuries to trauma centers) and undertriage (transporting seriously injured patients to non-trauma centers) can both create complications for the patient and burden healthcare system.18 While there are standardized criteria for TAs designated by the ACS and San Diego County, there are not standardized tiers to categorize the hospital resources responding to each TA. Our institution developed a multiple tiered TA scheme to deploy our resources more efficiently. By adding a TR category to our trauma triage system, we were able to significantly decrease cost and resource utilization associated with overtriage.
Only 17% of the patients designated as TR group required TS consultation and 16% required trauma admission. The TR patients used fewer personnel and hospital resources with no significant difference for in-hospital mortality. Prompt evaluation by a board-certified ED physician was key, with only two patients (0.4%) requiring immediate upgrade to TA status.
In our previous study of the TR patients, door to CT times were significantly longer in the TR group as compared with the TA group.16 By adding the PS evaluation, we were able to significantly decrease time from door to CT scan for the TR group from 67 to 50 minutes. The addition of the PS created a rapid evaluation and transport environment without the activation of the full trauma team resources, the most important of these aspects being:
Face-to-face hand-off between field emergency medical service and hospital providers.
Rapid primary and secondary survey evaluation.
Prearrival notification to radiology technicians.
The ability to transport directly to diagnostic testing prior to being placed in an ED room.
The PS was associated with a reduced time to CT scan. Our institution’s CT scanning triage protocol gives priority to TAs, stroke codes, and ED patients with acute neurologic deterioration. The TR patients upgraded to TA status demonstrated no change in time to CT when compared with TA patients.
Other ED patients including abdominal emergencies are generally triaged after TR patients. However, individual circumstances such as suspected ruptured abdominal aortic aneurysm will be discussed. Since the ED physician is generally ‘in charge’ of all these patients’ workups, and they determine relative prioritization.
Given that TR patients do not meet criteria for trauma team activation, it can be argued that many of these patients will not require TS evaluation or hospital admission. However, our data showed that 16% of the TR patients required admission to the TS and thus justifies the use of the ‘special considerations’ category of trauma triage criteria. Of note, the TR group was significantly older in comparison with the TA group, and ground-level falls were the most common mechanism of injury. Low-energy trauma mechanism, such as falls from standing, can be associated with significant injuries in the elderly but the physiological and anatomic findings may not rise to the level of TA, leading to undertriage in the field.9 20 21 Undertriage of these patients to non-trauma center can lead to increased mortality when compared with high-performing trauma centers.22 Other researchers have reported a 15% to 50% undertriage rate in those over 64 years of age.23 Additionally, Nakamura and colleagues stated that undertriage increases with age, and specifically found that those aged 45–54 years were associated with undertriage.24 However, if we aimed for decreasing undertriage rates by assigning TA for all middle-aged and elderly patients who sustain a ground-level fall, significant waste of unnecessary resources will occur. This will be an ongoing problem as the elderly population continues to increase in the USA and predictive factors for undertriage in the elderly will need to be studied more closely.21 25 Our study demonstrates one way to manage the undertriage problem in elderly patients, as well as patients on anticoagulants with minor trauma mechanisms.
Limitations of the study
This pilot represents one trauma center’s experience with a modified triage. The small sample of data is limited, and results may not be generalizable for all trauma centers.
Patient charges were used as a surrogate for hospital resources used which may not directly translate to cost, as compared with describing the response of staff (human) resources.
We relied solely on the Cribari matrix for calculating overtriage and undertriage. The Cribari matrix has been questioned for overestimating overtriage and undertriage.26
Conclusion
The TR tier designation has provided a safe and feasible method for our trauma center to decrease costs of overtriage while avoiding undertriage of the trauma patient. Through the addition of a rapid PS evaluation, we continue to improve the time to diagnostic testing in this population. Based on the results of this study, we propose future multicenter studies which use these methods to evaluate the large-scale applicability of this workflow. Refinement of TR utilization may lead to more cost-efficient delivery of trauma care.
Data availability statement
No data are available. Data are not in a repository state. Data sets will not be shared due to institutional restrictions in data use agreement but aggregate deidentified data supporting the findings of this study are available from authors upon reasonable request.
Ethics statements
Ethics approval
This study received research ethics review and approval from the Scripps Office for the Protection of Research Subjects (IRB-19-7325). There was no patient contact and no informed consent required.
Acknowledgments
The authors thank Marc Sedwitz, MD, J Gary Schwendig, MD, and Christine Wells, RN, for their help in implementing this study. The authors also acknowledge Jiayan Wang, BSPH, and Matthew Castelo, BS, for assistance with article preparation.
References
Footnotes
Presented at Poster presentation at the 77th Annual Meeting of the American Association for the Surgery of Trauma; San Diego, CA; September 25–28, 2018.
Contributors ISD, KBS, FSN and GTT were responsible for study design, analyses, interpretation, and article preparation. KBS, THD and DB were responsible for data management and acquisition. MG was responsible for study design and interpretation. FZZ and WLB were responsible for data analyses, interpretation and article preparation. All authors were involved in the drafting and critical revision of the article. All authors provided final approval of the version to be published.
Funding This study was funded by the Scripps Memorial Hospital Trauma Service Department Funding.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.