Article Text

Abstract
Background Angioembolization has been the gold standard for management of pelvic arterial bleeding, but applicability has been limited by delays in access at many trauma centers. We hypothesized that a quality improvement program to reduce time to start of angiography would be associated with lower in-hospital mortality in patients with pelvic fractures and shock.
Methods Retrospective study of adults with a pelvic fracture and vital signs consistent with shock admitted to a level I trauma center after the initiation of a quality improvement project to reduce the time to angioembolization (2012 to 2016). Time from admission to procedure start for hemorrhage control was examined based on destination and time of day. In-hospital mortality was the primary outcome and was compared with US benchmarks in the literature.
Results The study group included 424 patients with a mean Injury Severity Score of 41±14. Of these, 212 (50%) responded to resuscitation and were admitted to the intensive care unit; 143 (34%) patients went directly to interventional radiology (IR) with a median time to start of angiography of 86 minutes (IQR 66 to 116); and 69 (16%) patients went directly to the OR with a median time to start of operation of 52 minutes (IQR 37 to 73). There were no significant differences in time to procedures based on time of day or transfer status. In-hospital mortality for patients in shock on admission was 15%.
Discussion Patients with pelvic fracture and hemorrhagic shock, with a median time to angioembolization of <90 min, had a lower in-hospital mortality compared with published US benchmarks. These times were achieved by protocolization of pelvic fracture management that includes expeditious mobilization of the IR team, bypassing the CT scanner, and institutional quality metrics for compliance.
Study type Case series.
Level of evidence IV.
- pelvic fracture
- shock
- angiography
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
A recent multi-institutional study from the American Association for the Surgery of Trauma (AAST) reported a national benchmark for in-hospital mortality of 32% for patients admitted to level I trauma centers with pelvic fractures and hemorrhagic shock.1 Despite advances in resuscitation strategies, hemorrhage remains the most common cause of early death after injury, usually occurring within 3 hours of hospital admission.2 Although the majority of pelvic fracture hemorrhage is venous and can be managed with circumferential compression of the pelvis and a balanced blood product resuscitation, arterial bleeding can be life threatening and results in persistent hemodynamic instability. Patients with a pelvic fracture and shock who fail to respond to initial resuscitation, and who do not have evidence of other major sources of bleeding, require intervention to control arterial bleeding from the pelvis. Angiography with embolization is successful in >90% of patients and has been described as the gold standard for control of arterial pelvic hemorrhage.3–5 Availability of interventional radiologists to perform angiography within 30 minutes of notification for trauma-related bleeding is a required standard for level I and II trauma centers for verification by the American College of Surgeons Committee on Trauma.
Treatment algorithms for patients with pelvic hemorrhage are largely based on the availability of multidisciplinary resources and are institution-specific. The time delay to mobilize interventional radiology (IR) teams has limited the use of angioembolization in many centers. A recent study from Baltimore reported a median time of emergency department (ED) admission to angiography of 286 min, restricting the use of angioembolization to patients who survived the first 5 hours of hospitalization.6 As a result, preperitoneal packing (PPP) has been advocated as the standard initial approach to pelvic hemorrhage control.7–9 A recent series of 128 patients managed with initial PPP demonstrated a mortality of 21%.7 Although PPP has been demonstrated to be an effective, feasible and timely approach to obtaining pelvic hemostasis, the risk of infection and need for subsequent operations are not insignificant. Pelvic space infections are reported in 6% to 21% of patients who undergo a single packing of the pelvis, which increases dramatically with repacking of the pelvis (45%).7 10 11
The multidisciplinary trauma team at our level I trauma center has prioritized IR team mobilization to 30 minutes or less on activation.12 The purpose of this study was to examine time from admission to IR and operating room (OR) procedure start in patients presenting with pelvic fracture and shock, and to benchmark our single-center performance against the best available national data. We hypothesized that our IR mobilization time for patients with suspected pelvic bleeding was shorter than the reports from other level I trauma centers and that in-hospital mortality would be reduced.
METHODS
This is a retrospective cohort study of patients with pelvic fractures admitted to Harborview Medical Center (HMC) in Seattle, Washington, from January 2012 to December 2016. Patients 18 years and older with a blunt trauma mechanism were included in the study. Patients excluded from the study were those with isolated hip fractures, pregnancy or those with ongoing cardiopulmonary resuscitation (CPR) who died within 15 minutes of arrival to the ED because they were unlikely to benefit from an operation or angioembolization at the time of presentation. The trauma registry was queried for patient demographics, injury-specific data including mechanism of injury, type of admission (scene vs. interhospital transfer), time of admission (daytime vs. night/weekend), Injury Severity Score (ISS), admission vital signs, Glasgow Coma Scale (GCS) score and laboratory values. Outcome data, including trauma intensive care unit (ICU) and hospital length of stay (LOS), in-hospital mortality, cause of death and discharge disposition, were also obtained from the trauma registry. Procedures performed including pelvic angiography and angioembolization by IR, surgical intervention in the OR and procedure start times were extracted from the electronic medical records by chart review. Transfusion data were collected to document the number of units and timing of products administered to the patient. Chart review was conducted for all patients who died within 15 minutes of arrival to the ED and for patients who died within the first 48 hours to determine the suspected and/or actual cause of death, respectively.
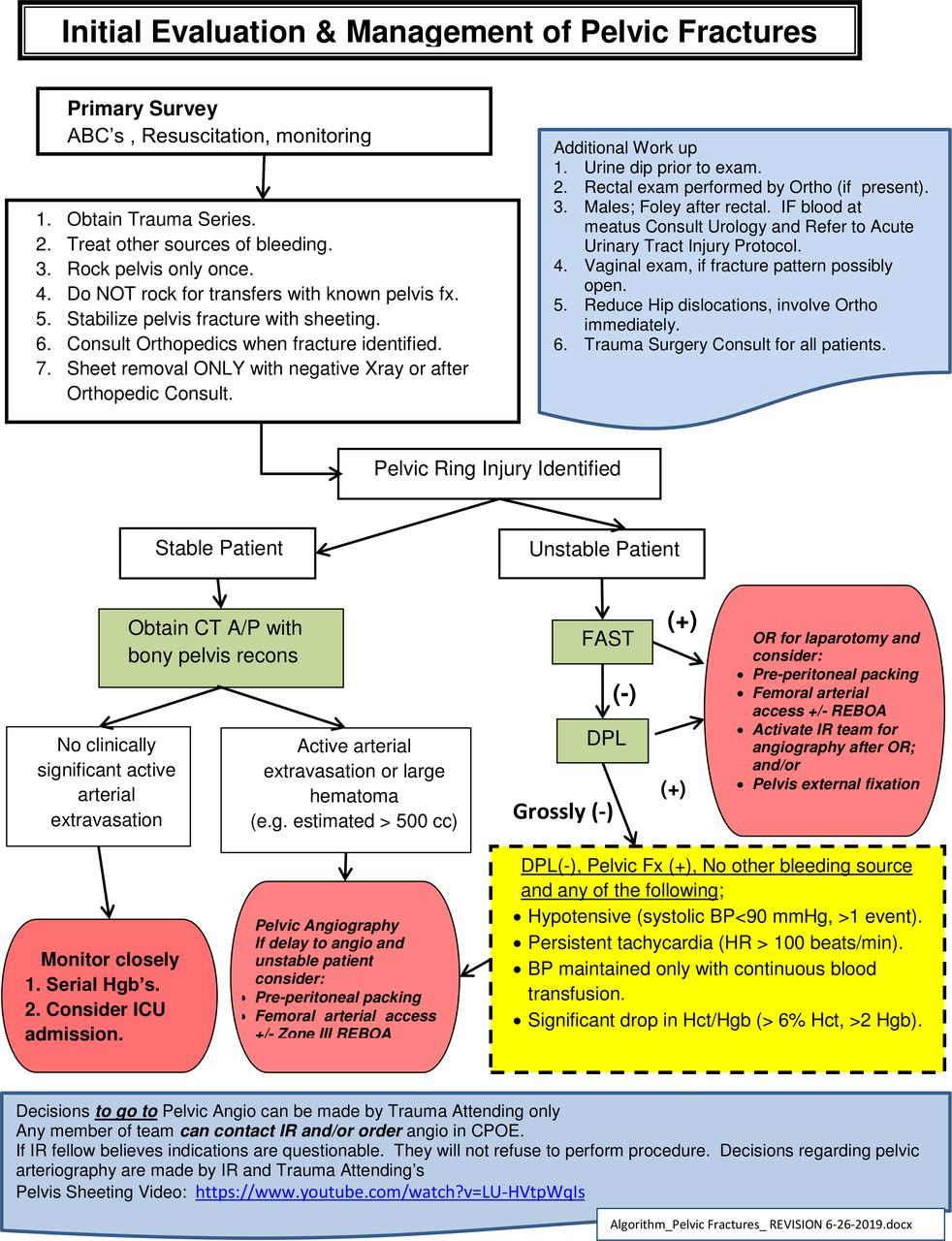
Patients who had pelvic fracture were managed via an institutional protocol that did not change during the study period (figure 1). All patients with pelvic fracture with abnormal hemodynamics underwent circumferential wrapping of the pelvis. If a prehospital binder had been placed in appropriate position this was left in place. If not, the pelvic volume was closed using a circumferential wrap with a bed sheet. The sheet was folded to a length of two feet and rolled at either end to meet in the middle. It was then positioned against the lateral pelvis and thigh, centered over the greater trochanter. With the patient in lateral decubitus and maintanence of full spinal precautions, the rolled sheet was passed to a partner across the table, pulled firmly in either direction and secured.13 This technique, which is performed routinely by orthopedic residents in the ED provides consistent closure of the pelvic ring, which is confirmed by X-ray. Simultaneously, resuscitation was initiated with a 1:1:1 ratio of plasma, platelets and red blood cells. Patients with evidence of major hemorrhage outside of the pelvis were transported directly to the OR for control of hemorrhage. Intra-abdominal bleeding was evaluated with focused assessment with sonography in trauma (FAST), and if equivocal, diagnostic peritoneal aspiration (DPA) was also performed. Patients for whom the primary site of bleeding was attributed to the pelvis were transported directly to IR for evaluation. The IR team was notified and expected to be ready to start the procedure within 30 minutes of notification. A radiology technician was in-house 24/7 to open the room so that the patient could be transported, positioned and prepped while the IR team was mobilized. Patients with persistent abnormal hemodynamics were not taken to the CT scanner. Resuscitative endovascular balloon occlusion of the aorta was available for placement in the ED or IR suite if needed.

Harborview Medical Center’s initial evaluation and management of pelvic fx algorithm. ABC, airway, breathing, circulation; A/P, abdomen/pelvis; CPOE, computerized provider order entry; DPL, diagnostic peritoneal lavage; Hct, hematocrit, Hgb, hemoglobin; BP, blood pressure; Fx, fracture; HR, heart rate; ICU, intensive care unit; IR, interventional radiology; OR, operating room; REBOA, Resuscitative endovascular balloon occlusion of the aorta.
The study group consisted of patients with a pelvic fracture who were in shock on presentation to the ED. To allow comparison to national benchmarks, the criteria used to define shock were based on those used in the AAST multi-institutional study by Costantini et al, which included any one of the following: initial systolic blood pressure (SBP) of <90 mm Hg, initial heart rate (HR) of >120 beats per minute (bpm) or base deficit of >6.1 The study group was examined based on their initial management pathway (ie, ED to IR, ED to OR, or ED to ICU).
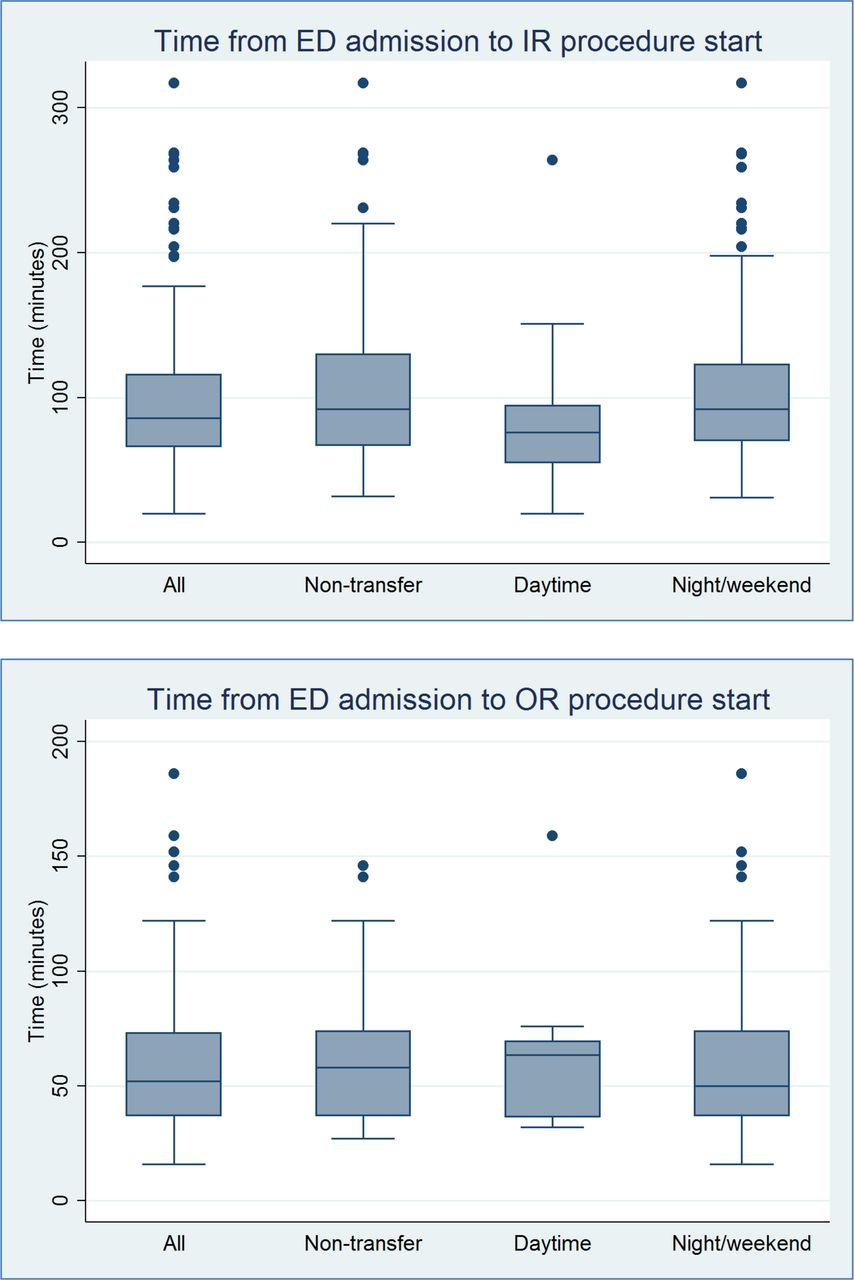
The length of time from ED admission to IR procedure start was analyzed and stratified by daytime admission, night/weekend admission and scene transports (not transferred from another hospital). Daytime admission was defined as 07:30 through 17:30 Monday to Friday, and weekend admission was defined as 17:31 Friday through 07:29 Monday as described by Schwartz et al.14 The number of units of packed red blood cells, plasma, platelets and cryoprecipitate transfused within the first 24 hours was analyzed by study group.
The primary outcome assessed was the incidence of in-hospital mortality. Benchmarks for mortality were obtained from the AAST multi-institutional study.1 Secondary outcomes assessed were time from ED admission to IR puncture time, time from ED admission to OR procedure start, ICU and hospital LOS and discharge disposition. Patient demographic and clinical data were described by shock status.
Continuous normally distributed data are presented as mean±SEs (SD), and non-normal data are presented as median±IQR. Patient outcomes were examined in bivariate analysis by shock status using Wilcoxon rank-sum test for continuous variables and χ2 test for categorical variables. Statistical significance was defined as p<0.05. Data analysis was performed using STATA MP V.13.1.
Results
From 2012 to 2016, there were 1182 patients admitted to HMC with a pelvic fracture. Twelve patients died within 15 minutes of arrival (five thought to be due to exsanguination and seven thought to be due to traumatic brain injury based on details from the prehospital course, physical exam findings, and initial workup) and were excluded from the analysis leaving 1170 patients. Twenty-five percent presented during the daytime (Monday to Friday, 07:30 to 17:30), and 75% presented during nights and weekends. Sixty-two percent of the patients were male, with a median age of 48 years (IQR 29 to 62). Sixty percent of patients were transferred from another hospital, and 11% were transferred from outside the state. The most common mechanism of injury for patients in this analysis was fall (28%), followed by motor vehicle collision (27%), pedestrian struck by car (18%), and motorcycle collision (12%). The mean ISS was 31 (±13.9). Table 1 demonstrates the demographic and injury-specific data of the overall cohort. For all patients with a pelvic fracture, the median ICU LOS was 3 days (IQR 1 to 7), and median hospital LOS was 9 days (IQR 5 to 18). The most common discharge destination was home (45%), followed by skilled nursing facility (42%). Four percent of patients died within 24 hours of admission, and overall in-hospital mortality was 8%.
Patient demographics and injury data
The study cohort consisted of the 424 (36%) patients with pelvic fractures who met criteria for shock (initial SBP<90 mm Hg or initial HR>120 bpm or base deficit >6) on admission. In this group, 68% were male, with a median age of 44 years (IQR 28 to 60). The mean ISS for the shock group was 41±13.8. Initial admission vital signs and exam findings were more abnormal compared with the overall cohort, with SBP of 107 mm Hg (IQR 85 to 126), heart rate of 113 bpm (IQR 90 to 128) and GCS score of 11 (IQR 3 to 15). Laboratory values on admission included median pH of 7.3 (IQR 7.2 to 7.3), base deficit of 7.2 (IQR 5.3 to 9.9), lactate of 3.6 (IQR 2.5 to 5.7) and hematocrit of 35 (IQR 30 to 39). Two patients underwent REBOA placement in the ED. Patients with shock had a longer median ICU LOS of 5 days (IQR 3 to 11) and longer median hospital LOS of 16 days (IQR 8 to 27) compared with the patients without shock (table 2).
Hospital outcomes in patients with pelvic fractures±shock
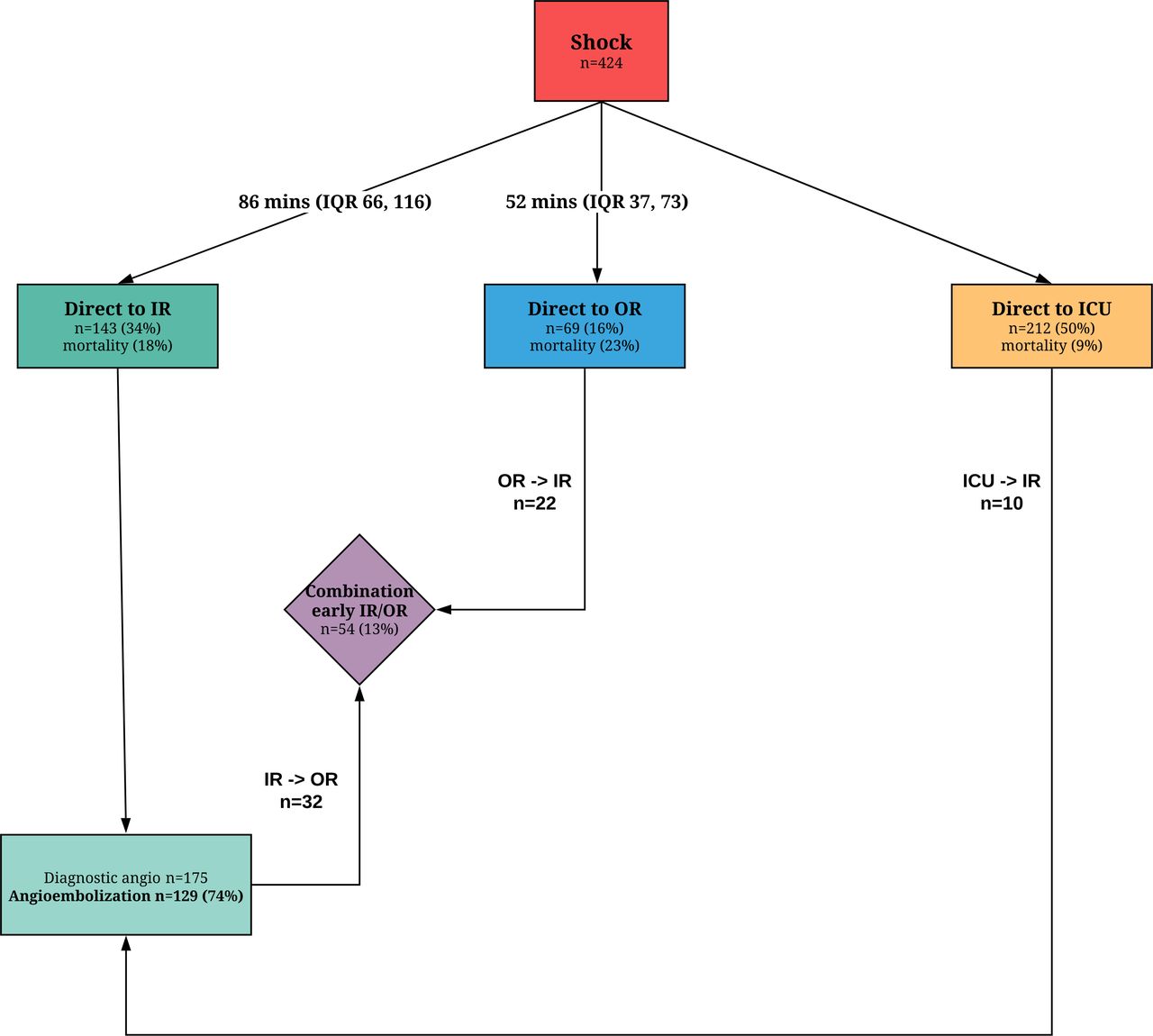
Figure 2 demonstrates the initial management of patients with pelvic fractures presenting in shock. There were 143 patients who screened negative for an intra-abdominal source of hemorrhage on FAST±DPA per the HMC’s initial evaluation and management of pelvic fractures algorithm (figure 1) and went directly to the IR suite from the trauma bay. Their median time from admission to IR procedure start was 86 minutes (IQR 66 to 116). This analysis included 11 patients whose time to IR was greater than 3 hours, all of whom either had delayed hemodynamic abnormalities or drop in hematocrit prompting evaluation by IR. When these patients with delayed signs of hemorrhage were excluded, the median time to IR was 79 minutes (IQR 57 to 104). There was very little variance in the time delay to IR procedure start when stratified by scene admission (excluding interhospital transfers) or by daytime versus night/weekend admission (figure 3). Of all patients with shock, 175 (41%) of patients underwent diagnostic angiography, and 129 (74%) underwent therapeutic angioembolization. Of the 216 patients with shock who arrived directly from the scene, 100 (46%) went to IR directly from the ED for diagnostic angiography, and 75 (75%) underwent therapeutic angioembolization. Despite meeting the AAST criteria for inclusion in the shock group, 212 (50%) of the patients responded to initial resuscitation and were admitted to the ICU. Ten of those patients demonstrated delayed hemodynamic changes or decreased hematocrits necessitating IR intervention for hemorrhage control (figure 2).

Initial management of patients with pelvic fractures presenting in shock. ICU, intensive care unit; IR, interventional radiology; OR, operating room.
{kind=link}
{kind=link}
{kind=link}
Time delay to IR/OR based on transfer status and time of admission. Boxes demonstrate the first to third quartiles with the line inside the box indicating median time from ED admission to IR procedure start. Whiskers indicate the degree of variability of time points, and the dots indicate outliers in each group. ED, emergency department; IR, interventional radiology; OR, operating room.
Sixty-nine (16%) patients went directly to the OR from the trauma bay, with a median time from admission to operation start of 52 minutes (IQR 37 to 73). Fifty-four (13%) of the patients with shock underwent a combination approach with both early surgical and IR interventions. Only time to first intervention (either IR or OR) was analyzed in this combination group. Early operations included 80 exploratory laparotomies, 7 thoracotomies, 5 craniotomies, 2 amputations and 3 vascular procedures. Eight (2%) patients underwent PPP, with an in-hospital mortality of 50%.
Transfusion data are demonstrated in table 3. Patients who went directly to IR from the trauma bay received less Packed red blood cells (p=0.001), plasma (p=0.007) and platelets (p=0.025) within the first 24 hours of admission than patients taken directly to the OR. Patients who went directly to the ICU had the lowest transfusion requirements of the three groups.
Initial 24-hour transfusion requirements of patients with pelvic fractures and shock
Forty-five (10.6%) patients with shock died within 48 hours of admission, with severe traumatic brain injury as the leading cause of death (17 patients). Twelve (2.8%) patients died secondary to uncontrolled hemorrhage, including 8 (1.9%) patients with uncontrolled pelvic hemorrhage (three died in the OR, 2 died in IR, 3 died in ICU after transition to comfort-focused treatments). Nine patients died within 30 minutes of arrival to the ED with unknown cause of death, the majority of which underwent prehospital CPR. Overall, in-hospital mortality for all patients with pelvic fracture was 8%, 15% for patients in shock, 18% in patients who went directly to IR, 23% in patients who went directly to the OR and 10% for those admitted directly to the ICU. Mortality was lower for patients in shock who were transferred from another institution versus those admitted directly from the scene (9% vs. 21%).
Discussion
The goal of this study was to examine our multidisciplinary trauma team’s performance in the initial management of patients with complex pelvic fractures and hemorrhagic shock, and to benchmark our outcomes relative to the best available national data. Studies have highlighted significant delays to angioembolization in level I trauma centers, which has contributed to an increased use of PPP to attempt timely hemorrhage control.6 14 A recent study using data from the American College of Surgeons Trauma Quality Improvement Project reported that delays to pelvic embolization were associated with increased in-hospital mortality, (OR 1.79 for each hour delay, 95% CI: 1.11 to 2.91, p=0.018).15
To benchmark our results, we matched the time period and the criteria for shock used in the 2015 AAST multi-institutional study examining the current management of hemorrhage from severe pelvic fractures at 11 level I trauma centers in the United States.1 Among all pelvic fracture admissions, our center had a higher proportion of patients that met the shock criteria (36% vs. 13%), and were more severely injured (mean ISS 41 vs. 28, AIS chest ≥3 60% vs. 49%, AIS abdomen≥3 34% vs. 32%). For patients with shock in our center, angiography was used more frequently (41% vs. 25%) compared with the AAST multi-institutional study. In-hospital mortality in our study was 15%, which benchmarks favorably compared with 32% mortality in the AAST trial (table 4).
Comparison to benchmark AAST multi-institutional study1
The delay in control of pelvic bleeding that is associated with IR mobilization is a deterrent to routine use in many centers. Time to angiography was not reported in the AAST trial, however, contemporary series have reported times far in excess of 90 min.6 7 14 The group from Maryland Shock Trauma published a median time to angiography of 286 minutes (IQR 210, 378) in patients with SBP ≤90 mm Hg or heart rate ≥120 beats per minute, and an associated mortality of 28%.6 The majority of these patients underwent a CT abdomen/pelvis prior to angiography (79%), which accounted for 99 minutes (IQR 75, 130) of the delay to angiography. Similarly, the Houston group documented considerable delays to start of angiography that were more prominent on nights/weekends with a median delay of 301 minutes (IQR 211, 389), compared with daytime delays of 193 minutes (IQR 137, 275).14 CT abdomen/pelvis accounted for a median delay of 176 minutes (IQR 133, 270) during nights/weekends and 87 minutes (IQR 56, 181) during the daytime. Our institutional pelvic fracture management algorithm discourages the use of CT scan in patients with pelvic fracture on X-ray, abnormal hemodynamics, and who screen negative for intra-abdominal bleeding (figure 1). Bypassing the CT scan on the way to the IR suite was a key factor in obtaining lower time to angiography in the current study.
PPP is not commonly used for pelvic fracture hemorrhage control in level I trauma centers and was rarely used in our center (2%) or the AAST multi-institutional study (5%), which included 11 major level I trauma centers.1 Notably, there was a subset of patients in the AAST multi-institutional study who were not in shock and still underwent PPP, demonstrating that this technique is being used in patients with lower acuity. Major risks associated with routine use of PPP include the necessity for subsequent operations, 16% requiring pelvic repacking and 12% incidence of pelvic space infections.7 A recent systematic literature review and practice management guideline from the Eastern Association for the Surgery of Trauma was unable to recommend for or against the initial use of PPP versus angioembolization based on the available evidence.16 PPP was conditionally recommended when angioembolization was not immediately available.
How much of a time delay is considered reasonable to proceed directly to angioembolization versus PPP remains unclear. Burlew et al reported a median time to the OR of 44 minutes (range 0 to 274 minutes).7 In our series, patients were only taken to the OR if a significant source of hemorrhage other than the pelvis required intervention. Our median time to OR was also shorter than our time to IR intervention, 52 minutes (IQR 37,73) versus 86 minutes (IQR 66,116). Mortality was higher in the direct to OR patients (23%) versus direct to IR patients (18%), which is likely explained by multiple sites of hemorrhage in the OR group. Overall, our data would suggest that a 30-minute target for mobilization of the IR is not unreasonable and emphasizes the importance of focused and continuous ongoing quality improvement efforts in our trauma centers.
The expectation at our institution is that the IR team will be in the hospital within 30 minutes of activation, as per the requirement of the American College of Surgeons Committee on Trauma.12 Time of activation is difficult to capture and so ED door-to-puncture time for patients taken directly to angiography is a quality metric that is monitored and reviewed by the trauma program and reported at the multidisciplinary trauma quality improvement (QI) meetings, analogous to the quality assurance programs for our acute stroke and cardiac programs. An IR technician is in the hospital 24 hours every day to facilitate preparation of the IR suite on activation of the team, and the patient can be transported to IR and positioned and prepped by the technician while the IR team is mobilized. This study demonstrates that when IR team mobilization is prioritized, supported and monitored at the institution level, reduced time to angioembolization is feasible.
This study has several limitations. A limitation is the retrospective nature of data collection, which made determination of the exact timing of interventions challenging. Consequently, extensive chart review was performed to extract relevant data from procedure notes and IR logs. Forty-nine percent of patients with shock were transferred from other institutions, which could impact the time to IR by prenotification of the team and potentially contribute to survival bias. We did not observe a significant difference in the time to IR for the transfer versus non-transfer patients, but transfer patients had an overall mortality of 9% compared with 21% for the non-transfer patients.
Thus, mortality in our patients arriving directly from the field benchmarks favorable to the AAST trial results and the isolated PPP cohort in the report from Denver, but, importantly, our protocol avoids the recognized significant complications of PPP. In addition, essentially half of all patients with pelvic fractures who met the AAST multi-institutional study criteria for shock did not require an acute hemorrhage control intervention (neither IR nor OR, including PPP). The same was true for 68% of the shock group in the AAST study, suggesting that either the criteria to designate shock was too broad or these patients had venous bleeding that was responsive to pelvic circumferential compression and resuscitation without the need for further intervention.
Although it may be necessary to implement use of PPP in facilities with limited local resources and time delays to angiography, this study demonstrates that use of strategies to reduce IR mobilization times at the institution level (complex pelvic fracture protocol development bypassing diagnostic CT scan for patients in shock, in-house IR technician, and quality improvement monitoring by a multidisciplinary council) can prove to be successful and appears to be associated with improved patient outcomes. This evaluation of our institution’s performance has reinvigorated our multidisciplinary effort to achieve further reductions in delays to angiography, especially in light of significantly lower in-hospital mortality and avoidance of morbid invasive procedures in this high-risk group of patients.
Footnotes
Contributors KMOC: conception and study design, data acquisition, statistical analysis, interpretation of data; drafting and revision of the article; approval of the final article version to be published. SK, KA and SJ: conception and study design and data acquisition; drafting and revision of the article; approval of the final article version to be published. QQ: data acquisition, statistical analysis, and interpretation of data; drafting and revision of the article; approval of the final article version to be published. CI, FR, MSV, RM and EMB: conception and study design and interpretation of data; drafting and revision of the article; approval of the final article version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The University of Washington institutional review board (ID STUDY00000505) approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author, KO, upon reasonable request.