Article Text

Abstract
Background Reports indicate social distancing guidelines and other effects of the COVID-19 pandemic impacted trauma patient volumes and injury patterns. This report is the first analysis of a large trauma network describing the extent of these impacts. The objective of this study was to describe the effects of the COVID-19 pandemic on patient volumes, demographics, injury characteristics, and outcomes.
Methods For this descriptive, multicenter study from a large, multistate hospital network, data were collected from the system-wide centralized trauma registry and retrospectively reviewed to retrieve patient information including volume, demographics, and outcomes. For comparison, patient data from January through May of 2020 and January through May of 2019 were extracted.
Results A total of 12 395 trauma patients (56% men, 79% white, mean age 59 years) from 85 trauma centers were included. The first 5 months of 2020 revealed a substantial decrease in volume, which began in February and continued into June. Further analysis revealed an absolute decrease of 32.5% in patient volume in April 2020 compared with April 2019 (4997 from 7398; p<0.0001). Motor vehicle collisions decreased 49.7% (628 from 1249). There was a statistically significant increase in injury severity score (9.0 vs. 8.3; p<0.001). As a proportion of the total trauma population, blunt injuries decreased 3.1% (87.3 from 90.5) and penetrating injuries increased 2.7% (10.0 from 7.3; p<0.001). A significant increase was found in the proportion of patients who did not survive to discharge (3.6% vs. 2.8%; p=0.010; absolute decrease: 181 from 207).
Discussion Early phases of the COVID-19 pandemic were associated with a 32.5% decrease in trauma patient volumes and altered injury patterns at 85 trauma centers in a multistate system. This preliminary observational study describes the initial impact of the COVID-19 pandemic and warrants further investigation.
Level of evidence Level II (therapeutic/care management).
- COVID-19
- wounds and injuries
- outcome assessment
- health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Early anecdotal reports indicate trends in trauma volumes and injury patterns may have changed significantly as a result of national social distancing guidelines enacted on March 16, 2020,1 2 after the WHO’s declaration of the COVID-19 pandemic.3 In comparing 2020 to 2019, trauma centers across the USA have reported differing results, with Santa Clara County, California,4 New Hampshire,5 and Minnesota all reporting decreased trauma volume and changes in pattern of injury,6 whereas a report from Kentucky noted comparable trauma volume.7 Additional anecdotal evidence reported decreased trauma volumes in Fort Worth, TX, Vacaville, CA, Allentown, PA, and Ann Arbor, MI.8 Although the majority of the reports indicated decreased trauma admissions and changes in injury patterns, they were only representative of single institution experiences and no comprehensive reports have appeared from large trauma systems describing the impact of the COVID-19 pandemic on trauma volumes and patient characteristics. The primary aim of this study was to compare trauma volumes during the first 5 months of 2020 to those in the year preceding the pandemic in a large, multistate network of trauma centers. Secondary aims were to describe variations in patient and injury characteristics and patient outcomes in the pre-COVID-19 versus active-COVID-19 periods within the same trauma center network.
Methods
Adult (>18 years) trauma patients were selected from all entries of the enterprise-wide trauma registry of the eligible trauma centers in a national multistate healthcare system. Eligible trauma centers were those that entered trauma patients into their trauma registry for the two assessed time frames. Data from the first 5 months of 2020 were compared with the same time frame in 2019. Data extraction was performed in mid-July 2020. As national ‘shelter-in-place’ orders were instituted on March 16, 2020, a focused analysis of trauma activation and admissions in April 2020 were compared with those in April 2019.
Data were collected from the enterprise-wide trauma registry containing patient record-level data conforming to the National Trauma Data Standard. Date of arrival was collected for all included patients to determine total trauma patient volume. A focused subset analysis of patients who arrived in April 2020 compared with April 2019 included additional data on arrival dates, patient characteristics, injury characteristics, and outcomes. To describe details of patients’ mechanism of injury, International Statistical Classification of Diseases and Related Health Problems, Tenth Revision external cause-of-injury codes were categorized based on the Centers for Disease Control and Prevention recommended trauma groupings.9 Patients were stratified by age groupings as described by Geifman et al, which consisted of Adults (18 to 64 years), the Elderly (65 to 79 years), and the Very Elderly (≥80 years).10 Payor source stratification was grouped as Medicare, Medicaid, Other Government, Private, Self-pay, and Other. Trauma centers were grouped into regions as defined by the US Census Bureau.11
Trends in trauma patient volume data from January through May of 2020 and the same time frame in 2019 were analyzed for differences between years and illustrated graphically. Emphasis was placed on comparisons of the month of April for each respective year, which is representative of the early phase of the pandemic in the USA. Daily hospital admissions were plotted using a locally weighted scatter-plot smoother curve. Descriptive statistical analysis was performed to analyze trends in trauma care between April 2020 and April 2019. To calculate a p value for the absolute volume percentage decrease, Pearson χ2 was used to calculate a p value for the test statistic, under the null hypothesis of no volume difference between the years. Patient characteristics, injury characteristics, and outcomes including patient volume, hospital length of stay (LOS), and mortality were compared between years using univariate analyses, including Pearson χ2 for categorical variables and Wilcoxon rank-sum for continuous variables. Presented data demonstrate both proportional categorical shifts, as well as absolute changes. R software V.3.6.2 was used for all statistical analyses, and p values less than 0.05 were considered statistically significant. This research was analyzed to be exempt or excluded from Institutional Review Board (IRB) oversight in accordance with current regulations and institutional policy.
Results
Of the 94 trauma centers in the system, 9 were excluded due to lack of complete patient data from the two assessed time periods, leaving 85 hospitals included in the final analysis. Of the 85 hospitals, 8 (9.4%) were level I centers, 36 (42%) were level II centers, and 26 (31%) were level III centers. The majority of the centers were in Region 3 (59 of 85, 69%), which represented facilities located in the South. Trauma center level and region are listed in table 1.
Description of center-specific patient volume change and location of hospitals contributing to the enterprise-wide trauma registry
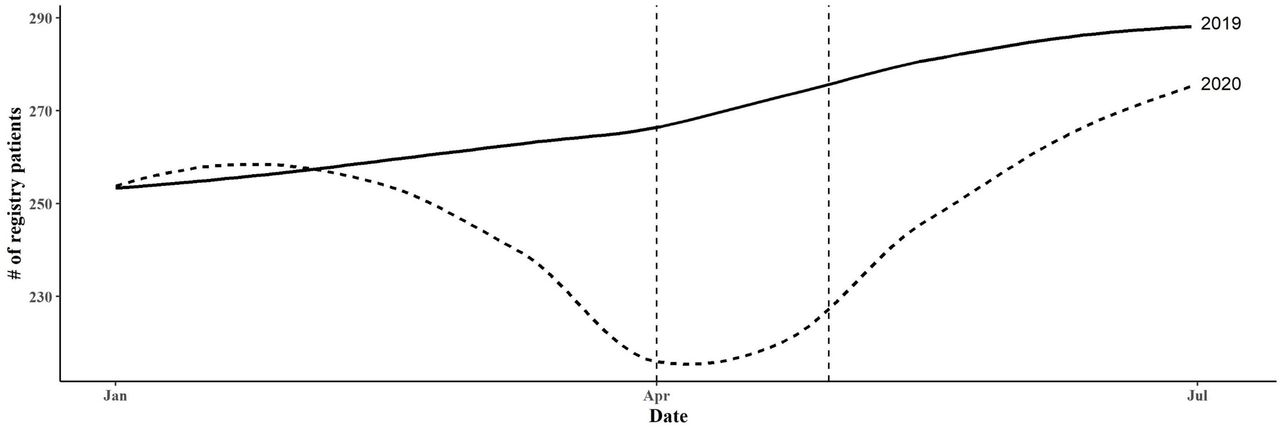
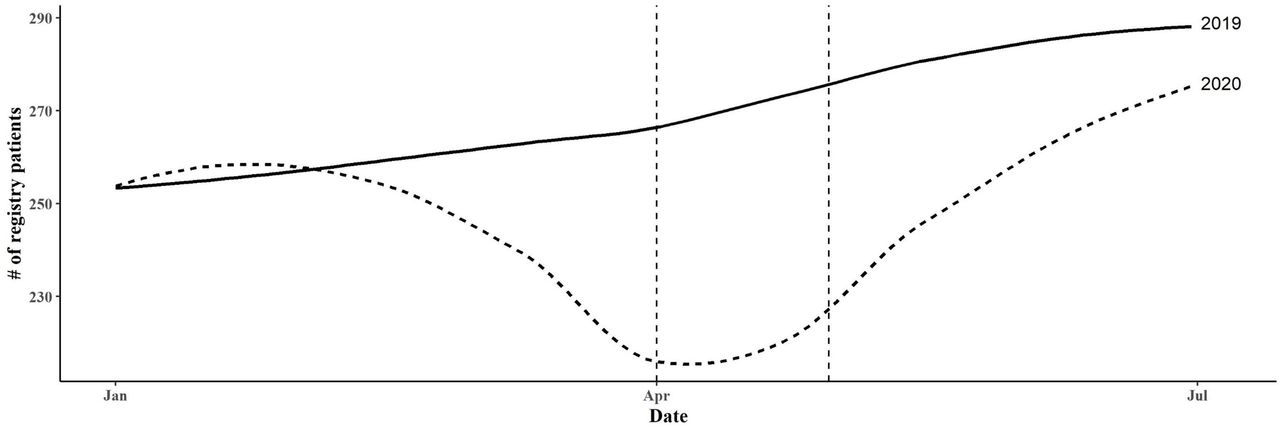
Data from the first 5 months of 2020 compared with the same time frame in 2019 in this large network of trauma centers demonstrated a substantial absolute volume decrease in patients entered into the enterprise-wide trauma registry, which began in February 2020, and continued to decline into June 2020 (figure 1). A focused comparative analysis of April 2020 to April 2019 displayed a substantial absolute volume decrease in trauma patients in the 85 facilities across the USA. Trauma volume decreased 32.5% to 4997 patients in April 2020 compared with 7398 patients in April 2019, p<0.0001. Although 69 (81%) of the centers experienced a decrease in trauma patients, this difference varied across individual hospitals, regions, and trauma center levels. Level I, II, and III centers experienced a median trauma patient absolute volume decrease of 27.6%, 24.8%, and 22.5%, respectively, whereas level IV centers experienced a median decrease of 38.6% (table 1). There was variability among individual level IV sites, with several showing smaller decreases, or even increases from year to year.
{kind=link}
Daily number of registry patient arrivals at a network of 85 hospitals. Daily number of registry patient arrivals are shown from January through May of both 2019 and 2020 for comparison. Locally estimated scatterplot smoothing splines are used to represent registry patient arrival counts. The dashed line represents 2019 and the solid line represents 2020. Vertical dotted lines are used to highlight the month of April for 2019 and 2020.
There was a significant difference in the proportion of trauma activation types when comparing April 2020 to April 2019, with fewer partial activations and consultations and an increase in non-activations (table 2). Although the percentage of full activations remained similar from year to year, there was a significant proportional shift (as a proportion of all trauma activation types) in other activation categories, with a 4.8% decrease in partial activations, and a corresponding 2.6% increase in consultations. A significant difference in the proportion of transfers was not detected.
Comparison of April 2019 and 2020 trauma activations
Individual patient characteristics are shown in table 3. There were no significant differences in mean age, age groupings, gender or race distribution between patients admitted in April 2020 versus those admitted in April 2019 (table 3). An increase in the proportion of men (2.2%) who presented to trauma centers was noted between the 2 years (p=0.016). Payor comparison between the 2 years demonstrated there to be a decrease in the proportion of patients with private insurance (26.4% in 2020 vs. 28.1% in 2019, p=0.035), and an increase in the proportion of uninsured Self-pay patients (18.6% in 2020 vs. 15.8% in 2019, p<0.001) in 2020 compared with 2019.
Comparison of April 2019 and 2020 patient characteristics
The type and severity of injures were statistically significantly different when comparing 2020 to 2019 (table 4). There was a statistically significant increase in injury severity score (ISS) to 9.0 in April 2020 from 8.3 in April 2019 (p<0.001). The distribution among ISS classification was significantly different between the 2 years, with a 5.6% decrease in proportion of mild injuries, and increases of 3.3% in moderate (p<0.001) and 1.5% in severe injuries (p=0.002). Statistically significant differences were also noted among Glasgow Coma Scale (GCS) mean and distribution (p=0.009), with a statistically significant increase (4.9% from 4.1%) in the proportion of patients that presented with a severe GCS between three and eight (p=0.018).
Comparison of April 2019 and 2020 injury characteristics and patient outcomes
The absolute numbers of both blunt and penetrating injury volumes decreased when comparing 2020 to 2019 (table 4). Although the percent volume decrease year-to-year of blunt injuries was 34.8% (4364 from 6692), penetrating injuries only decreased 6.9% (500 from 537). As a proportion of the injury types between years, there was a statistically significant decrease of 3.1% in the proportion of those with blunt injuries and a corresponding increase in the proportion of penetrating injuries of 2.7% (p<0.001) in 2020 compared with 2019. Statistically significant increases in the proportion of firearm injuries (212 from 204;1.5%) and cut/pierce injuries (291 from 259;1.2%) were observed comparing April 2020 to April 2019 (p<0.001), as well as a significant absolute decrease of 49.7% in total motor vehicle collisions (MVC) to 628 in April 2020 from 1249 in April 2019. Of note, there was also a statistically significant increase in the mean ISS for patients admitted for MVC to 11.1 from 10.0 (p=0.003), although this has limited clinical impact.
Comparisons of patient outcomes are listed in table 4. There was a statistically significant absolute decrease in hospital LOS to 4.5 days in April 2020 from 5.1 days in April 2019 (p<0.001), and a statistically significant increase in the unadjusted proportion of patients who did not survive to discharge (3.6% from 2.8%; p=0.01). Of those discharged alive, there was a statistically significant decrease in patients who were discharged to a skilled nursing facility (26% from 27.7%; p=0.038), although this may have limited clinical significance.
Discussion
Using data from 85 trauma centers in a national healthcare system, this study found that the absolute number of trauma patients decreased significantly in 2020 during the initial months of the COVID-19 pandemic after the implementation of shelter-in-place guidelines.1 Furthermore, compared with April 2019, patients in April 2020 were more severely injured, suffered an increase in the relative proportion of penetrating firearm and cut/pierce injuries, experienced an absolute decrease in hospital LOS, and had a proportional shift in payor source distribution, with more uninsured patients encountered in 2020.
In April 2020, 81% of the trauma centers experienced a decrease in enterprise-wide trauma patient registry volume compared with April 2019. This varied across individual hospitals, regions, and trauma center levels, with a few level IV trauma centers experiencing an increase in volume during April 2020 compared with April 2019. These findings are consistent with several—but not all—previous reports from the USA.4 5 7 The observed differences in reported trends may reflect the disparate incidence of the disease, and the varied application of social distancing and other precautionary measures within different regions of the USA. There have also been reported global trends reflecting reductions in hospital volume during COVID-19 restriction periods.12–15 This study of a large healthcare system revealed similar results to most national and international studies, with an average decrease of 32.4% in enterprise-wide trauma patient registry volume.
Differences in injury patterns were detected in the present study, with a proportional (but not absolute) increase in penetrating injuries when comparing April 2020 to April 2019. During this time frame, there was also an observed proportional increase in firearm-related injuries and cut/pierce injuries among the participating trauma centers as noted in other reports.7 12 A decrease in MVCs was also observed, consistent with findings in Florida, New York, Massachusetts,16 and New Hampshire.5 This large decrease in MVCs likely represents lower volumes of road traffic due to the shelter-in-place orders, and/or decreased employment.17 18 Changes in penetrating injury patterns may be related to psychosocial pressures due to school closings,19 job layoffs,20 or social isolation.21 This suggests that as additional quarantines or shelter-in-place orders are implemented, trauma centers may see further changes in injury patterns, including more penetrating trauma and injuries related to lockdown fatigue (such as domestic violence, child abuse/neglect, self-harm). Outreach and injury prevention messaging may be useful in response to changing injury patterns. Although some of the observed changes in injury patterns have minimal clinical significance, this early report may portend future, more significant changes as the pandemic expands. Centers may be able to focus surveillance efforts in specific areas to guide future operational responses and public health messaging.
The COVID-19 pandemic created unprecedented challenges for America’s hospitals. Hospitals reduced staff as elective surgery rates fell dramatically, potentially impacting surge capacity for complex trauma and mass casualty events. Unexpected and unpredictable trauma volume trends may impact staffing schedules and work duties and require development of response plans, such as described by Ross et al.22 Opportunities may exist for reallocation of personnel and other resources typically reserved for trauma to other areas within the hospital or the healthcare system where the need is greatest.23 Since many trauma surgeons are trained and experienced in critical care, they may be able to assist in the care of patients with COVID-19 in critical care settings if their surgical workload is reduced. Similarly, critical care units that normally house significant numbers of trauma patients can become backup units in support of medical intensive care units that have reached capacity. However, major adjustments to trauma staffing and physical resource allocation should be approached cautiously as it is possible that trauma resources can become overwhelmed by unpredictable events such as disasters and mass casualty events.
This study also revealed a significant shift in payor sources comparing 2020 to 2019, with a decrease in patients with private insurance, and a corresponding increase in uninsured patients. An analysis of the age group below Medicare eligibility (18 to 64 years) revealed a significant increase in the proportion of uninsured trauma patients. This shift may be due to loss of medical insurance associated with sudden unemployment, as well as other factors, and warrants further investigation to analyze future responses to pandemic situations which may require modifications to our healthcare reimbursement system. The findings of decreased volumes and higher rates of uninsured patients may disproportionally impact smaller medical centers which are already under great pressures in such crises.
Future research should continue to evaluate trends in trauma activations and admissions during the COVID-19 pandemic. As the pandemic continues, identifying patterns of traumatic injury may guide injury prevention strategies, as well as future planning and management of potential influxes of trauma and critical care patients. These findings may also influence staffing and resource allocation decisions within individual hospitals and healthcare systems.
This study has several limitations, as it is retrospective data from an enterprise-wide trauma registry, which is not solely designed for research, and may have included potential data entry errors. These data represent a large, multistate healthcare system at a single point in time and is oversampled in the South, which may not have experienced the same effects of COVID-19 as other regions with high COVID-19 volumes, such as the Northern, Northeastern, and upper Midwestern US.24 25 As such, different regions of the USA and the world experienced the effects of the pandemic at different times and at different levels of severity, making it likely that all the emerging data should be interpreted with those caveats. It is likely that once the pandemic has been controlled, a more comprehensive review of more global data will provide a more complete picture of the full effect of this outbreak. Changes in trauma activations may be the result of local changes in activation criteria and/or regional differences in the severity of, and response to, the pandemic. This was an observation of the response to the initial impact of COVID-19 relative to the March 16, 2020 social distancing guidelines, whereas different locations may have implemented emergency responses to the COVID-19 pandemic at different times.
Conclusion
Early phases of the COVID-19 pandemic resulted in significant decreases in the number of trauma registry patients and altered injury patterns among 85 trauma centers, likely due to the national social distancing guidelines enacted in March 2020. A statistically significant decrease in overall trauma registry patient volume was observed, with fewer injuries from MVCs, a relative increase in penetrating injuries (including firearm injuries), and slightly higher ISS—although the increase in ISS was of limited clinical significance. An increase in the proportion of patients who were uninsured was also observed. These shifts in trauma patterns are concerning consequences of the pandemic and the initial viral transmission prevention measures that have been implemented. Adjustments in trauma center staffing and response models may be needed if these shifts persist or are exacerbated underlining the need for continued real-time tracking of volumes and patterns. In addition, public health messaging to educate the public on more relevant home-based injury prevention and lockdown resilience may be indicated.
Footnotes
Contributors All authors certified they made contributions in design, data acquisition, data analysis/interpretation, and drafting/revising the article. Authors have given approval of the version to be published.
Funding This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity.
Disclaimer The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This research was analyzed to be exempt or excluded from Institutional Review Board (IRB) oversight in accordance with current regulations and institutional policy by HCA Corporate Research Compliance. The internal reference number for this determination is 2020-441.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study have been included in the article.