Article Text

Abstract
Background The Glasgow Coma Scale (GCS) score has been adapted into categories of severity (mild, moderate, and severe) and are ubiquitous in the trauma setting. This study sought to revise the GCS categories to account for an interaction by age and to determine the discrimination of the revised categories compared with the standard GCS categories.
Methods The American College of Surgeons National Trauma Data Bank registry was used to identify patients with traumatic brain injury (TBI; ICD-9 codes 850–854.19) who were admitted to participating trauma centers from 2010 to 2015. The primary exposure variables were GCS score and age, categorized by decade (teens, 20s, 30s…, 80s). In-hospital mortality was the primary outcome for examining TBI severity/prognostication. Logistic regression was used to calculate the conditional probability of death by age decade and GCS in a development dataset (75% of patients). These probabilities were used to create a points-based revision of the GCS, categorized as low (mild), moderate, and high (severe). Performance of the revised versus standard GCS categories was compared in the validation dataset using area under the receiver operating characteristic (AUC) curves.
Results The final population included 539,032 patients with TBI. Age modified the performance of the GCS, resulting in a novel categorization schema for each age decile. For patients in their 50s, performance of the revised GCS categories mirrored the standard GCS categorization (3–8, 9–12, 13–15); all other revised GCS categories were heavily modified by age. Model validation demonstrated the revised GCS categories statistically significantly outperformed the standard GCS categories at predicting mortality (AUC: 0.800 vs 0.755, p<0.001). The revised GCS categorization also outperformed the standard GCS categories for mortality within pre-specified subpopulations: blunt mechanism, isolated TBI, falls, non-transferred patients.
Discussion We propose the revised age-adjusted GCS categories will improve severity assessment and provide a more uniform early prognostic indicator of mortality following traumatic brain injury.
Level of evidence III epidemiologic/prognostic.
- brain injuries
- traumatic
- Glasgow Coma Scale
- geriatrics
- mortality
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Traumatic brain injury (TBI) remains a significant cause of mortality despite improvements in prevention and treatment.1 2 Several prognostic indicators of mortality following TBI have been reported, chief among them are neurologic status and patient age.3–5 Neurologic status is typically measured using the Glasgow Coma Scale (GCS) score, where clinicians evaluate central nervous system function through verbal, motor, and eye-opening responses to stimuli.6
Many major organizations, including The American College of Surgeons (ACS) Advanced Trauma Life Support manual, the Eastern Association of the Surgery of Trauma, and the Centers for Disease Control and Prevention, use the GCS score to classify TBI into categories of mild (13–15), moderate (9–12), and severe (3–8). However, age is known to affect TBI, including the initial physiologic response (eg, presenting GCS), specific CT findings, aggressiveness of neurosurgical management, and morbidity and mortality.7 The trauma population,8 9 and specifically the TBI population,10 is aging and revision of these GCS severity categories may be warranted to reflect the age distribution of the current trauma population.
Previously, we demonstrated that injured elderly patients present to the hospital with more favorable GCS scores compared with younger patients, despite having the same anatomic severity and worse outcomes.11 These findings have been substantiated by publications examining differences in GCS scores for younger adults versus elderly (≥65 years) patients.12–14 However, this age threshold of ≥65 years is arbitrary,15 and it is not known when the interaction between GCS score and age for other outcome/severity begins.
To address this gap in the literature, we sought to account for any observed variation by age by revising the GCS score categories (mild, moderate, severe) and determine whether the discrimination of the revised categories is improved compared with the standard GCS categories.
Methods
Design, setting, and participants
The ACS National Trauma Data Bank (NTDB)16 was used to identify trauma patients who presented between 2010 and 2015 with a TBI, defined by ICD9-CM diagnostic codes 850.0 through 854.19. Patients at participating US trauma centers are included in the NTDB based on ICD-9-CM diagnosis codes 800–959.9 and who were admitted to the hospital, died after being evaluated, or were dead on arrival.
Patients were excluded from our study if they were missing an emergency department (ED) GCS score, if age was missing or the patient was <10 or >89 years, or the ED GCS score was recorded while the patient was chemically sedated, intubated, or paralyzed.
Prior to analysis, the study population was randomly divided into two subsets: a model development dataset consisting of 75% of the total sample and a model validation dataset consisting of the remaining 25%.
Primary variables of interest
The primary outcome variable used for metric generation was in-hospital mortality. The main independent variables of interest were age and GCS score. Age was examined by decade (teens, 20s, 30s, 40s, 50s, 60s, 70s, and 80s), and the GCS recorded on arrival to the ED was examined first by total GCS score (3–15) and then by GCS category.
Secondary outcomes used for metric validation included neurosurgical intervention, unfavorable discharge disposition, and in-hospital mortality occurring within the following subpopulations defined a priori: (1) isolated TBI, defined by Abbreviated Injury Scale (AIS) scores ≤1 in non-head regions; (2) fall as a cause of injury; (3) non-transferred patients; (4) blunt mechanism; (5) penetrating injury. Neurosurgical intervention was identified by ICD-9-CM procedure codes 01.01–02.31 (incision and excision of skull, brain, and cerebral meninges, cranioplasty, repair of cerebral meninges, ventriculostomy, extracranial ventricular shunt) and 02.91–02.99 (other operations on skull, brain, and cerebral meninges). Unfavorable discharge disposition was defined as discharge to morgue, hospice, long-term care facility, skilled nursing facility, intermediate care facility, short-term general hospital for inpatients, or a rehabilitation facility.
Prognostic models
In order to generate the new metric, logistic regression models were used in the development dataset to calculate the conditional probability of death for each combination of age and GCS score. These probabilities were used to develop a point-based system to allocate risk for mortality. Specifically, the conditional probability of death for the group with the lowest risk (GCS score 15, ages 10–19) was identified as our reference group and assigned a point of 1. An age-specific and GCS-specific point-based system was created by taking the conditional probability for each age and GCS category combination and dividing it by the conditional probability of the reference group. We subsequently created three risk categories (low, moderate, and high) using these points based on thresholds that mirrored the distribution of the original GCS categories (eg, mild GCS (scores 13–15) represent 23% of possible GCS scores; the lowest 23% of points made up the new mild risk GCS category).
Logistic regression models were then constructed using the validation set to compare the predictive performance of the revised GCS categories with the standard GCS categories. The primary set of models were used to compare the discrimination between GCS categories for overall mortality. Second, logistic regression models were used to compare discrimination between GCS categories (standard vs revised) for mortality in each pre-specified subpopulation. Third, logistic regression models were used to compare the discrimination between GCS categories (standard vs revised) for neurosurgical intervention and an unfavorable discharge disposition.
Analysis
Data were analyzed with SAS V.9.4. A conservative p value <0.01 was selected for statistical significance due to the large size of the dataset. Descriptive statistics were used to evaluate differences in variable distributions between the development and test datasets. Model discrimination was examined from the logistic regression models using the area under the receiver operator characteristic (AUROC) curves.
Results
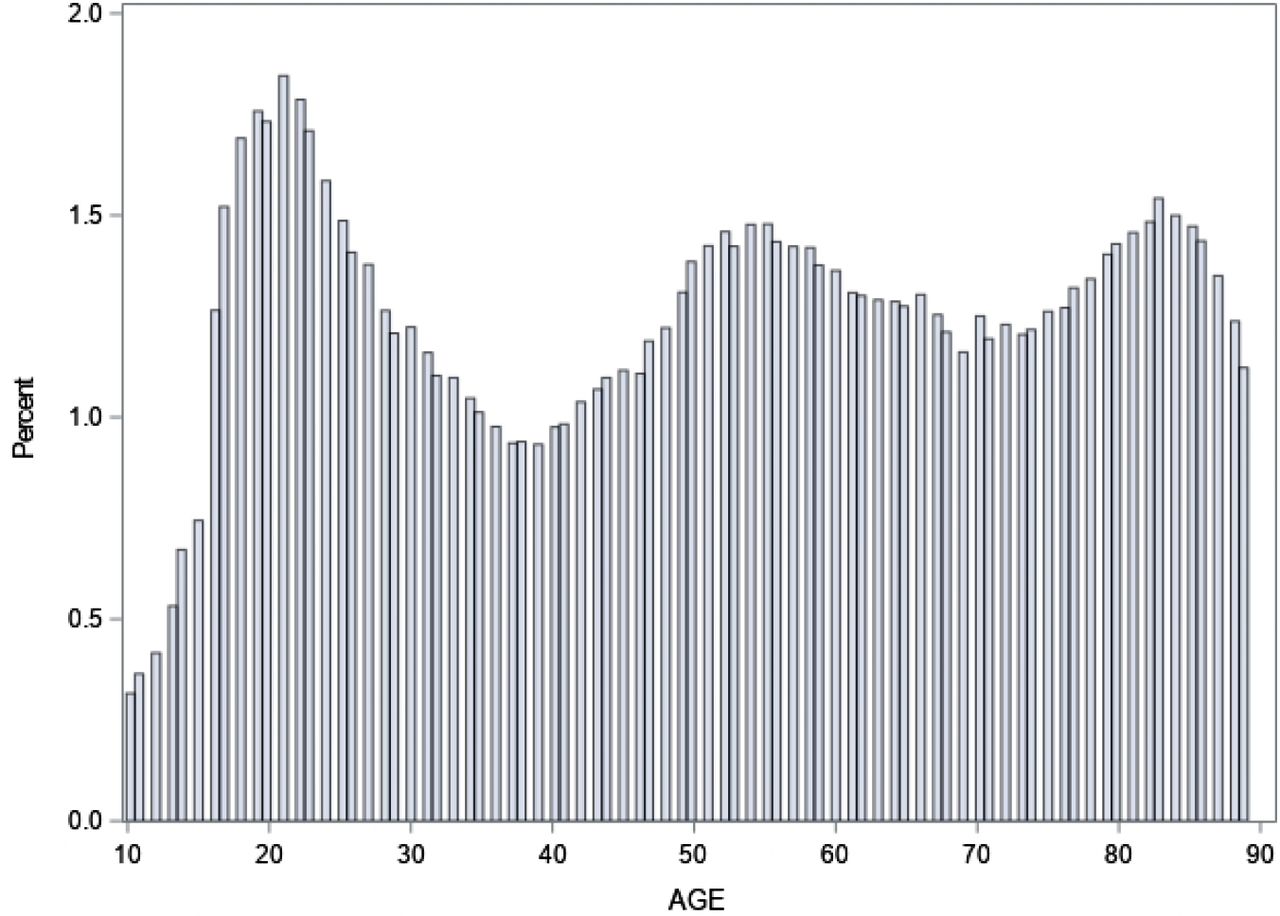
The final population of 539,032 patients with TBI was randomized into a development set (n=403,948) and a validation set (n=135,084). The development and validation datasets were similar across dependent and independent variables: age decade (p=0.67), ED GCS score (p=0.85), mortality (p=0.30), unfavorable disposition (p=0.98), and neurosurgical intervention (p=0.98). The age distribution of the final population with TBI was trimodal, with the largest mode at age 21 (figure 1).

Age distribution of 539,032 patients with traumatic brain injury, ages 10–89.
The percent mortality conditional on age and GCS score is shown in table 1. Within each age decade, the risk of mortality was greatest in patients with GCS 3 and decreased as the GCS score increased (improved). Likewise, within each GCS score, the risk of mortality was greatest in patients in their 80s and decreased as the patient’s age decreased. Points were assigned to each combination of age and GCS score using the baseline risk of mortality (0.31%, teens with GCS 15). Points were categorized into the following groups: 1–10 (low risk (mild)), points 11–35 (moderate risk (moderate)), and points >35 (high risk (severe)).
Conditional probability of in-hospital mortality (%) by age and ED GCS score—development set
The revised GCS risk categories are shown in table 2. For patients in their 50s, the revised GCS categories of high, moderate, and low (3–8, 9–12, 13–15) mirrored the standard GCS categorization of mild, moderate, and severe TBI. All other revised GCS categories were heavily modified by age, and each age decade resulted in a different categorization, except for patients in their 20s and 30s (who were combined). The revised GCS categories shifted incrementally with increasing decade such that the youngest patients had the narrowest definition of high risk (GCS 3–5) and the widest definition of low risk (GCS 10–15), and the oldest patients had the widest definition of high risk (GCS 3–13) and the narrowest definition of low risk (GCS 15).
Revised GCS risk categories for mortality based on age
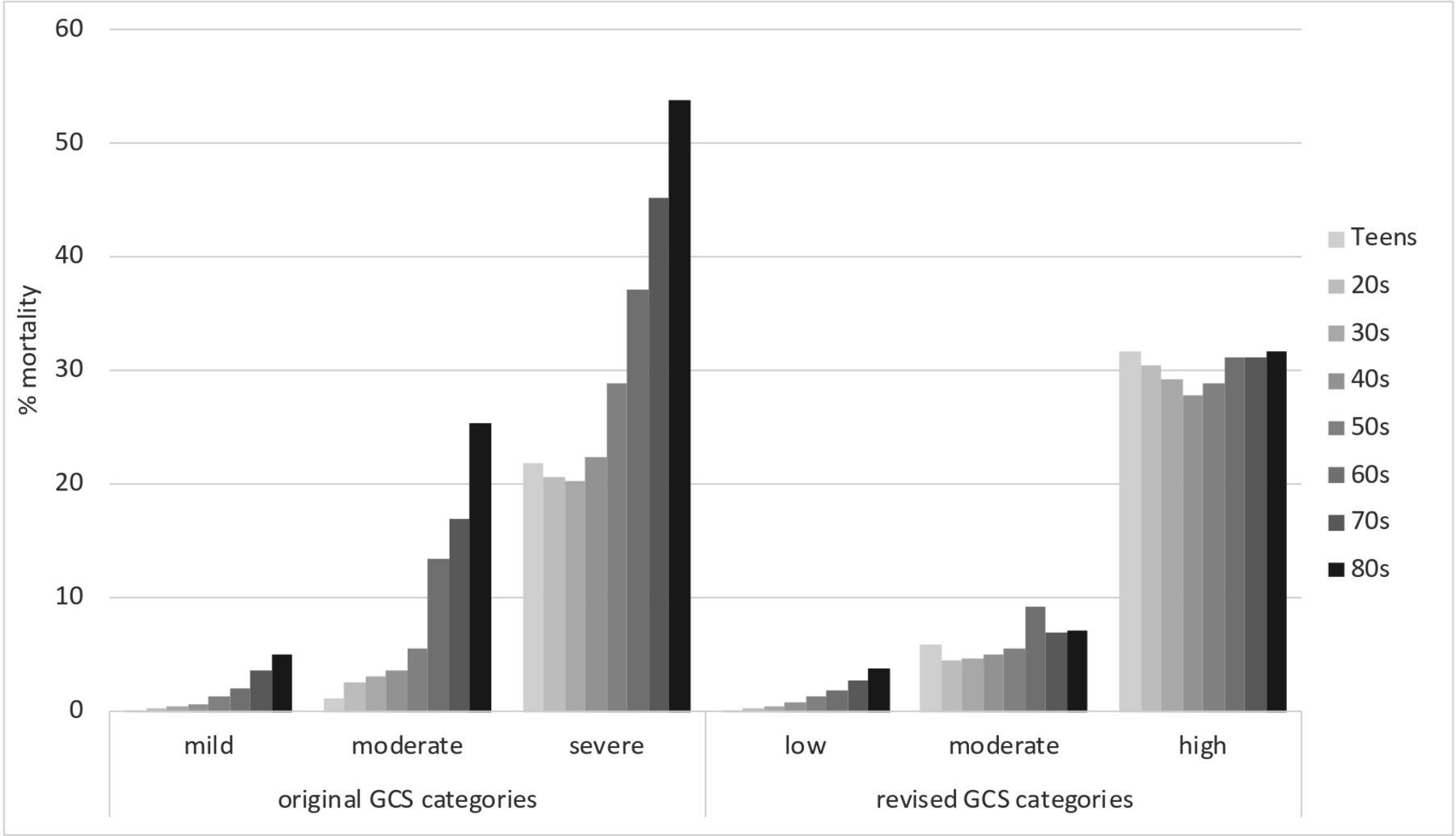
As shown in figure 2, there was a uniform risk of mortality across age decade when using the revised GCS categorization compared with the standard GCS categories. Notably, patients with a severe TBI based on the standard categories (GCS 3–8) had an overall risk of mortality of 29%, but there was a high degree of variability in mortality by age—approximately 20% for the youngest patients but greater than 50% for octogenarians. On the contrary, the revised categorization of high-risk (severe) TBI resulted in a consistent mortality prognosis across age groups of approximately 30%.

{kind=link}
{kind=link}
Percent mortality by age decade and Glasgow Coma Scale (GCS) risk category.
The ROC curves for the standard vs the revised GCS categories are presented in table 3. The revised GCS categories provided significantly better discrimination for mortality than the standard GCS categories (c-statistic: 0.800 vs 0.755, p<0.001).
AUROC for outcomes using standard and revised GCS risk categories—validation set
In the second set of models, we compared the discrimination for mortality within various subsets. The revised GCS categories significantly outperformed the standard GCS categories for patients without extracranial injuries, patients who were not transferred from an outside facility, patients with a blunt mechanism, and patients with fall as a cause of injury (table 3). Patients who were injured from a fall are typically older; this subgroup had the numerically largest improvement in mortality prediction using the revised GCS categories than the standard GCS categories. The only subset that did not show a significant improvement in mortality prediction were patients with a penetrating injury.
In the third set of models (table 3), the revised GCS categories also provided significantly better discrimination for neurosurgical intervention (0.657 vs 0.645, p<0.001) and unfavorable discharge disposition (0.648 vs 0.589, p<0.001) than the standard GCS categories.
Revision of the GCS categories affected 10.12% of all patients and affected older patients more than younger patients (table 4). Approximately 25% of all patients in their 70s and 80s had a revision in their GCS category, whereas approximately 6% of patients in their teens, 20s, and 30s were affected by the revision to the GCS category.
Percentage of patients whose revised GCS category differed from the standard GCS category, by age decile—validation set
Discussion
The GCS score has been adapted into categories of severity and are ubiquitous in the trauma setting and trauma treatment guidelines.5 17–19 In the standard GCS categorization, all patients are classified as a severe TBI based on GCS 3–8, moderate based on GCS 9–12, and mild based on GCS 13–15. The usage of GCS scores of 3 to 8 to denote severe TBI is simple to recall, but this categorization scheme assumes that all patients with GCS 3–8 fall into the same TBI severity regardless of age; this convention appears to be inappropriate. In this study of over half a million patients with TBI, we identified a significant interaction between GCS score and age for mortality following TBI and created revised GCS categories that account for the variability in prognosis by age. We propose that these revised categories will improve severity assessment and early prognosis of TBI based on the initial GCS score.
Our study objective was to create a straightforward revision of the GCS to take into account an age interaction. While these findings may be intuitive, the GCS has not previously been objectively recalibrated for this reason. The predictive performance of the revised GCS categories compared with the standard GCS categories, as measured by the AUROC, was statistically significantly improved. This study did not address whether this effect size is clinically meaningful; we suspect there exists a threshold to which the predictive performance of the GCS can increase because it is an imperfect predictor of mortality. Other studies have recognized the limitations of the GCS score,20–22 especially for risk prognostication.23–26
The majority of the TBI population presented to the ED with GCS scores at the extreme end of the range (GCS 3, GCS 15) where revision of the GCS categories was not affected. The revised GCS had the greatest impact on patients in their 70s and 80s, leading to recategorization of 25% of the population. One likely reason for this finding is that any deviation from a normal (GCS 15) at the initial assessment may be clinically meaningful in an older patient because they are more likely to have cerebral atrophy and occult findings due to blunted or delayed response to injury, or polypharmacy that masks the injury response.27 28 Alternatively, it might suggest their risk of death is not attributable to the TBI, but rather to their pre-injury health and frailty status and lack of compensatory mechanisms.29 30 Regardless of the reason, these insights might allow for more accurate evaluation of an elderly patient’s clinical status, potential outcome, and precise discussion and prognostication with patient’s family.
The revised GCS risk categories have implications for TBI research as part of study/trial selection criteria, as well as adjustment for baseline severity. For research studies or clinical trials of patients with severe TBI (GCS 3–8), younger patients will be disproportionately represented, and older patients will be underrepresented because their GCS scores are typically less severe. The GCS is commonly included in outcome assessment models as a means for adjusting the population based on head injury severity in order to make comparisons between groups of patients, but this adjustment may not lead to a meaningful correction among older patients. Finally, the GCS is used in risk prediction models, such as the revised trauma scale, the trauma injury severity score, and the APACHE II risk scoring systems. We suspect that current risk prediction models might be systematically misclassifying older patients due to reduced validity of the original GCS score over time.
The GCS categories are also used to guide clinical practice. For instance, the Brain Trauma Foundation (BTF) publishes guidelines for the management of severe TBI by synthesizing published studies of patients with GCS 3–8 and then translating the findings into recommendations.31 There already exists age disparities in following BTF guidelines.32 Our findings suggest this age disparity, or systematic bias, might be even more profound because the guidelines are based on a definition of severe TBI using GCS 3–8. Older adults with a true severe TBI may be underrepresented because their presenting ED GCS score may not reflect the severity of their injuries; conversely, younger adults may be overrepresented in severe TBI management guidelines, in that their TBI does not result in neurosurgical intervention or poor morbidity or mortality.
In selecting our study population, we excluded patients who were sedated, intubated, or chemically paralyzed at the time of their ED GCS assessment to improve accuracy, but this resulted in exclusion of a quarter (24.6%) of the TBI population. We performed a sensitivity analysis to test whether the results held true when this population was included in the development of the recalibrated GCS and examined in the validation dataset (online supplemental table 1). The majority of patients who were sedated, intubated, or chemically paralyzed presented to the ED with a GCS 3 but also had elevated mortality and were therefore properly categorized in the high-risk category, resulting in minimal change to the overall revised GCS categorization. The sensitivity analysis demonstrated that the revised GCS categories still provided significantly better discrimination for mortality than the standard GCS categories (c-statistic: 0.845 vs 0.822, p<0.001). Including these patients did not affect the results; still, we excluded them from the final analysis population for accuracy.
Supplemental material
This study has limitations. First, the GCS has undergone minimal change since its creation in 1974. However, the GCS40 is an updated version of the GCS that incorporates a pupillary reactivity score that is subtracted (−2 when both pupils are unreactive), resulting in GCS40 scores ranging from 1 to 15. The GCS40 has been incorporated into the NTDB since 2019; additional validation (or recalibration) of the GCS categories will be required. Second, our findings are not meant to recommend changes to hospital protocols or algorithms, but to provide an effective way to convey mortality risk from TBI based on two major prognostic indicators: age and GCS score. We hypothesize that incorporation of the revised GCS categories into hospital guidelines may have an effect on outcomes, but this research needs to be conducted. Third, we used older NTDB data (admission year 2010–2015) for the analysis for consistency; the NTDB is currently updated through 2017, but the international classification of diseases changed from version ICD-9 to ICD-10 at the end of 2015. Fourth, the AIS is not a mandatory variable in the NTDB and was only documented for 17% of the population, which limited our ability to examine patients with isolated TBI and, conversely, patients with extracranial injuries. Fifth, we do not know the cause of death and if it was TBI related, nor do we know whether an unfavorable discharge destination was due to the TBI or an extracranial injury such as an orthopedic injury. Finally, the NTDB is a convenience sample of patients from over 400 trauma centers and is not nationally representative, as trauma patients treated at non-trauma community hospitals will be underrepresented and patients treated at children’s hospitals may be overrepresented.33
Conclusion
The GCS and its severity categorization (mild, moderate, severe) has become an integral tool for clinical practice and research worldwide, especially in patients with TBI. Although the GCS is used for TBI for severity and prognosis, it was originally intended to communicate a patient’s neurologic status. Prior to its creation, there was no objective way to convey impaired consciousness aside from using descriptors such as ‘obtunded’ and ‘unresponsive’. We do not debate the utility of the GCS in clinical practice; rather, we want to reinforce that the GCS is a clinical tool first and foremost. However, this analysis of the NTDB of over half a million patients with TBI suggests it may be time to modify the GCS severity categorization definitions of mild, moderate, and severe because, as we age, the GCS does not accurately recognize the severity of TBI. We set out to identify whether the definitions of mild/moderate/severe GCS can be significantly improved with a simple recalibration by incorporating the interaction with age. Our age-adjusted GCS categorization of low, moderate, and high risk provides significantly better discrimination for severity of TBI as assessed by mortality, as well as for neurosurgical intervention and unfavorable hospital discharge disposition. This revision of the GCS categories may help eliminate confusion and improve communication for TBI severity and prognostic risk, particularly among older adults.
Acknowledgments
We are grateful to Richard Calvo, PhD for statistical consulting.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KS conceived the study. KS and DB-O designed the study. KS performed data analysis and RP, RMM, and DB-O contributed to data analysis. LD, KLB, DH and WR provided interpretation of the data. KS drafted the manuscript. RP, LD, RMM, KLB, DH, WR, and DB-O provided critical revisions, administrative support, and final approval of the submitted manuscript.
Funding Internal funding provided by Swedish Medical Center, St. Anthony Hospital, Medical City Plano, Penrose-St. Francis Medical Center, Wesley Medical Center, and Research Medical Center Kansas City.
Disclaimer The American College of Surgeons is not responsible for any claims arising from works based on the original data, text, tables, or figures.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study did not require IRB approval because the analysis of secondary, de-identified, publicly available data does not constitute research involving human subjects under the federal Common Rule, 45 CFR Part 46.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. The datasets used and/or analyzed during the current study are publicly available. The NTDB remains the full and exclusive copyrighted property of the American College of Surgeons.