Article Text

Abstract
Background Post-traumatic stress disorder (PTSD) has debilitating psychiatric and medical consequences. The purpose of this study was to identify whether PTSD diagnosis and PTSD symptom scale score (PTSD severity) could be predicted by assessing peritraumatic experiences using a single question or screening tools at different time points in patients hospitalized after admission to the hospital after significant physical trauma, but with stable vitals (level II trauma).
Methods Patients completed the ‘initial question’ and the National Stressful Events Survey Acute Stress Disorder Scale (NSESSS) at 3 days to 5 days after trauma (NSESSS-1). The same scale was administered 2 weeks to 4 weeks after trauma (NSESSS-2). The Posttraumatic Stress Disorder Symptoms Scale Interview for DSM-5 (PSSI-5) was administered 2 months after trauma. PTSD diagnosis and PTSD severity were extracted from the PSSI-5. Linear multivariate regression analyses were used to establish whether scores for NSESSS-1 or NSESSS-2 predicted PTSD diagnosis/PTSD severity. Non-linear multivariate regression analyses were performed to better understand the relationship between NSESSS-1/NSESSS-2 and PTSD diagnosis/PTSD severity.
Results A single question assessing the experience of fear, helplessness, or horror was not an effective tool for determining the diagnosis of PTSD (p=0.114) but can be a predictor of PTSD severity (p=0.039). We demonstrate that administering the NSESSS after either 3 days to 5 days (p=0.008, p<0.001) or 2 weeks to 4 weeks (p=0.039; p<0.001) can predict the diagnosis of PTSD and PTSD severity. Scoring an NSESSS above 14/28 (50%) increases the chance of experiencing a higher PTSD severity substantially and linearly.
Discussion Our initial question was not an effective predictor of PTSD diagnosis. However, using the NSESSS at both 3 days to 5 days and 2 weeks to 4 weeks after trauma is an effective method for predicting PTSD diagnosis and PTSD severity. Additionally, we show that patients who score higher than 14 on the NSESSS for acute stress symptoms may need closer follow-up.
Level of evidence Level III, prognostic.
- stress disorders
- post-traumatic
- diagnosis
- accidents
- mental disorders
Data availability statement
Data are available upon reasonable request. The deidentified participant data (including demographics, scores on the screening questionnaires, and the original screening questionnaires) are available from Dr Yvette Smolin by contacting Yvette.Smolin@wmchealth.org.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Post-traumatic stress disorder (PTSD) is a complex psychiatric disorder. Fortunately, not everyone with exposure to a traumatic experience develops PTSD. Within the general population, there is a 1 year prevalence between 3% and 4.7%.1 2 This prevalence increases to 17.5% to 42% in persons who incur physical trauma 1 month to 6 months after injury.3 PTSD exacerbates underlying medical comorbidities and subsequently increases the risk of death.4 5 Work impairment translates into an estimated annual productivity loss in excess of $3 billion.6 Only 9.8% of individuals diagnosed with PTSD received treatment.7
To qualify for the diagnosis of PTSD according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), subjects must be exposed to a trauma, and exhibit several symptom criteria (figure 1). If they exhibit these symptoms for less than 1-month duration, then the diagnosis becomes acute stress disorder (ASD).8 The diagnosis of full criteria of ASD has been shown to be correlated with the diagnosis of PTSD.9

Post-traumatic stress disorder diagnostic criteria.
The purpose of this study was to identify whether the diagnosis of PTSD and PTSD symptom severity could be predicted by assessing peritraumatic experiences using a single question and/or a short screening tool. Prior studies have shown that peri-traumatic emotional factors such as fear, helplessness, and horror at the time of trauma can be an effective predictor of PTSD.10–12 The single question asked hospitalized level II trauma patients to rate their experience of fear, helplessness, or horror 3 days to 5 days after the trauma. We also evaluated whether the severity of ASD symptoms 3 days to 5 days after the trauma or the severity of ASD symptoms 2 weeks to 4 weeks after the trauma could be used to predict PTSD diagnosis and PTSD symptom severity.
Patients and methods
Design and procedures
The study was approved by the New York Medical College Institutional Review Board and Clinical Research Institute of Westchester Medical Center (WMC). WMC is a quaternary care medical center that serves a large catchment area and is an American College of Surgeons Verified Level I Trauma Center. Within our institution’s protocols, patients are classified as level II trauma that consider mechanistic, physiological, and anatomic criteria, as well as clinician judgment as detailed in online supplemental figure 1.13 14 Level I trauma activations represent the highest level of activation with respect to resources and urgency. Level I trauma activation patients are critically ill, often to the extent of functional dependence among survivors. Our selection criteria focused on trauma patients admitted after level II trauma activation, because we chose to study injured but physiologically normal patients that could (1) consent to be included in the study and (2) could have maximized opportunity to participate in both the initial and follow-up screening tools without the confounding element of injury patterns rendering subjects with an inability to participate or complete the study.
Supplemental material
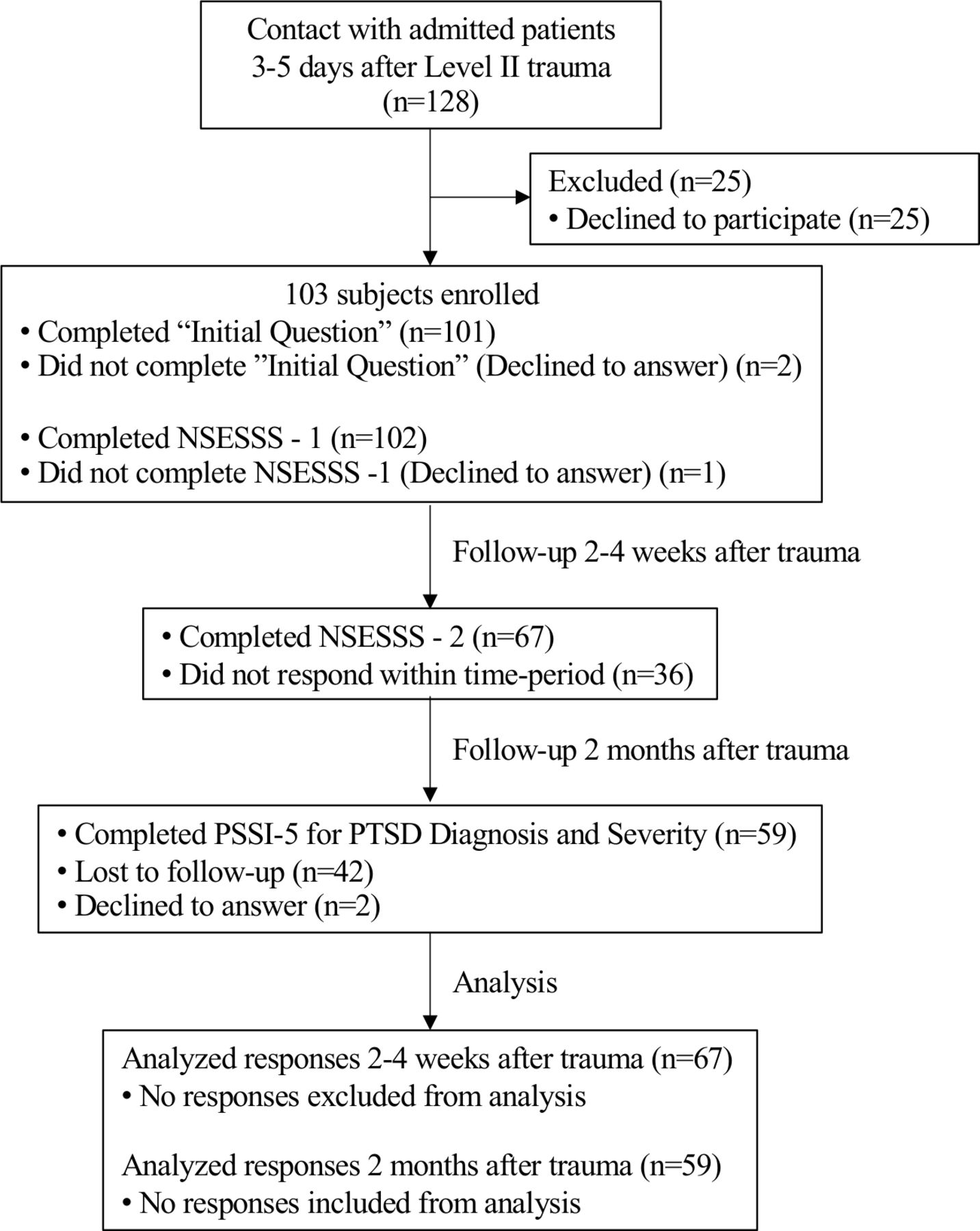
Level II trauma patients were approached for enrollment in the study 3 days to 5 days after trauma by either of two trained clinicians (SR, senior psychiatry resident, and JV, nurse practitioner). The protocol was fully explained to the subjects and their written informed consent was obtained. The subjects completed the initial question and the standardized National Stressful Events Survey Acute Stress Disorder Scale (NSESSS) 3 days to 5 days after trauma in person (NSESSS-1), the NSESSS 2 weeks to 4 weeks after trauma by phone (NSESSS-2), and the Post-Traumatic Stress Disorder Symptom Scale Interview for DSM-5 (PSSI-5) 2 months after trauma by phone (see figure 2). The outcomes of PTSD diagnosis and PTSD severity were extracted from the PSSI-5.
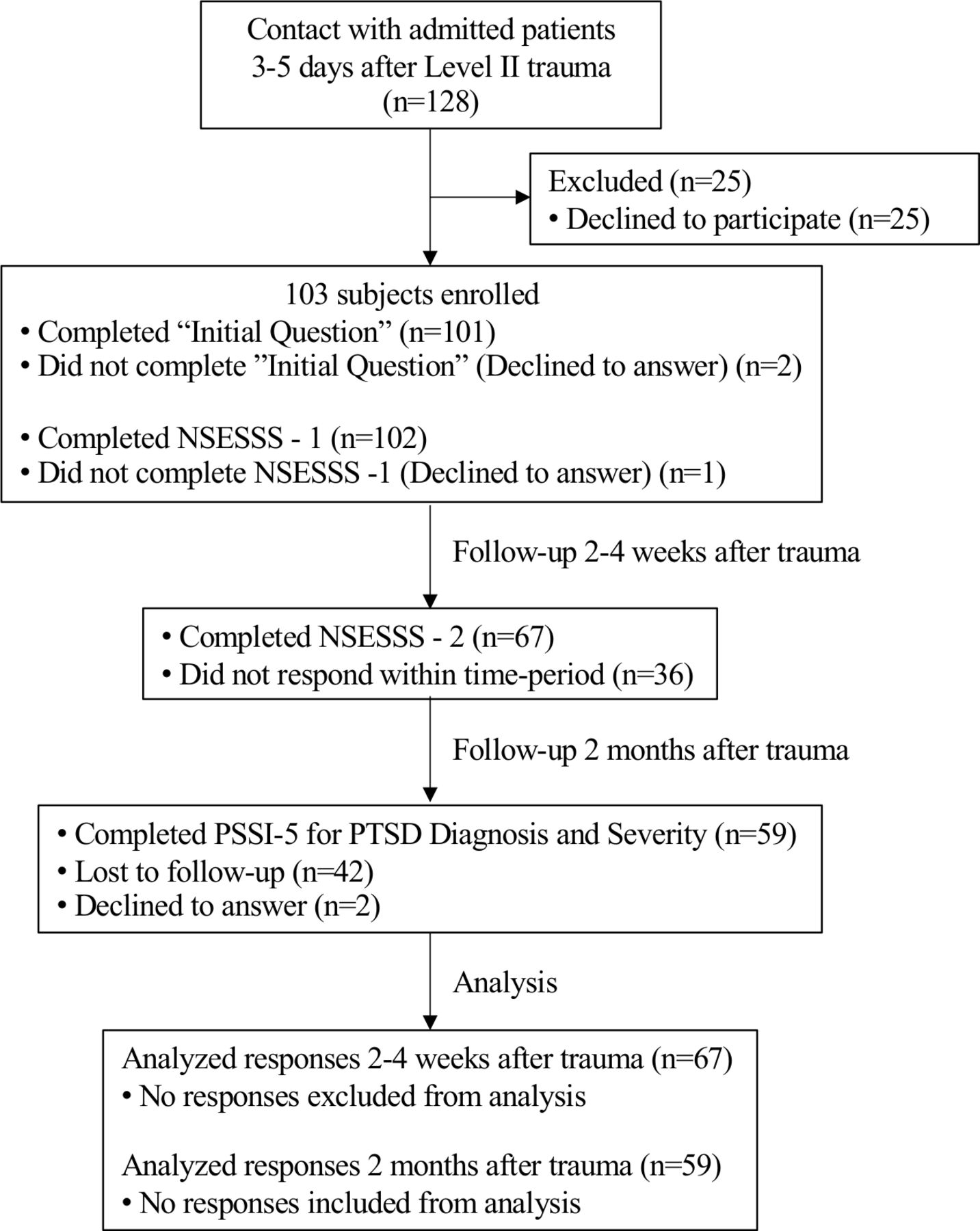
Modified consort flow diagram. NSESS, National Stressful Events Survey Acute Stress Disorder Scale; PSSI-5, Posttraumatic Stress Disorder Symptoms Scale Interview for DSM-5.
Injury Severity Score (ISS) was abstracted from each subject’s chart. The ISS is based on severity score from six regions of the body (head or neck, face, chest, abdominal or pelvic contents, extremities or pelvic girdle, and external).15
Screening tools
The ‘initial question’ asked was ‘To what extend did you feel fear, helplessness, or horror?’ with three possible choices (‘not at all,’ ‘somewhat’, and ‘intensely’). This question was a significant criterion for diagnosis of PTSD in DSM-IV TR and has been removed from DSM-5. The NSESSS for acute stress symptoms (online supplemental figure 2) is a seven-item screener that assesses the severity of symptoms of ASD. Each item on the measure is rated on a 5-point scale (0=not at all, 1=a little bit, 2=moderately, 3=quite a bit, and 4=extremely). The total score ranges from 0 to 28, with higher scores indicating greater severity of ASD. The average score for each subject was used. ASD can be evaluated in terms of none (0), mild (1), moderate (2), severe (3), or extreme (4).16 The PSSI-5 is a 24-item semistructured interview that assesses PTSD symptoms in the past month.17 18 A diagnostic determination of PTSD was made by a clinician if the enrolled patient met the DSM-5 criteria of PTSD on completion of the PSSI-5 (figure 1). The PTSD symptom scale from the PSSI-5 was used to assess the severity of PTSD symptoms. The PSSI-5 instructions indicate that a presumptive diagnosis of PTSD may be made if a patient scores ≥23 on the symptom scale, but there is no available literature confirming this assumption. Symptoms are also rated on a 5-point scale of frequency and severity ranging from 0 (not at all) to 4 (6 or more times a week/severe). The sum of the 20 PTSD symptom items yields a total PTSD symptom scale, which is evaluated as follows: minimal symptoms (0 to 8), mild (9 to 18), moderate (19 to 30), severe (31 to 45), and very severe (46 to 80).
Supplemental material
Subjects
Eligible study subjects were trauma patients meeting level II activation criteria and deemed to be medically stable by an interdisciplinary team of providers. The NSESSS and the PSSI-5 were administered in English. Patients who did not speak English or had a hospital stay of <72 hours were excluded from the study. In addition, vulnerable populations such as pregnant women, prisoners, and persons with decisional incapacity were excluded. Any patients in the hospital who had symptoms of ASD that were causing distress underwent an inpatient psychiatric consultation as per the standard of care. After discharge from the hospital, subjects who had symptoms of PTSD who self-identified as affecting daily living were provided a referral to a mental health clinician in their locale.
Statistical analysis
Descriptive statistics were used to describe demographics. Non-parametric tests were used for data analyses. Statistical analyses were conducted in SPSS V.27 using two-tailed tests with a 0.05 significance level. The general population prevalence of 3.5% 1-year prevalence of PTSD in the general population was used for the expected incidence as the range of injury was unknown at the outset of the study.19 The post hoc power analysis of the study to detect PTSD was 96.3% as the incidence of PTSD in our study group was 16.9% as we ultimately had 59 subjects complete the PSSI-5. Univariable logistic regression was used to assess association of PTSD diagnosis with baseline covariates (age, gender, and ISS) and the scores for the initial question, NSESSS-1, and NSESSS-2. Multivariable logistic regression was used to analyze if the initial question, NSESSS-1, and NSESSS-2 predict PTSD diagnosis. Similarly, multivariable linear regression analyses were used to establish whether scores for the initial question, NSESSS-1, and NSESSS-2 predict the PTSD severity using the PTSD symptom scale. In addition, using a generalized additive model (GAM), a non-linear multivariable regression analysis was performed to gain a better understanding of the relationship between NSESSS-1 and PTSD severity, as well as NSESSS-2 and PTSD severity.
Results
A total of 1633 level II trauma activations occurred at WMC during the time period of this study. A total of 1183 activations had an associated ISS available in the trauma registry. A total of 103 subjects were enrolled in the study (figure 2). The mean (±SD) of the age of enrolled subjects was 55 (±22.4) years. Although <10% of the eligible patients enrolled in the study, table 1 demonstrates that there were no appreciable differences in gender, age, or ISS between those enrolled, who completed the PSSI-5, and in all level II trauma activations who had an ISS completed.
Demographics
Of the study sample, 63.1% were male. Of the 103 enrolled subjects, 101 completed the initial question: 28.2% responded ‘not at all’; 25.2% responded ‘somewhat,’ and 44.7% responded ‘Intensely.’ NSESSS-1 was completed at the same time as the initial question. Of the 103 subjects, 102 completed NSESSS-1. Sixty-seven of the 103 subjects completed NSESSS-2. Forty-five of the 103 subjects completed NSESSS-2 and PSSI-5. Ffty-nine of the 103 subjects completed PSSI-5 (figure 2). These subjects also completed the initial question and NSESSS-1. None of the results showed a normal distribution of values. Of the 59 (16.9%) subjects, 10 met the criteria for the diagnosis of PTSD. Twenty-five subjects refused to participate after the study was explained to them. Enrolled subjects had a mean (±SD) ISS of 11.68 (±6.83), similar to subjects who refused to enroll (10.95 (±7.30)). Age, gender, and ISS did not show a significant association in any model with either the diagnosis of PTSD or the PTSD severity using the PTSD symptom scale. None of the enrolled subjects had a documented prior diagnosis of PTSD.
Administering question 1 after 3days to 5 days was not a predictor for the diagnosis of PTSD in either the univariable or multivariable model (table 2). However, answers to the initial question were predictive of the PTSD severity based on the PTSD symptom scale (p=0.039) (table 3). In contrast, PTSD diagnosis was predicted by NSESSS-1 (p=0.008) (table 2). PTSD severity using the PTSD symptom scale was also predicted by NSESSS-1 (p<0.001) (table 3). PTSD diagnosis was predicted by NSESSS-2 (p=0.039) (table 2). PTSD severity was also predicted by NSESSS-2 (p<0.001) (table 3).
Ability of screening tools to predict PTSD diagnosis
Ability of screening tools to predict PTSD symptom scale (severity)
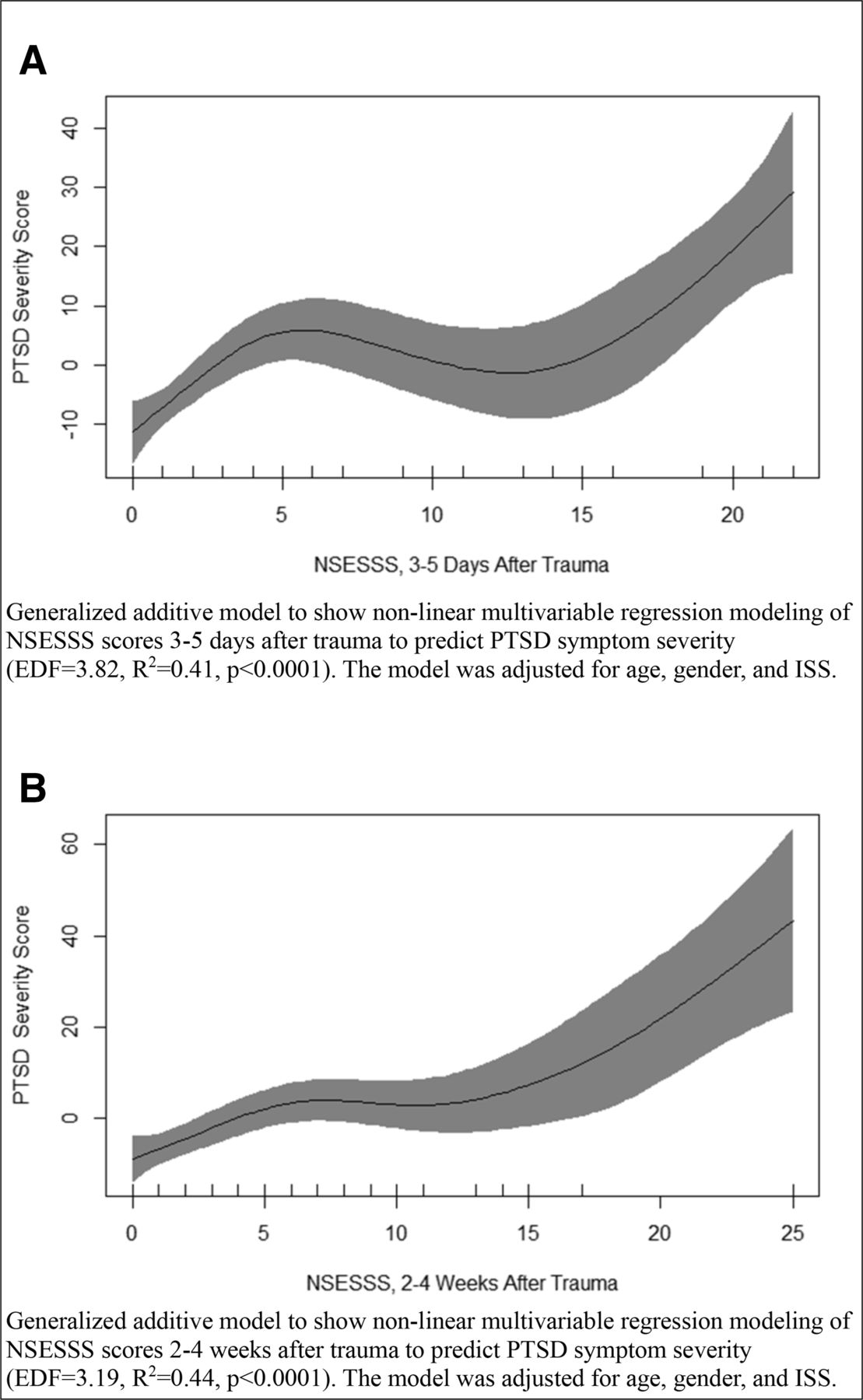
Non-linear multivariable regression analysis by GAM showed significant association (p<0.001) between NSESSS-1 scores and severity on the PTSD severity, and a significant association (p<0.001) between NSESSS-2 and PTSD severity. Of interest, non-linear multivariable regression analysis indicated that the likelihood of PTSD diagnosis increased significantly after a subject scored more than 14/28 (>50%) on the NSESSS at both 3 days to 5 days and 2 weeks to 4 weeks after trauma. Every average point increase in the average NSESSS score after 2 weeks to 4 weeks showed an increase by 10 points in PTSD symptom scale. This relationship is presented in figure 3A,B.
{kind=link}
{kind=link}
{kind=link}
Non-linear multivariable regression modeling. ISS, Injury Severity Score; NSESSS, National Stressful Events Survey Acute Stress Disorder Scale; PTSD, post-traumatic stress disorder EDF, estimated degrees of freedom.
Discussion
A recent study has shown that only 7% of adult Level-1 trauma centers20 and 36.17% of pediatric trauma centers had a protocol for assessing PTSD; 12.5% of Level I adult centers and 27.66% of pediatric trauma centers had an assessment protocol for ASD.21 In this study, we found 4 x as many subjects (16.9%) qualified for a diagnosis of PTSD compared with the 1 year prevalence for PTSD (3.5%) in the general population, and almost 1.5 x higher than what has previously been reported among trauma patients.1 2 Individuals who were hospitalized after a trauma are at a significantly elevated risk for developing PTSD compared with the general population. As such, it is important to screen this population for developing PTSD. Of note, we found that ISS was not a predictor for PTSD for patients who are hospitalized after a level II trauma. This is consistent with previous literature that has shown that ISS is not a predictor for PTSD or PTSD severity.22 23 It should be noted that ISS is primarily a marker of injury severity in blunt trauma (as that suffered by our study sample). This finding may not be replicated when working with ISS in patients who have penetrating trauma.
Our findings indicate that although using a simple screening question assessing the experience of fear, helplessness, or horror predicted PTSD severity, it was not effective for predicting PTSD diagnosis. Administering a multifaceted screening tool such as the NSESSS at either 3 days to 5 days or 2 weeks to 4 weeks after the trauma was an effective predictor for both the diagnosis of PTSD and PTSD severity. This suggested that there is utility in administering the NSESSS for trauma patients who were admitted to the hospital as early as 3 days to 5 days after their trauma. To our knowledge, this is the first study that demonstrates a relationship between NSESSS scores and PTSD severity. Using a simple linear regression, we saw that for every average point increase in the average NSESSS score at 3 days to 5 days, we see an increase in PTSD symptom scale score by 8 points. Similarly, every average point increase in the average NSESSS score after 2–4 weeks showed an increase by 10 points in the PTSD symptom scale score.
The current study evaluated the relationship between NSESSS and PTSD severity. We demonstrated that if a subject scores below 14 on the NSESSS at either 3 days to 5 days or 2 weeks to 4 weeks after the trauma, then there would be a low chance to experience greater PTSD severity after 2 months. However, if they scored above 14 on the NSESSS at either 3 days to 5 days after trauma or 2 weeks to 4 weeks after trauma, then the chance of experiencing greater PTSD severity would increase substantially and linearly. As such, it may be beneficial to pre-emptively establish outpatient psychiatric follow-up for individuals who score more than 14 on the NSESSS for acute stress symptoms.
This study not only highlighted the fact that level II trauma patients were at an increased risk of PTSD but also established that the diagnosis and severity of PTSD can be predicted with the use of a simple screener in this population at an early stage of the hospital course. We successfully identified an early time frame for administering the NSESSS, established the utility of using the NSESSS for ASD to predict PTSD diagnosis and severity, and found a threshold for establishing outpatient care to help improve the quality of life of these patients.
Prior studies have demonstrated that PTSD diagnosis can be predicted after injury using different screeners such as the Injured Trauma Survivor Screen (9-item), Posttraumatic Stress Disorder Checklist for DSM-5 (20-item), and Posttraumatic Adjustment Scale (10-item).24–26 We chose to use the NSESSS as not only did it have a shorter screener with only seven items but also it validated to assess severity of symptoms. Our study is unique in comparison to previous studies as none of the prior studies assessed for predicting symptom severity.
As screening for substance abuse has become standard practice among trauma centers, this study suggests screening for PTSD should also become routine practice for all systems of trauma-related patient care. Given both the ease and predictive power of PTSD screening as demonstrated in our study, we suggest the development of both institutional and societal guidelines where all trauma patients should undergo screening as part of the multidisciplinary care that trauma patients are expected to receive. Incorporating PTSD screening as standard trauma care will allow for earlier diagnosis with minimal additional requirements for healthcare resources. In turn, this will lead to earlier opportunities for interventions that may significantly improve quality of life and reduce morbidity. There remain multiple systemic barriers in obtaining quality long-term outpatient mental healthcare, particularly for individuals without insurance. Earlier and more effective identification of PTSD in the civilian population may alert policymakers and healthcare systems to the unrealized demand for mental health resources.
Limitations
As with most longitudinal studies, this analysis was hampered by difficulty with follow-up as less than half of the enrolled subjects completed all three screeners. Another limitation was that factors that have been found to be associated with PTSD such as prior psychiatric diagnoses (including prior history of PTSD), socioeconomic status, childhood abuse, anxiety, or substance use were not ascertained through a psychiatric history at the time of administering the screener.27–29 The effect of injury mechanism, particularly penetrating trauma and traumatic brain injuries has been correlated with the development of PTSD.30 Both of these groups were under-represented in our sample population.⇓ Although assessing the effect of injury mechanism and functional status of the patient is outside the scope of this study, these are important factors that have been correlated with the development of PTSD.31 This study is limited in its scope in that it focuses on level II trauma patients who were hospitalized. It would be instrumental to see whether these results could be replicated in Level I trauma patients who are more likely to suffer from greater injury severity, a traumatic brain injury, gun-shot wounds, and penetrating trauma, and are more likely to suffer medical trauma. We did not conduct psychiatric evaluations after discharge and did not assess the development of affective disorders, but this may be appropriate for future investigations. It would be equally important to assess trauma patients who were discharged directly from the emergency department and, to broaden the study, to include all trauma patients regardless of activation level using a similar protocol.
Conclusions
We demonstrate a higher prevalence of PTSD in hospitalized trauma patients than in the general population, suggesting increased screening for PTSD among this patient population. We confirm that ISS is not predictive of PTSD diagnosis or severity. Using a simple, but multifaceted, screener such as the NSESSS as a screener at either 3 days to 5 days or 2 weeks to 4 weeks after the trauma is an effective method for predicting the diagnosis and the severity of PTSD symptoms. In addition, we show that patients who score higher than 14 on the NSESSS for Acute Stress Symptoms may need closer follow-up.
Data availability statement
Data are available upon reasonable request. The deidentified participant data (including demographics, scores on the screening questionnaires, and the original screening questionnaires) are available from Dr Yvette Smolin by contacting Yvette.Smolin@wmchealth.org.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the New York Medical College Institutional Review Board and the Clinical Research Institute of Westchester Medical Center (approval ID: L12004). Written informed consent was obtained for all subjects before taking part in the study.
Acknowledgments
The authors thank Rida Khan.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JV, MK, YS, and RD designed the study. JV and SR participated in enrollment and data collection. SR, JV, MF, RD, AS, KP, PR and YS participated in data analysis and interpretation. All authors read and approved the final submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.