Article Text

Abstract
Background Trauma elicits a complex inflammatory response that, among multiple presenting factors, is greatly impacted by the magnitude of injury severity. Herein, we compared the changes in circulating levels of mediators with known proinflammatory roles to those with known protective/reparative actions as a function of injury severity in injured humans.
Methods Clinical and biobank data were obtained from 472 (trauma database-1 (TD-1), University of Pittsburgh) and 89 (trauma database-2 (TD-2), Indiana University) trauma patients admitted to the intensive care unit (ICU) and who survived to discharge. Injury severity was estimated based on the Injury Severity Score (ISS), and this was used as both a continuous variable and for the purpose of grouping patients into severity-based cohorts. Samples within the first 24 hours were obtained from all patients and then daily up to day 7 postinjury in TD-1. Sixteen cytokines were assayed using Luminex and were analyzed using two-way analysis of variance (p<0.05).
Results Patients with higher ISSs had longer ICU and hospital stays, days on mechanical ventilation and higher rates of nosocomial infection when compared with the mild and moderate groups. Time course analysis and correlations with ISS showed that 11 inflammatory mediators correlated positively with injury severity, consistent with previous reports. However, five mediators (interleukin (IL)-9, IL-21, IL-22, IL-23 and IL-17E/25) were suppressed in patients with high ISS and inversely correlated with ISS.
Discussion These findings suggest that severe injury is associated with a suppression of a subset of cytokines known to be involved in tissue protection and regeneration (IL-9, IL-22 and IL-17E/25) and lymphocyte differentiation (IL-21 and IL-23), which in turn correlates with adverse clinical outcomes. Thus, patterns of proinflammatory versus protective/reparative mediators diverge with increasing ISS.
- accidents
- cytokines
- intensive care units
- inflammation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Among the multiple intrinsic and extrinsic factors that contribute to trauma patient morbidity and mortality is the dysregulated immune response that often follows severe injury.1 2 Although injured tissues release endogenous molecules such as damage-associated molecular patterns, chemokines and cytokines to mobilize immune defenses and to promote tissue repair, an insufficient or overly exuberant inflammatory response can lead to further damage.3 4 The ensuing trauma-induced inflammatory response varies not only by type and severity but also by individual variables such as age, sex, genetics and combinations thereof.5 6 Nevertheless, among all these presenting factors, the magnitude of injury severity which is often accompanied by physiological and metabolic derangement can greatly impact the ensuing inflammatory response.2 Estimation of trauma severity currently relies on clinical diagnoses and scoring systems, among which the Injury Severity Score (ISS) is the most widely used to predict clinical outcomes and mortality after traumatic injury.7 We have previously shown, using highly matched cohorts of trauma patients that a series of circulating proinflammatory mediators, including interleukin (IL)-6, IL-8, IL-10 and monocyte chemotactic protein (MCP)-1/CCL2, significantly and positively correlate with ISS.2 A follow-up study examining levels of soluble suppression of tumorigenicity 2 and its ligand, IL-33, surprisingly showed that IL-33 levels were suppressed in patients that do not survive or survive but have higher ISSs.8 The IL-33 findings were intriguing in that this cytokine can have both inflammatory and reparative functions.9 These findings suggested that levels of all mediators may not simply increase with injury severity, but some with reparative potential could be suppressed.
To address the hypothesis that circulating mediator levels diverge in an injury severity-dependent manner, we analyzed a subset of mediators that included cytokines with known tissue protection and repair properties (IL-9, IL-22 and IL-17E/25) in two previously reported trauma cohorts.4 Our findings indicate that circulating patterns of proinflammatory versus protective/reparative cytokines diverge as injury severity increases. These novel findings provide insights into factors that may drive outcomes and suggest that therapies targeting the immune response after injury may need to be tailored differently based on the degree of injury severity.
Patients and methods
Patient enrollment and sampling
Two separate databases/biobanks were used in this study, including trauma database-1 (TD-1, University of Pittsburgh) and Trauma database-2 (TD-2, Indiana University). Patients eligible for enrollment were victims of blunt trauma, at least 18 years of age and admitted to the intensive care unit (ICU). Exclusion criteria included isolated head injury, pregnancy or expected duration of survival of <24 hours. Three plasma samples, starting with the initial blood draw on arrival to the emergency department (ED) with a median time of 3 hours and 50 min (IQR: 2 hour and 22 min–5 hour and 40 min) from injury to the first blood sample. Blood was collected into citrated tubes via venous or arterial catheters. Additional blood samples were obtained at 24 hours after injury and then daily up to day 7. Blood samples were collected into citrated tubes via venous or arterial catheters and stored at 4°C before being centrifuged within 2 hours of collection. Thereafter, plasma aliquots were stored in cryopreservation tubes at −80°C for subsequent assay of inflammatory mediators.
Data collection
Demographic and clinical data including ICU length of stay (LOS), hospital LOS, days on mechanical ventilation, ISS, the Abbreviated Injury Scale (2005–update 2008 version, where a 0 value was assigned when no injury was present), the Marshall Multiple Organ Dysfunction Score10 was calculated as an index of organ dysfunction using clinical parameters obtained from the inpatient electronic medical record (EMR). This score has six variables, including (1) the respiratory system (PO2/FiO2 ratio); (2) the renal system (serum creatinine concentration); (3) the hepatic system (serum bilirubin concentration); (4) the hematological system (platelet count); (5) the central nervous system (Glasgow Coma Scale) and (6) the cardiovascular system—the pressure-adjusted heart rate, shock index (defined as the ratio of heart rate to the systolic blood pressure, where an index of >1 signifies hypovolemic shock),11 admission values of arterial base deficit (BD) and lactic acid were abstracted from the EMR and the trauma registry database. Nosocomial infection (NI) was defined based on the US Centers for Disease Control clinical criteria using clinical data obtained from the EMR.12
Study design
The derivation cohort consisted of 472 blunt trauma patients admitted or transferred to the ED of the Presbyterian University Hospital (level 1 trauma center) and who survived to hospital discharge; the salient characteristics were described recently.4 The contemporary validation cohort consisted of 89 blunt trauma survivors who were admitted to the ED of the Indiana University Health Methodist Hospital (also a level 1 trauma center). Based on the ISS degree, three ISS-based cohorts were defined: mild ISS, 1–15 (n=180 and n=12); moderate ISS, 16–24 (n=170 and n=21); and severe ISS, ≥25 (n=122 and n=56) in the TD-1 and TD-2 databases, respectively. To determine normal values of circulating inflammation biomarkers, plasma was obtained from 12 healthy volunteers with no history of pre-existing illness (7 men and 5 women; mean age: 43.2±2.6).
Analysis of inflammation biomarkers
Both TD-1 and TD-2 plasma samples were assayed using the human inflammatory MILLIPLEX MAP Human Cytokine/Chemokine Panel-Premixed 26 Plex, MILLIPLEX MAP Human Th17 Panel (Millipore Corporation, Billerica, MA, USA), Luminex 100 IS analyzer (Luminex, Austin, TX, USA) and MAGPIX system (MilliporeSigma, Austin, TX, USA) were used to measure plasma levels of interleukin (IL)−1β, IL-1 receptor antagonist (IL-1RA), soluble IL-2 receptor-α (sIL-2Rα), IL-4, IL-5, IL-6, IL-7, IL-8 (CCL8), IL-9, IL-10, IL-17A, IL-17E/IL-25, IL-21, IL-22, IL-23 and MCP-1 (CCL2). The Luminex system was used in accordance to the manufacturer’s instructions.
Statistical analysis
All data were analyzed using SigmaPlot V.11 software (Systat Software, San Jose, CA, USA), STATA statistical software and GraphPad Prism V.7 (Graphpad Software, San Diego, CA, USA). Statistical comparisons were performed using either Kruskal-Wallis one-way analysis of variance (ANOVA) followed by the Dunn’s post hoc test (for continuous data) or Fisher’s exact test (for categorical data), as appropriate. We note that the assayed inflammatory biomarkers exhibited high patient-to-patient variability in both the TD-1 and TD-2 trauma cohorts due to multiple factors (demographics, illnesses, time and treatments). It is, therefore, very difficult to meet the assumptions of independency, normality and sphericity, unless using an extremely large and controlled (with inclusions and exclusions) sample size. Given these limitations and to overcome the inequality in sample size at these multiple measurement points (due to dropout of some patients (discharge) as we go further in hospitalization time), we used Friedman two-way ANOVA on ranks (p<0.05) to evaluate the group–time interaction of plasma inflammatory mediators' levels. Correlation analysis among the inflammatory mediators and ISS are expressed as Spearman correlation coefficients (CCs). A p value of <0.05 (two-sided) was considered statistically significant for all analyses.
Results
Demographics and clinical outcomes of ISS-based groups
TD-1 was composed of 472 trauma survivors and TD-2 included 89 trauma survivors. Patients from each database were segregated into three injury severity-based groups (mild, ISS 1–15; moderate, ISS 16–24; and severe, ISS≥25). The patient distributions across the levels of injury severity and the patient characteristics and outcomes are shown in the table 1. Patients in TD-2 were younger compared with TD-1 in all three ISS groups. Patients with higher ISS had longer ICU LOS, total hospital LOS, longer duration of mechanical ventilation and higher rates of NI in both datasets. Moreover, the severe group had higher rates of disposition to facilities other than home, such as rehabilitation centers and skilled nursing facilities than the other groups. In TD-1, the severe ISS group had statistically significantly higher BD and lactate levels on admission to the ED when compared with the mild and moderate ISS groups. Whereas the difference was not statistically significant in the TD-2 dataset, the severe ISS group similarly exhibited a higher BD and lactate compared with the mild and moderate ISS groups. The degree of shock at admission was assessed by calculating the shock index, which was higher on admission in the highest ISS group in both TD-1 and TD-2. Therefore, as expected, patients in the highest ISS group exhibited the greatest physiological derangement and worst outcomes in both datasets.
Overall demographics, trauma scores, mechanism of injury, clinical outcomes and disposition of the three injury severity groups segregated based on their ISS for the two separate databases used in the study, including TD-1 (University of Pittsburgh) and TD-2 (Indiana University)
Distinct inflammatory patterns emerge among the ISS-based groups
We have previously shown, using highly matched subsets of patients from TD-1, that circulating proinflammatory cytokines and chemokines are higher in patients with greater ISS.2 To characterize an expanded set of mediators across all patients in the TD-1 and TD-2 datasets, we performed non-parametric correlation analysis to examine the associations between different grades of injury severity and levels of 16 plasma inflammatory immune mediators as described in the Patients and methods section. Consistent with our previous work, ISS correlated positively with concentrations of known proinflammatory biomarkers, including IL-6 (CC=0.33, 95% CI 0.27 to 0.39, p<0.001), IL-8 (CC=0.25, 95% CI 0.19 to 0.32, p<0.001), IL-10 (CC=0.19, 95% CI 0.12 to 0.25, p<0.001) and MCP-1 (CC=0.29, 95% CI 0.22 to 0.35, p<0.001) (online supplemental figure 1). In striking contrast, levels of IL-9 (CC=−0.18, 95% CI −0.24 to −0.11, p<0.001), IL-21 (CC=−0.20, 95% CI −0.26 to −0.13, p<0.001), IL-22 (CC=−0.14, 95% CI −0.21 to −0.07, p<0.001), IL-23 (CC=−0.18, 95% CI −0.25 to −0.12, p<0.001) and IL-17E/25 (CC=−0.09, 95% CI −0.16 to −0.02, p=0.008), although elevated above baseline at low ISS, failed to elevate in the circulation in both trauma cohorts at higher ISS (figure 1). Thus, levels of the proinflammatory cytokines and the levels of IL-9, IL-21, IL-22, IL-23 and IL-17E/25 diverge in patients with greater injury severity.
Supplemental material
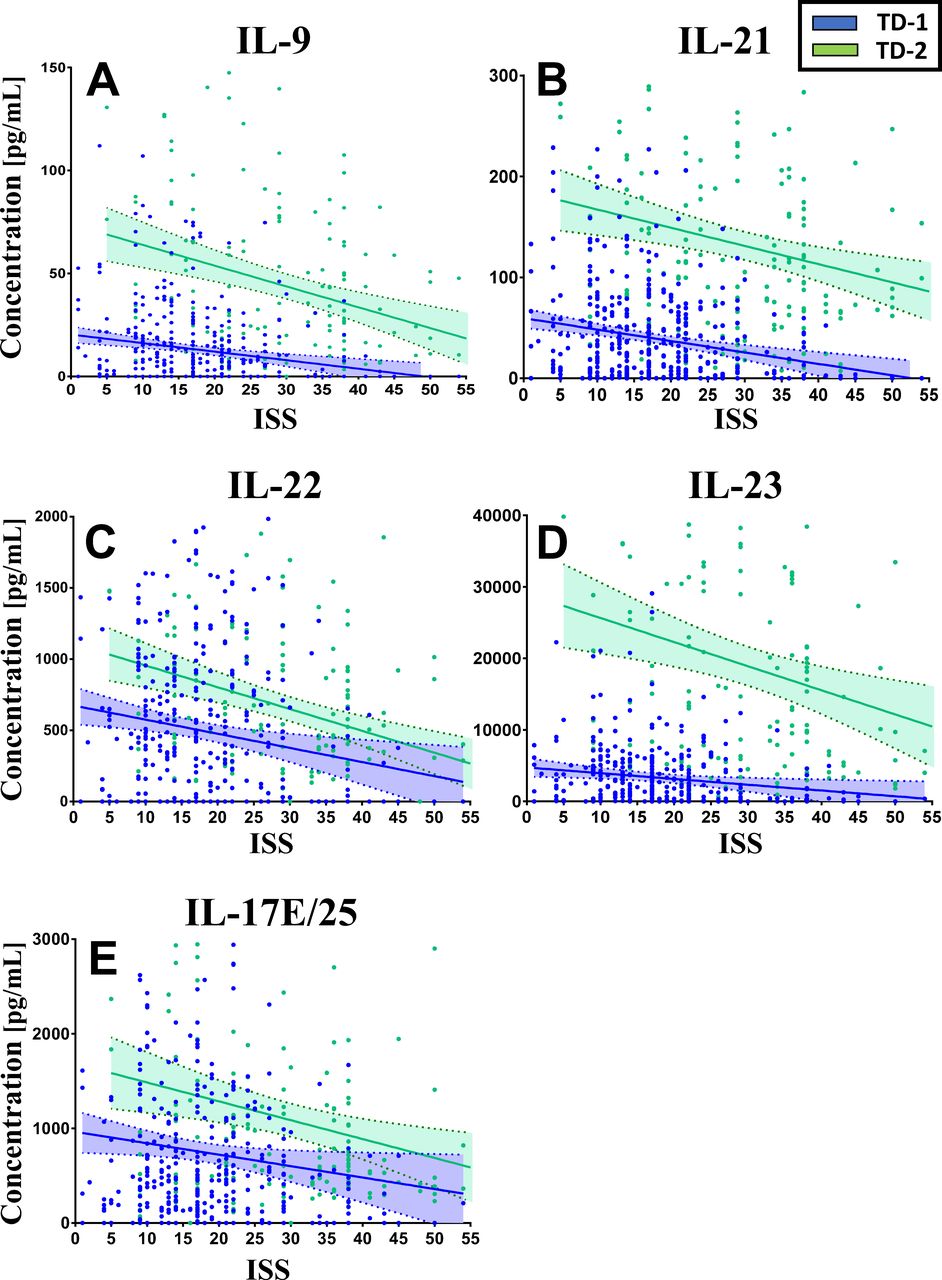
Linear regression of plasma inflammatory biomarkers and ISS within the first 24 hours postinjury in the overall TD-1 (n=472) and TD-2 (n=89) survivor cohort. (A) IL-9, (B) IL-21, (C) IL-22, (D) IL-23 and (E) IL-17E/25. IL, interleukin; ISS, Injury Severity Score; TD-1, trauma database-1; TD-2, trauma database-2.
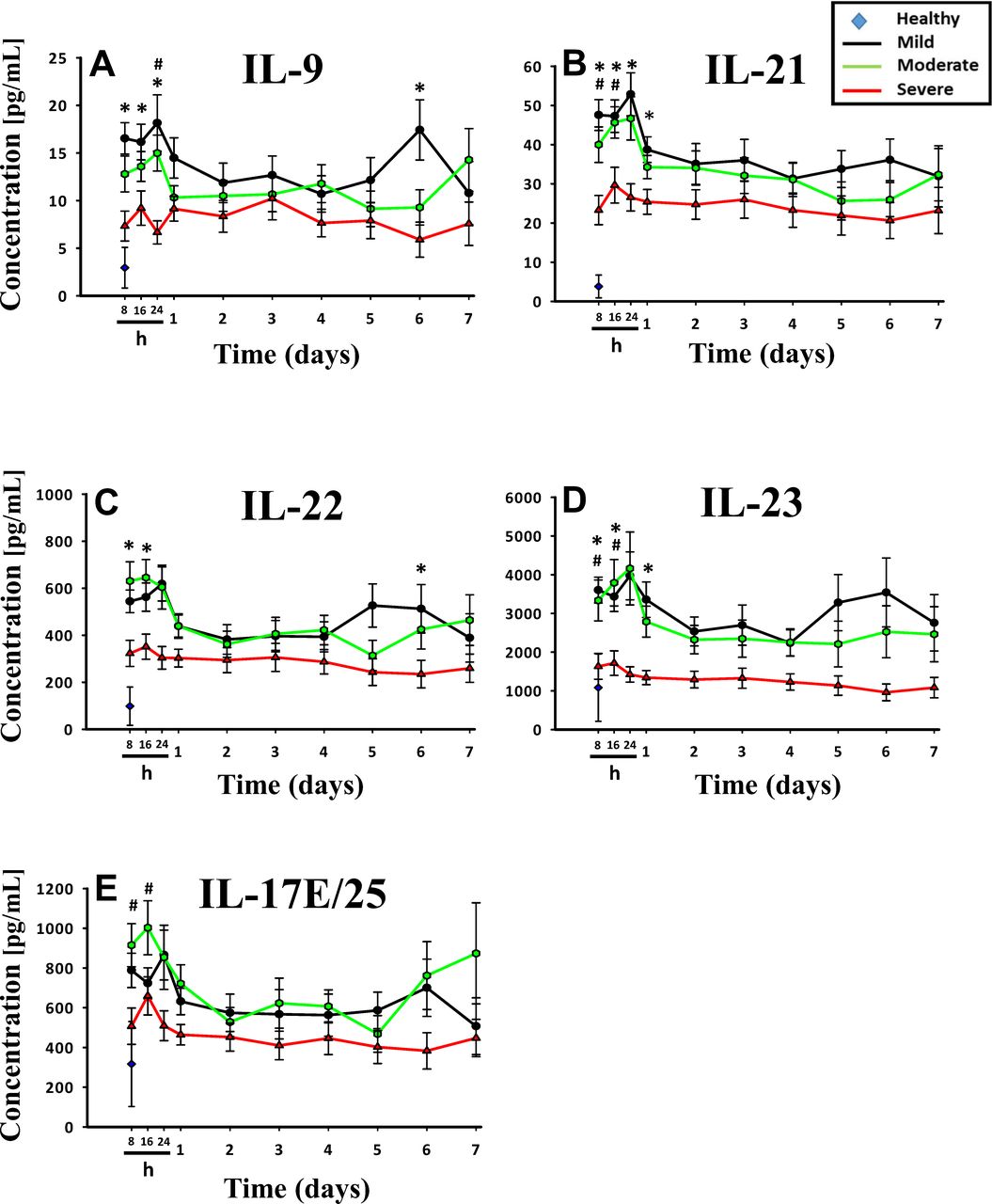
We next extended these observations to determine if the ISS-dependent suppression of IL-9, IL-21, IL-22, IL-23 and IL-17E/25 persisted over time using data from TD-1 (figure 2). This permitted an analysis of the cytokines daily to day 7 after injury. Interestingly, the five inflammation biomarker levels exhibited a paradoxical suppression that was discerned in the severe ISS group (IL-9 (p<0.001), IL-21 (p<0.001), IL-22 (p<0.001), IL-23 (p<0.001) and IL-17E/25 (p<0.001)) (figure 2 and online supplemental figure 2). Whereas the levels of these mediators in the mild, moderate and severe ISS subgroups were significantly higher than controls, all five were statistically significantly lower within the initial 24 hours postinjury and during the entire 7 days of hospital stay in the severe ISS group when compared with the mild and moderate ISS groups.
Supplemental material
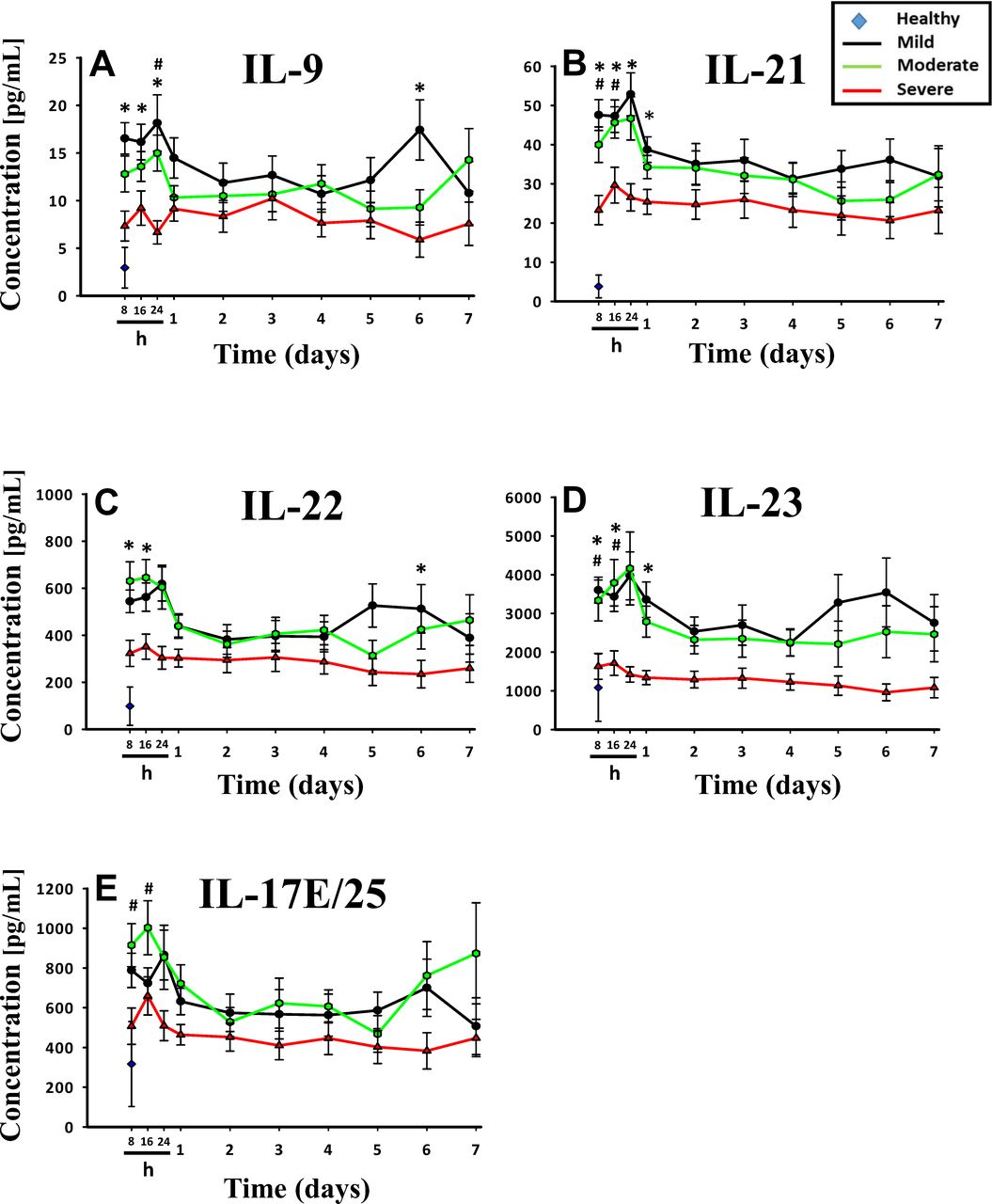
Time course analysis of inflammation biomarkers in the mild, moderate and severe ISS-based groups from time of injury up to 7 days in TD-1 (University of Pittsburgh). Circulating levels of inflammatory mediators in the mild (n=180), moderate (n=170) and severe (n=122) ISS groups assessed in serial plasma samples obtained at the indicated time points. Time courses of (A) IL-9, (B) IL-21, (C) IL-22, (D) IL-23 and (E) IL-17E/25. Values are mean±SEM. *Mild versus severe, #moderate versus severe; p<0.05 by two-way analysis of variance. IL, interleukin; ISS, Injury Severity Score; TD-1, trauma database-1.
Finally, we sought to evaluate the effect of age and gender differences on the circulating levels of the five biomarkers. To do this, we used age cutoffs of ≤30 and ≥65 years to signify the young and old groups, respectively, which was adapted from a recent study using the TD-1 cohort.5 This analysis revealed that there were no statistically significant differences in the five biomarkers between the young (n=114) and the aged (n=101) trauma patients (data not shown). In addition, the TD-1 cohort was analyzed based on gender differences, and the five biomarkers were compared between 330 male and 142 female trauma patients. This analysis showed that there was no statistically significant difference in circulating levels in all the five biomarkers between male versus female patients (data not shown).
Validation of results using a contemporary and separate patient dataset
Next, we performed the same analysis with TD-2 data using 8-hour, day 1 and day 3 samples postinjury. Similarly, it was found that IL-9 (p<0.001), IL-21 (p=0.049), IL-22 (p<0.001) and IL-17E/25 (p=0.049) were statistically significantly lower in the severe group compared with the mild and moderate ISS groups (figure 3). Of note, the absolute circulating levels of these biomarkers in TD-2 were relatively higher compared with absolute biomarker levels in TD-1 (figure 2); this was also apparent in the linear regression analysis. In contrast, IL-1RA (p<0.001), IL-1β (p=0.010), sIL-2RA (p=0.003), IL-5 (p=0.093), IL-6 (p=0.045), IL-7 (p=0.009), IL-8/CCL8 (p=0.025), IL-10 (p=0.003) and MCP-1/CCL2 (p<0.001) remained statistically significantly elevated with increasing injury severity (online supplemental figure 3).
Supplemental material
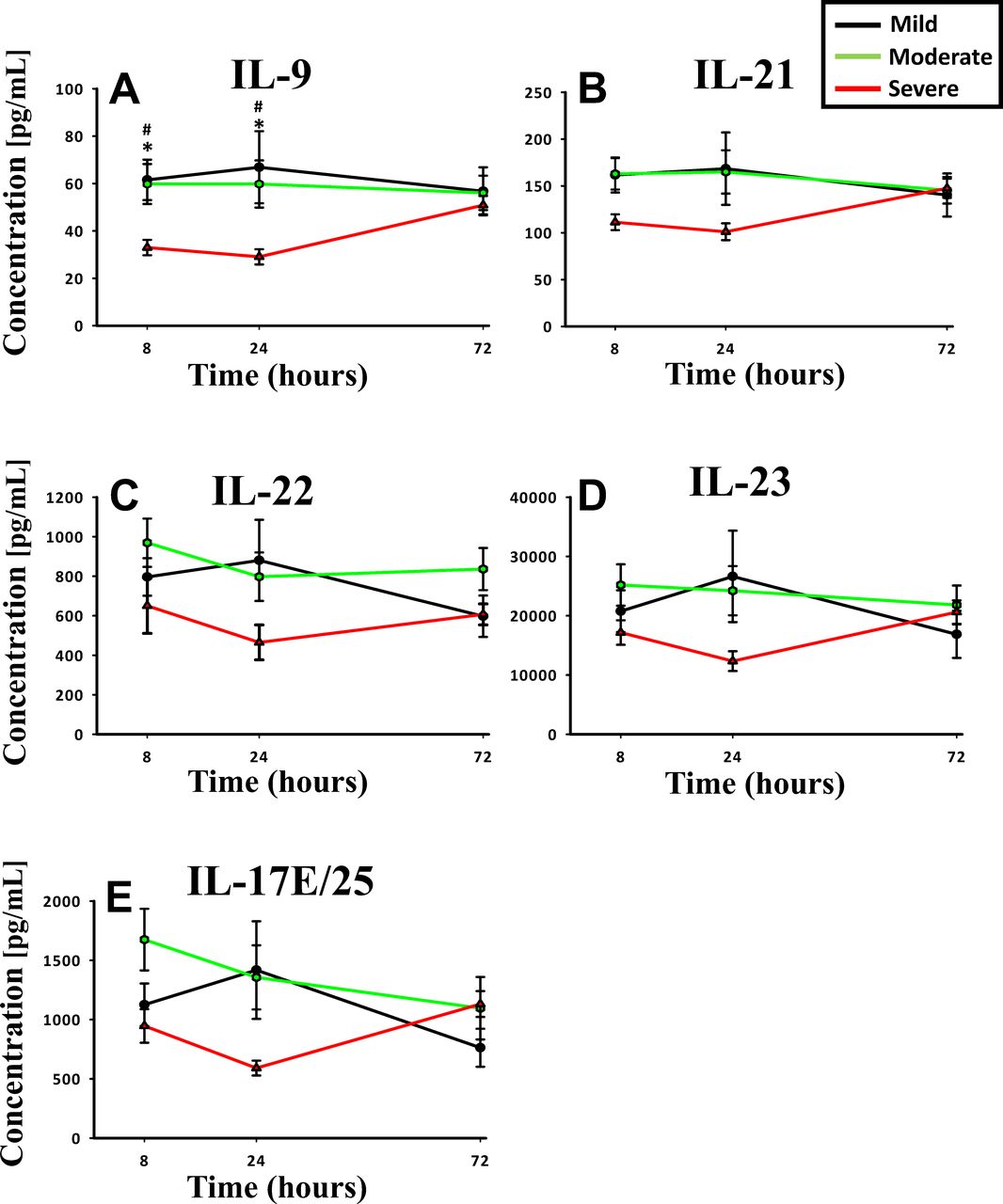
Time course analysis of inflammation biomarkers in the mild, moderate and severe ISS-based groups from time of injury up to 3 days in TD-2 (Indiana university). Mean circulating levels of inflammatory mediators in the mild (n=12), moderate (n=21) and severe (n=56) ISS groups assessed in serial plasma samples obtained at the indicated time points. Time courses of (A) IL-9, (B) IL-21, (C) IL-22, (D) IL-23 and (E) IL-17E/25. Values are mean±SEM. *Mild versus severe, #moderate versus severe; p<0.05 by two-way analysis of variance. IL, interleukin; ISS, Injury Severity Score; TD-2, trauma database-2.
Discussion
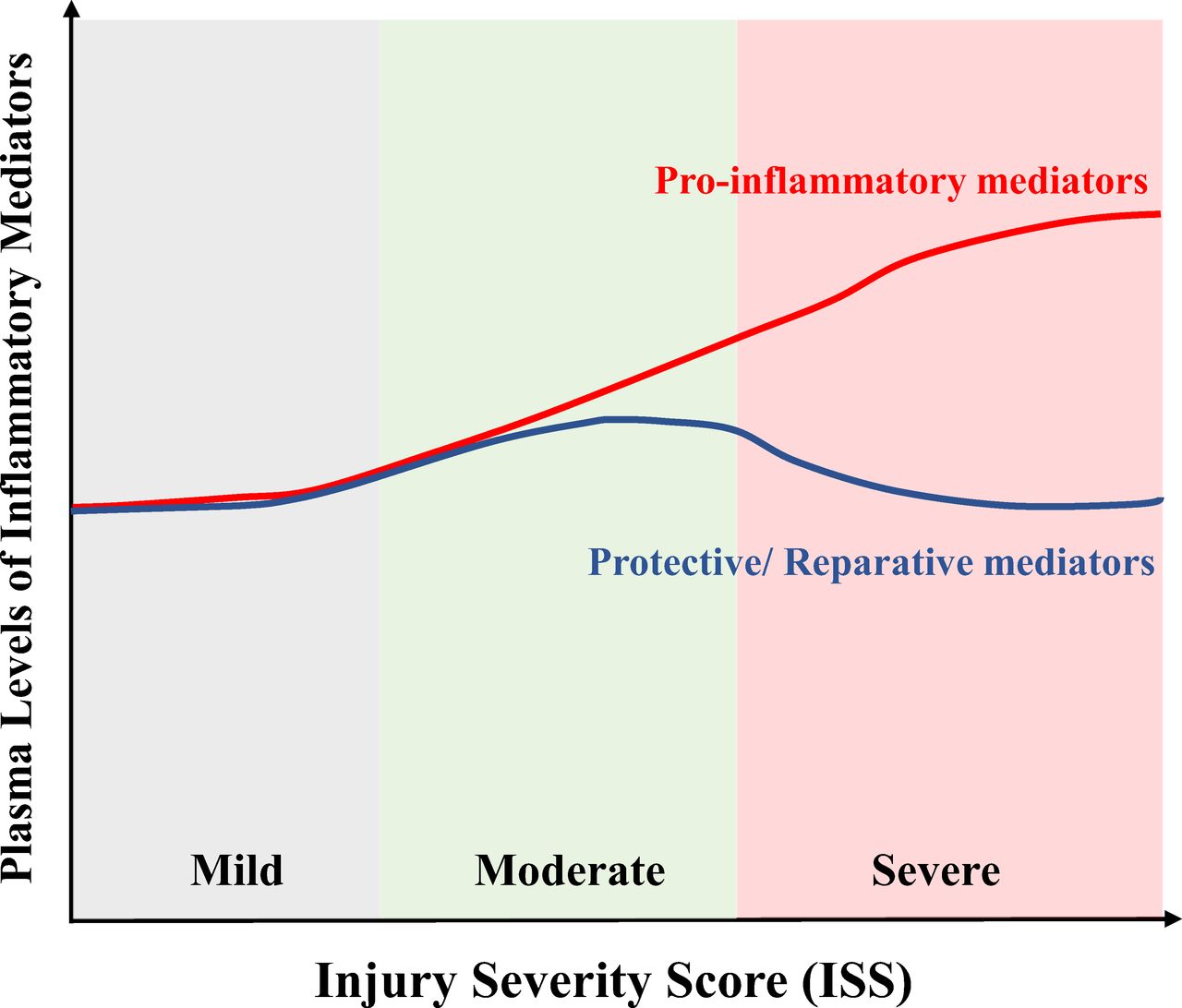
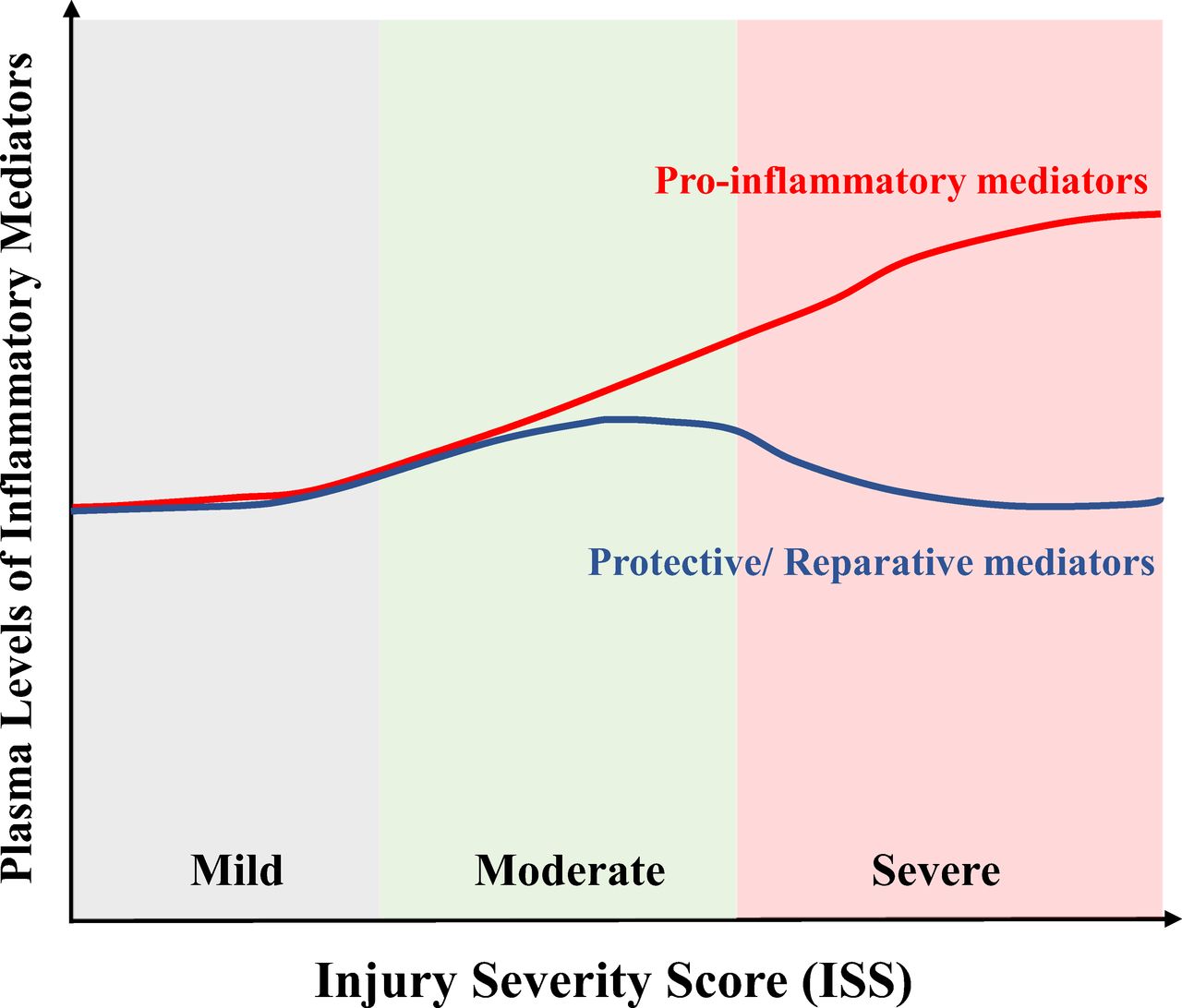
By extending the number of mediators analyzed in two previously reported trauma datasets to include cytokines associated with tissue repair and protection, we were able to demonstrate that, unlike proinflammatory cytokines that increase in the circulation with injury severity, protective/reparative cytokines are suppressed in the most severely injured patients. Although we observed a similar pattern of suppression of protective/reparative cytokines in both the TD-1 and TD-2 cohorts, the absolute concentration levels were different between the two cohorts. We speculate that this difference could be related, in part, to different patient demographics and different injury patterns between the two cohorts. These novel observations have led us to propose the paradigm depicted in figure 4 to demonstrate the relationship between injury severity and the release of cytokine immune modulators after injury. We speculate that the suppression of protective/reparative cytokines in the face of higher proinflammatory mediators could render the severely injured patient more susceptible to persistent organ dysfunction and tissue damage. The mechanisms leading to the suppression of protective/reparative cytokines will require further research; however, these findings can serve as the bases for further work in this important area of investigation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic that depicts the relationship between injury severity and the release of cytokine immune modulators after injury. Proinflammatory mediators, which are known to contribute to excess inflammation and tissue injury after trauma, continue to increase as injury severity increases. In contrast, a set of protective/reparative cytokines increase at lower and more survivable levels of injury but then become suppressed above a certain threshold of injury severity.
IL-22 plays an important role in host protection against microbes by preserving the integrity of boundary organs and tissues, such as skin, pancreas, intestine, liver and lung,13 and by enhancing the production of antibacterial proteins and proteins involved in tissue protection and survival.14 Subcutaneous administration of IL-22 accelerates wound closure by inducing keratinocyte migration and proliferation in murine model of diabetes.15 In addition, IL-22 ameliorates renal injury in acute kidney injury by suppressing inflammation.16 IL-17E/25 is derived from the epithelium and has a recognized role in the promotion of type II immunity. Recent work has shown that after injury, IL-17E/25 and IL-33 act on innate immune cells including basophils, mast cells and group 2 innate lymphoid cells for initial production of type II cytokines IL-4, IL-5 and IL-13.17 These cytokines support differentiation of CD4+ T cell into T helper 2 (Th2) cells and promote Th2 cell effector functions. Other studies have shown that IL-17E/25 and IL-22 act synergistically in type II immune responses.18 Similar to IL-22, IL-17E/25 was shown to be capable of inhibiting Lipopolysaccharide (LPS)-stimulated production of proinflammatory cytokines from macrophages.19 As part of the type II immunity, IL-9 was shown to also play an important role in tissue protection after injury20 and restoring hemostasis after inflammation.21
The underlying mechanism leading to the suppression of IL-21 and IL-23 at high ISS is less clear. Both have a range of regulatory functions relevant to the immune response to injury. IL-23 has been shown to promote neutrophil influx into the lungs of mice subjected to hemorrhagic shock.22 IL-21 is regulated by IL-17A and can also propagate Th2 and Th17 responses, depending on the circumstances.23 The consequences of the suppression of these two cytokines after severe injury will require further study.
We recognize that there are several limitations in our study. First, this study was performed using blunt trauma cohorts who survived up to discharge. We suggest that a prospective evaluation of biomarker changes in a more heterogenous trauma population that includes non-survivors and other injury patterns would yield more insight into the association between the trauma-induced inflammatory response and outcomes after injury. Second, severe traumatic injury is often accompanied by physiological and metabolic perturbations which in turn can contribute to immune dysregulation, and therefore the results should be interpreted within this context. Finally, as patients with favorable clinical trajectories were discharged from hospital, this led to a decreasing number of patients over time, which resulted in a gradual selection of patients with unfavorable outcome, probably most pronounced in patients with lower ISS (online supplemental figure 4). However, examining the circulating biomarker levels, we note that our results showed that most of the statistically significant differences among the three ISS groups occurred within the first 24 hours from time of injury, which in theory captured the majority of the patient sample size during the initial 24-hour period.
Supplemental material
Acknowledgments
The authors acknowledge all study collaborators and research staff for collection and analysis of the data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
TRB and RAN are joint senior authors.
Contributors Conception and design of the study: JC, TRB and RAN. Acquisition of data, analysis and data interpretation: JC, TMcK, IB, MSZ, GG, YV, DSG and RAN. Drafting the article or revising it critically for important intellectual content: JC, TMcK, MSZ, GG, YV, TRB and RAN. Final approval of the version to be submitted: JC, TMcK, MSZ, YV, TRB and RAN.
Funding This work was supported, in part, by the National Institutes of Health (grant P50-GM-53789).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the University of Pittsburgh and Indiana University Institutional Review Boards (IRBs) (PRO number 08010232 and 1411863767, respectively). Informed written consent was obtained from each patient or next of kin per IRB regulations.
Provenance and peer review Not commissioned; externally peer reviewed.