Article Text

Abstract
Background Resuscitative endovascular balloon occlusion of the aorta (REBOA) is an emerging technique used for non-compressible torso hemorrhage. However, its current use continues to be limited and there is a need for a simple, fast, and low profile REBOA device. Our objective was to evaluate the feasibility of a novel 4 French REBOA device called the COBRA-OS (Control of Bleeding, Resuscitation, Arterial Occlusion System).
Methods This study is the first-in-human feasibility trial of the COBRA-OS. Due to the difficulty of trialing the device in the trauma setting, we performed a feasibility study using organ donors (due to the potential usefulness of the COBRA-OS for normothermic regional perfusion) after neurological determination of death (NDD) prior to organ retrieval. Bilateral 4 French introducer sheaths were placed in both femoral arteries and the COBRA-OS was advanced up the right side and deployed in the thoracic aorta (Zone 1). Once aortic occlusion was confirmed via the left-sided arterial line, the device was deflated, moved to the infrarenal aorta (Zone 3), and redeployed.
Results A total of 7 NDD organ donors were entered into the study, 71% men, with a mean age 46.6 years (range 26 to 64). The COBRA-OS was able to occlude the aorta in Zones 1 and 3 in all patients. The mean time of placing a 4 French sheath was 47.7 seconds (n=13, range 28 to 66 seconds). The mean time from skin to Zone 1 aortic occlusion was 70.1 seconds (range 58 to 105 seconds); mean balloon volumes were 15 mL for Zone 1 (range 13 to 20 mL) and 9 mL for Zone 3 (range 6 to 15 mL); there were no complications and visual inspection of the aorta in all patients revealed no injury.
Discussion The COBRA-OS is a novel 4 French REBOA device that has demonstrated fast and safe aortic occlusion in this first-in-human feasibility study.
Level of evidence Level V, therapeutic.
- REBOA
- COBRA-OS
- organ donor
- trauma
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Further data are available through Trillium Gift of Life Network, 2020, Toronto, Ontario but must remain confidential due to the sensitive nature of organ donation.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Despite a steady increase in the use of endovascular resuscitation and trauma management techniques in recent years,1 the widespread adoption and use of resuscitative endovascular balloon occlusion of the aorta (REBOA) has been limited. REBOA, a minimally invasive alternative to resuscitative thoracotomy, is a procedure that provides temporary aortic control and minimizes hemorrhage to allow for definitive surgical hemostasis in non-compressible torso hemorrhage (NCTH), among other clinical applications.2 There has been a concerted effort to more clearly define the patient populations that truly benefit from REBOA,3 4 but controversy remains.5–7 Furthermore, the technological limitations of currently available REBOA devices have limited their use primarily to the most experienced trauma providers and centers, and in military settings.8 There is a need for improved REBOA technologies to better meet the needs of the front-line personnel who are using this tool to serve their patients.
Apart from being used as an adjunct for hemorrhage control, another potential application of aortic occlusion devices is during organ donation, particularly donation after circulatory death (DCD) with normothermic regional perfusion (NRP), when oxygenated blood helps to prevent warm ischemic injury to organs.9 Aortic occlusion in these donors helps to prevent perfusion of oxygenated blood to the heart and brain, a reversal of typical REBOA applications. Organ donors therefore represent an ideal population to study the feasibility of placing an aortic occlusion balloon percutaneously for NRP purposes and simultaneously evaluating a novel REBOA device in a more controlled environment than the trauma suite with often unstable patients.
This study represents the first-in-human feasibility trial of the COBRA-OS (Control of Bleeding, Resuscitation, Arterial Occlusion System) (Front Line Medical Technologies, London, Ontario, Canada), a novel 4 French (Fr) REBOA device, in organ donor patients.
Methods
An investigational testing authorization (ITA) (Application #298250) was obtained through Health Canada to conduct this study using a patient population of organ donors after neurological determination of death (NDD). Research Ethics Board approval (REB #112212) was obtained from Western University prior to recruitment. Approval was also obtained from the Trillium Gift of Life working groups in Ontario, Canada, to ensure that the protocol did not interfere with the quality of procured organs. The study was conducted at London Health Sciences Center in London, Ontario, Canada. Inclusion criterion was NDD organ donors over the age of 18 and subjects were excluded if the research team was unable to obtain consent, if the subject was considered hemodynamically unstable, or if the organ donor team had objections due to the condition of the intended recipient. Informed consent was obtained from the subject’s substitute decision maker by the study team, separately from and after the consent for organ donation.
The COBRA-OS
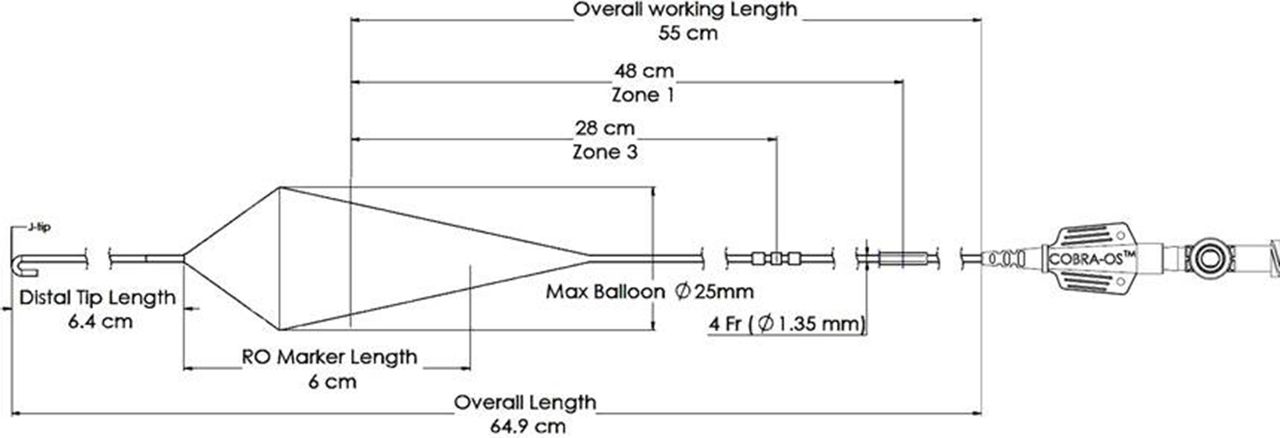
The device used for aortic occlusion in this study was the COBRA-OS (see figures 1 and 2). The COBRA-OS is a large vessel balloon occlusion system designed to be inserted through a 4 Fr sheath. A 4 Fr Custom Sheath Introducer Kit (0.018-inch guidewire) that accompanies the device is used to gain access to the common femoral artery in the groin (see figure 3A,B). The COBRA-OS is designed to occlude the aorta in the descending thoracic aorta (Zone 1; solid black marker; indicating 48 cm depth) or to occlude the aorta below the renal arteries (Zone 3; three black markers; indicating 28 cm depth). Its overall working length and therefore maximal reach is 55 cm. The device consists of a stiff stainless-steel inner guidewire with an atraumatic floppy distal J-tip that is housed in a compliant occlusion balloon with proximal and distal necks. No other guidewires are required and this is not an over-the-wire device. A reusable J-tip straightener is preloaded on the distal neck to facilitate the introduction of the device into the 4 Fr introducer sheath hemostasis valve. Although the 4 Fr sheath can be used as an arterial line monitor, a separate femoral arterial line may already be in place. For example, if a typical Arrow 18 gauge, 16 cm length, femoral arterial line (Teleflex, Pennsylvania, USA) is initially used, then the 42 cm 0.018 inch guidewire included with the 4 Fr Custom Sheath Introducer Kit can easily be inserted through the arterial line lumen. The arterial line would then be removed over the wire and the 4 Fr introducer sheath placed over the same wire for subsequent aortic occlusion with the COBRA-OS.
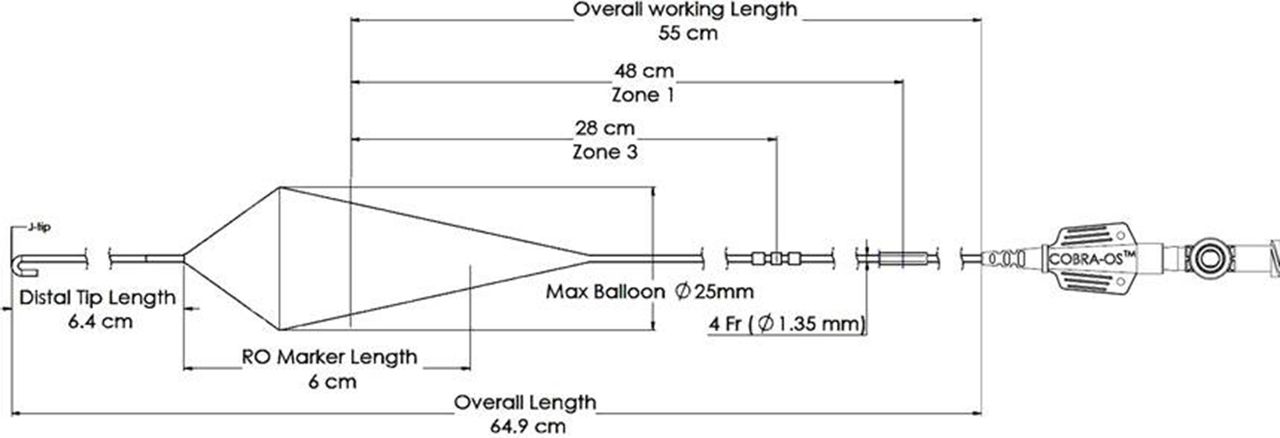
Schematic of the COBRA-OS. COBRA-OS, Control of Bleeding, Resuscitation, Arterial Occlusion System.

Image of the COBRA-OS with syringe attached. COBRA-OS, Control of Bleeding, Resuscitation, Arterial Occlusion System.
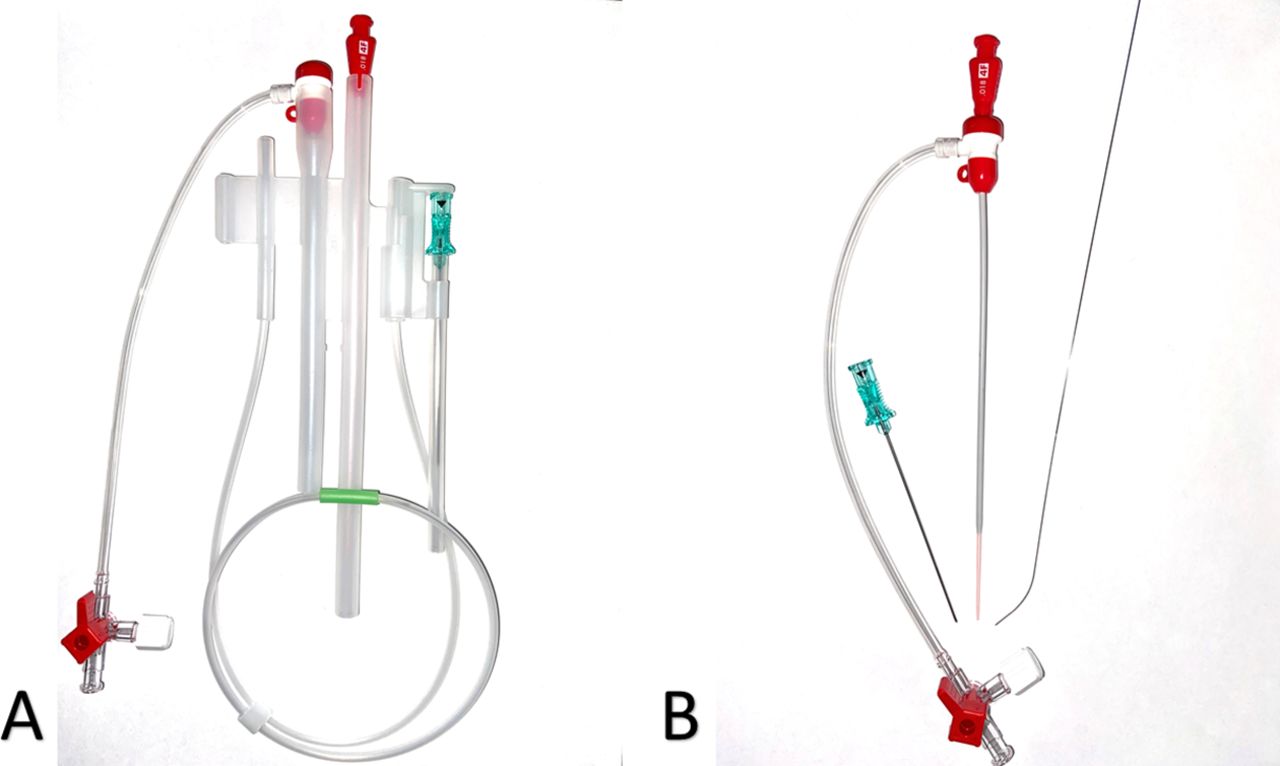
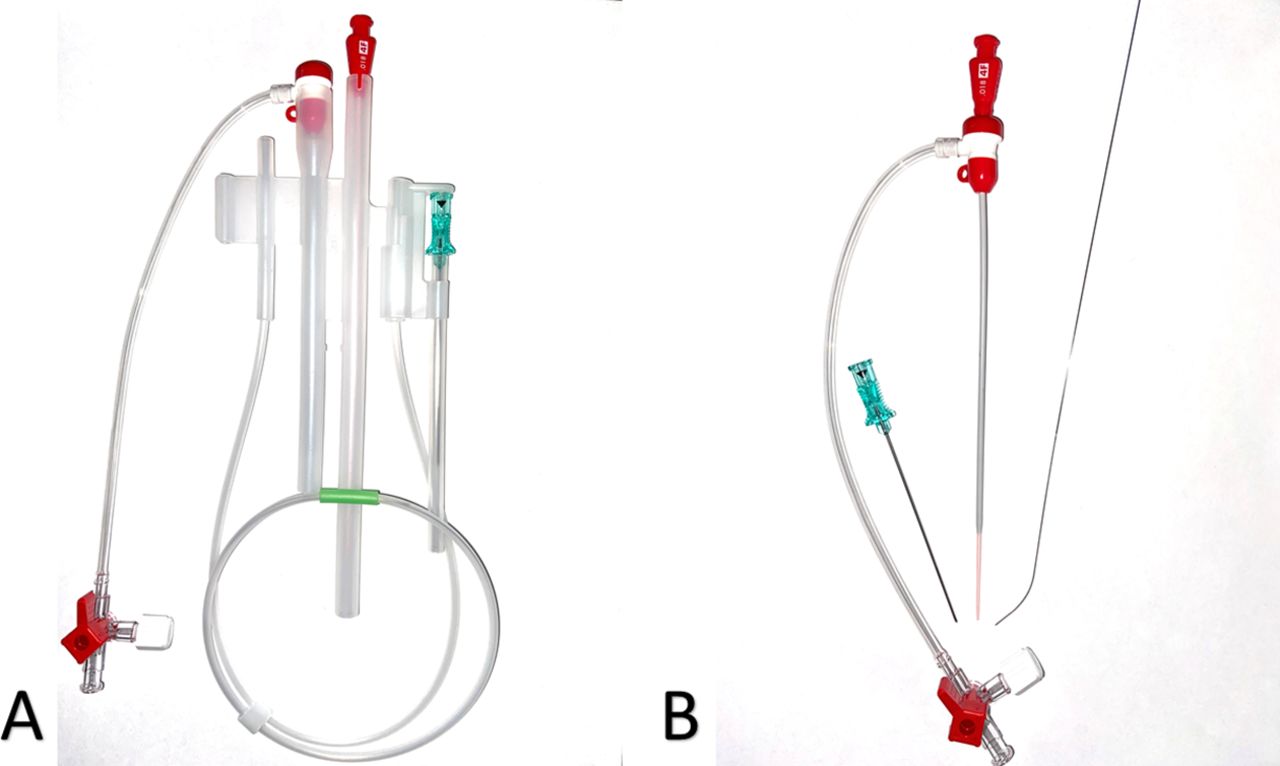
Image of the 4 Fr Custom Sheath Introducer Kit. (A) Kit in holster. (B) 4 Fr sheath with introducer, 21-gauge needle, 0.018-inch guidewire. Fr, French.
Procedure
A single general and vascular surgeon (AP) performed all procedures as per the approved ITA protocol and the instructions for use were followed for the device. The study subject was brought to the operating room for organ procurement and prior to incision, a 4 Fr sheath was placed in the left common femoral artery percutaneously using an 0.018-inch micropuncture kit (4 Fr Custom Sheath Introducer Kit) under ultrasound guidance. The sidearm was attached to an arterial line setup to measure femoral artery blood pressure and ultimately to confirm aortic occlusion. Organ procurement started in the standard fashion and when the supraceliac aortic occlusion step was necessary prior to controlled cardiac arrest, a right-sided 4 Fr sheath was placed as before and the COBRA-OS was introduced and inflated with normal saline in the descending thoracic aorta (Zone 1 REBOA) for 1 minute and then deflated. Successful aortic occlusion was documented with flat-lining of the left-sided femoral arterial line and loss of pulse with palpation of the aorta directly below the device. Palpation of the aorta above and below the device also confirmed appropriate zone positioning. The COBRA-OS device was then pulled back and deployed in the infrarenal aorta (Zone 3 REBOA) for another minute and aortic occlusion/positioning was again documented. The device was then deflated and removed from the sheath. Visual inspection of the aorta at the aortic occlusion sites was performed directly for any external damage. Organ procurement then proceeded using standard techniques.
The primary outcomes of this study were the ability of the COBRA-OS to occlude the aorta at Zones 1 and 3, the individual times of placing the 4 Fr introducer sheaths, and the time from needle touching skin (including access) to Zone 1 aortic occlusion. Balloon volumes, access related complications, and external visual inspection of the aorta at Zones 1 and 3 were also recorded.
Results
A total of 10 NDD organ donor subjects were approached for the study and 3 were excluded (1 was hemodynamically unstable, 1 organ donor team refused participation due to the condition of the intended recipient, and 1 subject’s substitute decision maker did not give consent). Therefore, five male patients (71%) and two female patients (29%) were entered into the study, for a total of seven patients with a mean age of 46.6 (range 26 to 64). Causes of death were kept confidential to protect the identity of the donors, but all donors met criteria for brain death and were considered hemodynamically stable on entry into the operating room.
The COBRA-OS was able to occlude the aorta in Zone 1 and Zone 3 in all seven patients. The mean time of placing the 4 Fr sheaths was 47.7 seconds (n=13, range 28 to 66 seconds). The mean time from needle in skin to Zone 1 aortic occlusion was 70.1 seconds (range 58 to 105 seconds). Mean balloon volumes were 15 mL for Zone 1 (range 13 to 20 mL) and 9 mL for Zone 3 (range 6 to 15 mL). There were no complications and external visual inspection of the aorta in all patients revealed no injury.
Discussion
REBOA is indicated for traumatic life-threatening hemorrhage below the diaphragm in patients who present in hemorrhagic shock and are unresponsive or transiently responsive to resuscitation.10 Although REBOA offers a minimally invasive approach to aortic occlusion, there are technical challenges that accompany the procedure which have contributed to its limited use in practice. One of the limiting factors has been device profile, as procedure time and complications may increase with catheter size.11–16 It is intuitive that smaller access sheaths in coagulopathic trauma patients would be preferred from an access site bleeding complication standpoint and eliminating the need to upsize an initial low-profile sheath can speed up the overall procedure.
This first-in-human feasibility study demonstrates the safety and effectiveness of a novel 4 Fr REBOA device. Existing REBOA devices continue to require a 7 Fr sheath, which is a larger sheath profile than with most standard percutaneous endovascular products used by expert interventionalists (most often 5 to 6 Fr). By reducing the profile to 4 Fr, the aim was to decrease access site complications and simplify the procedure by eliminating the need to upsize an initial sheath. In addition to the reduction in profile, the COBRA-OS was also designed to be “fluoroscopy-free” (without the need to be tracked over a wire), have an atraumatic flexible tip for safe blind advancement in arteries, and have a stiff enough body to withstand aortic pressures during full aortic occlusion. Besides safety and effectiveness, this study also demonstrates that the device can be deployed very quickly in experienced hands, although under very controlled circumstances.
There are some key differences to be noted about the COBRA-OS compared with other REBOA devices besides the reduction in profile. Similar to other devices, but not all, it is not an over-the-wire device and instead is inserted directly through the empty 4 Fr sheath and advanced atraumatically into the aorta to either Zone 1 or Zone 3. The device does not have a built-in arterial line, contrary to some other devices, and therefore an alternative means to monitor blood pressure and confirm aortic occlusion must be used. The device is also only indicated for vessels up to 25 mm in diameter, with typical trauma patient proximal thoracic aortic diameters being approximately 23 mm.17 This was a conscious design feature to help prevent aortic and balloon rupture by setting the maximum volume of the compliant balloon at 13cc, equivalent to 25 mm. In addition, the COBRA-OS has only two markers on the shaft to indicate typical distances for Zone 1 (single black marker at 48 cm depth) and Zone 3 (three black markers at 28 cm depth) as suggested by Eliason et al for fixed REBOA length catheters,18 compared with other devices with either no markers or markers on the entire length of the device. It also has a unique offset ice-cream cone shaped balloon with a safety shoulder reservoir, compared with other elliptical or spherical shaped balloons, that was incorporated into the design to help prevent rupture of the balloon or aorta during inflation. The shape and design of the balloon also lends to its ability to achieve partial-REBOA on deflation if desired, which is not easily achieved by some other compliant REBOA balloon systems.19
The COBRA-OS can be used to improve the situations in which REBOA is currently being used. Depending on local institutional protocols for trauma patients, the COBRA-OS 4 Fr sheath can be placed in the femoral artery and used as a femoral arterial line to monitor blood pressure. Early femoral access when considering REBOA has been associated with a survival advantage.20 If REBOA is not required, the 4 Fr sheath can be removed and manual compression can be used for hemostasis. However, if REBOA is required, the COBRA-OS can be quickly deployed without the need to insert a separate stiff wire and upsize to a larger sheath, thus making the procedure simpler and less cumbersome, avoiding additional endovascular equipment which is not always readily available in trauma suites.
Apart from the advantages of reducing potential access site complications and increasing the speed of the procedure, a smaller profile access sheath and device traversing the iliac arteries and aorta has other benefits. Larger sheaths are known to be more obstructive in small and often tortuous iliac vessels. Trauma patients are frequently known to have vasospastic blood vessels and are often started on vasopressor medications which vasoconstrict their vasculature. Therefore, a 7 Fr sheath may be fully or partially occlusive, potentially promoting vessel thrombosis, especially if left in place when patients are transferred to postoperative care. It is unknown if a 4 Fr sheath will reduce vessel thrombosis if left in place postoperatively but the significantly lower profile makes this a possibility. The 4 Fr sheath may be used as an arterial line monitor during postoperative care and even as a conduit to a subsequent REBOA device placement if the patient becomes hemodynamically unstable again.
When considering applications other than trauma, a low-profile system may be equally advantageous. In patients with hypercoagulable postpartum hemorrhage who often have small vasospastic iliac vessels and aorta, the 4 Fr COBRA-OS may be the ideal Zone 3 aortic occlusion device to be placed and only deployed if necessary, decreasing the chance of vessel thrombosis and potential limb loss when using REBOA as a surgical adjunct.21 Furthermore, in patients presenting with severe trauma to non-level 1 trauma centers or in prehospital scenarios, the smaller and less obstructive 4 Fr sheath and COBRA-OS may potentially be placed prophylactically for patient transfer and REBOA only used if the patient becomes unstable.22 Finally, in pediatric REBOA scenarios, a low-profile system would be preferable due to the inherent smaller size of access vessels and aorta in this patient population.23
As described here, low-profile aortic occlusion balloons may be used to potentially improve the efficiency of NRP techniques during organ procurement. NRP is an evolving technique to improve the function of procured organs after controlled or uncontrolled DCD.24 Low-profile occlusion balloons placed percutaneously may enable less manipulation of the DCD organ donor during preparation prior to organ procurement. These devices may play an important role in the future of NRP techniques, but have yet to be studied extensively.
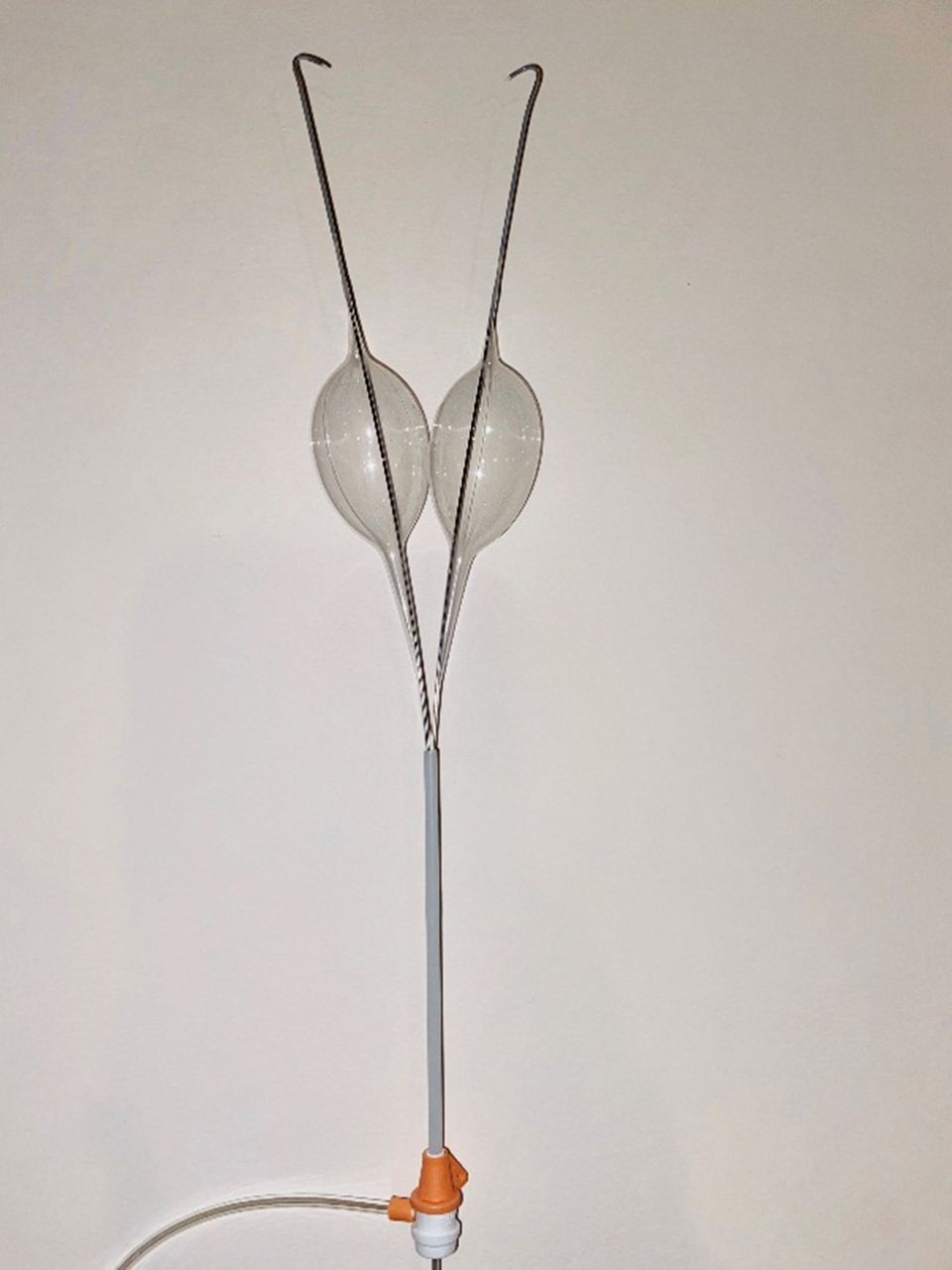
To our knowledge, this is the lowest profile aortic occlusion device ever reported25 and we think that the 4 Fr COBRA-OS represents a significant improvement in REBOA technology by lowering the profile without compromising aortic occlusion ability. Due to the lower profile, we expect adoption for REBOA to increase when this device becomes widely available, similar to when there was a transition from 12 Fr to 7 Fr devices. For perspective on device profile, a typical femoral arterial line is 18 gauge or 1.3 mm outer diameter (OD); the 4 Fr sheath used with the COBRA-OS is approximately 1.8 mm OD; and a typical 7 Fr sheath is approximately 3.1 mm OD. See figure 4 for demonstration of two COBRA-OS devices fitting through a 7 Fr sheath. Further studies and use of the COBRA-OS will help elucidate the benefits of this low profile REBOA device.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Image of two COBRA-OS devices fitting through a 7 Fr sheath. COBRA-OS: Control of Bleeding, Resuscitation, Arterial Occlusion System; Fr, French.
There are a number of limitations with this study. The procedure was completed by a single expert general and vascular surgeon under controlled circumstances at a single center which raises the question of whether these results are repeatable in emergency trauma suite scenarios with users that are not as familiar with the device. In addition, the relatively small number of patients limits broad generalizations about the device in all patient populations and applications.
Conclusion
The novel 4 Fr COBRA-OS has demonstrated the ability to provide fast and safe aortic occlusion in this first-in-human feasibility study and is a viable option for patients in whom REBOA is deemed necessary.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Further data are available through Trillium Gift of Life Network, 2020, Toronto, Ontario but must remain confidential due to the sensitive nature of organ donation.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank the Trillium Gift of Life Network, 2020, Toronto, Ontario, for their incredible support of this project.
References
Footnotes
Contributors APo, OS, and TN were involved in study design and submission of the ITA application to Health Canada and Western University’s REB. APo, APa, OS, and TN were involved in data collection. All authors were involved in data analysis, data interpretation, and critical revisions. The first draft of the article was written by APo.
Funding This study was generously funded by Western University’s Department of Surgery Internal Research Fund 2019.
Competing interests A Power and A Parekh are co-founders and have an equity stake in Front Line Medical Technologies Inc. L J Moore is Chair of the Scientific Advisory board, has an equity stake, and receives consulting fees from Front Line Medical Technologies Inc.
Provenance and peer review Not commissioned; externally peer reviewed.