Article Text

Abstract
Background Trauma is an ever evolving world problem that needs close attention and devising means to prevent and treat. The aim of the study is to identify the main reason for trauma admissions and assess the patient outcome after intervention. Therefore, knowing its actual nature might aid in postulating possible intervention as well as prevention measures.
Method A cross-sectional study was conducted from August to December 2015 in Jimma University Specialized Hospital, which is located in south-western Ethiopia. Two hundred and eleven consecutive trauma admissions to surgery department were included in the study. Data were collected and analyzed using computer software SPSS V.23.
Result A total of 211 admitted trauma patients were studied with male to female ratio of 3.14. The leading cause of trauma admission was road traffic collision at 84 (39.8%) and the least being bullet injury which was 6 (2.8%). Hospital mortality was 31 (14.7%). Factors associated with outcome of patients before discharge from hospital were male sex, adjusted OR (AOR)=2.3, 95% CI 1.08 to 4.75; Glasgow Coma Scale score 15/15, AOR=0.04, 95% CI 0.00 to 0.46; and hemoglobin >10 g/L, AOR=0.225, 95% CI 0.074 to 0.464, p<0.05.
Conclusion Road traffic collision takes the top position from all causes of trauma and unlike other developed countries and low and middle-income countries, pedestrians and motorcyclists were the major victims of the collision in this study.
Level of evidence VI (This level of effectiveness rating scheme is based on the following: Ackley, B. J., Swan, B. A., Ladwig, G., & Tucker, S. (2008). Evidence-based nursing care guidelines: Medical-surgical interventions. (p. 7). St. Louis, MO: Mosby Elsevier.
- accidents
- traffic
- multiple trauma
- patient outcome assessment
Data availability statement
Data are available upon reasonable request. The data can be readily available from the corresponding author upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Trauma is a leading cause of death and disability worldwide, contributing significantly to the global burden of disease but with no much due attention given. The WHO estimates that injury is responsible for more than 5 million deaths annually, more than the mortality caused by HIV, malaria, and tuberculosis combined. It is the most frequent cause of death in the first four decades of life, and it remains a major public health problem in every country, regardless of the level of socioeconomic development.1 2
More than 90% of injury occurs in low and middle-income countries, where formal trauma systems and methods for data tracking have not yet been widely implemented.3 It has traditionally been defined as physical damage to a person caused by an acute transfer of energy (mechanical, thermal, electrical, chemical, or radiation energy) or by the sudden absence of heat or oxygen. This definition has been broadened to include damage that results in psychological harm, maldevelopment, or deprivation.4 Injuries are most commonly categorized with reference to the presumed underlying intent: unintentional injuries include those caused by road trafficcollisions, falls, drowning, burns, and poisonings, and injuries considered to be intentional include those caused by self-harm, interpersonal violence, and war and conflict.4 5
The distribution of injury by mechanisms varies for death, hospitalizations, and emergency department visits. The two leading causes of trauma-related death are related to motor vehicles and firearms, accounting for 29% and 18%, respectively, of all injury-related deaths in 2003. In contrast, falls, the leading cause of non-fatal injury, account for about one-third of hospitalizations and emergency department visits (15% and 18%, respectively). Leading causes of death among the fatal injuries are injuries sustained to the central nervous system for 40% to 50% of the total, and the second one is hemorrhage, accounting for 30% to 35%.2
There are triphasic occurrences of death in trauma patients in which one-third of them occur at the scene of the injury and are therefore inevitable death. Early phase of trauma-related death occurs when patients reach the hospital and cannot be salvaged without emergent intervention. But patients who get advanced trauma management were thought to be salvaged at this phase. The late trauma-related death is associated with infections and malnutrition.6
There were studies conducted in similar set-ups of Ethiopia including Jimma zone and nearby administrative regions concerning the magnitude of trauma visiting emergency departments,7 8 but there was paucity of data with regard to pattern of general trauma admissions and treatment outcomes in these centers.
So this study was aimed to look for the specific causes of trauma admission and treatment outcome of patients at the time of hospital discharge.
Materials and methods
Study design and setting
A cross-sectional study was conducted in Jimma University Specialized Hospital (JUSH) from August 1 to December 31, 2015 which is located in Oromiya region, south-western Ethiopia, 341 km from the capital city. Emergency surgical admissions to surgical ward of JUSH, which is named currently as Jimma University Medical Center, were taken as source population.
Population
The source population was all emergency surgical admissions to JUSH, from which study units with history of trauma were used and calculated using single population formula, N=Zα/2×P(1-P)/d2 (where P is the proportion of trauma admission from similar studies, Z=1.96 at 95% CI, and margin of error d=0.05), taking proportion of trauma admission (P)=20.9%,7 and sample size of 246 was calculated to have adequate power. Due to small study units, convenient sampling technique was used to incorporate all eligible cases of interest. A total of 241 patient registries were retrieved out of which 30 were excluded due to incomplete documentation, and finally 211 cases were included for analysis. We acknowledge that the power from the calculated sample might not be strong as it was based on uncontrolled previous study.
Data collection tool and techniques
The data were collected using a structured questionnaire which was adapted from literatures9–11 by two trained surgical residents. The checklist has sociodemographic characteristics of patients, mechanism of trauma, intention of the injury, specific mechanism of trauma modifiers, patient clinical condition and treatment outcomes. The data were collected prospectively at the time of discharge from patient charts but analyzed retrospectively.
Statistical analysis
The data were analyzed using computer program SPSS V.23. Descriptive statistics were made for categorical variables with frequency, percent and inferential statistics done using logistic regression method. Independent variables were separately analyzed with bivariate logistic regression; variables with p value <0.05 were further analyzed with multivariate logistic regression analysis and explained with adjusted OR (AOR) at 95% CI and p value <0.05 taken as significant association.
Operational definition
Elective trauma surgery patients operated on an elective base after stabilization of acute conditions within a week; especially type I and II Gustilo-Anderson AO (Arbeitsgemeinschaft für Osteosynthesefragen (German for "working group for bone fusion issues")) classification of compound fractures.
Trauma outcome: the condition of a patient on discharge whether alive or dead.
STROBE checklist was used to organize the checklist for editors.12
Result
Sociodemographic characteristics
A total of 211 trauma patients admitted to surgical wards and intensive care unit (ICU) were included during the study period, with the proportion of 160 (75.8%) males and 51 (24.2%) females, with male to female ratio of 3.14. The age distribution showed 120 (56.8%) were in the age range of 11–30 years old (table 1).
Sociodemographic characteristics of trauma admissions to Jimma University Specialized Hospital, August to December 2015
Pattern of trauma, clinical condition and intervention given
Concerning the mechanism of trauma, 84 (39.8%) were from road traffic collisions (RTC) and six patients sustained bullet injury. When these mechanisms of trauma differentiated into age-specific groups, RTC caused 56.0% of patients aged 21–30 years (table 2).
Pattern of trauma and patient characteristic among trauma patients admitted to JUSH, August to December 2015
According to the system involved in the trauma, 111 (52.6%) were musculoskeletal injuries. From the scene of injury to the hospital arrival, it took about 4 hours for 86 (40.8%) of the 111 patients to come, while 25 (12.3%) of them came after 4 days of trauma.
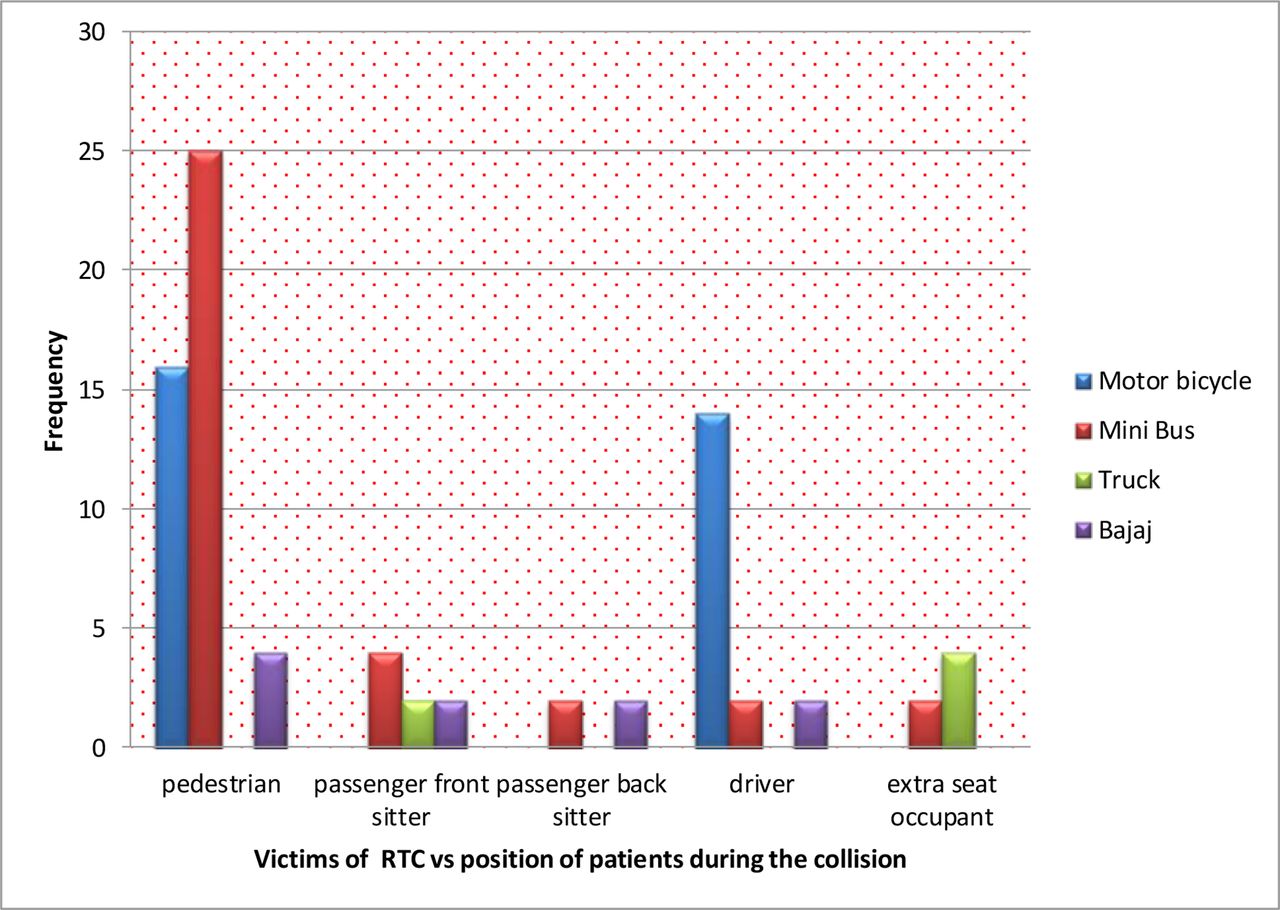
Forty-seven (22.3%) patients sustained intentional injuries of which 32 (68.1%) were due to interpersonal violence. All the RTCs occurred unintentionally and a minibus caused 38 (45.2%) of the collisions. Pedestrians accounted for the higher proportion in which one-third of the victims were children below 10 years (figure 1, table 2).

{kind=link}
The type of motor vehicle and the position of patients during the trauma in patients admitted to Jimma University Specialized Hospital (JUSH) from August to December 2015. RTA, road traffic accident.
Out of the emergency operations done, 34 (24.6%) of them had external fixation for compound fractures/multiple fractures, 20 (14.6%) had laparotomy only for both blunt and penetrating abdominal injuries, 15 (10.9%) had tube thoracotomy, and 23 (16.8%) were operated for traumatic brain injury and depressed skull fractures with elevation and burr hole. Nine patients had both laparotomy and chest tube insertion simultaneously. From the overall 29 laparotomies, 10 (34.5%) had hollow organ perforations, 5 (17.2%) had combination of hollow organ and solid organ injuries, 2 had isolated solid organ injury, another 2 patients had intraperitoneal bladder injury and 3 had diaphragmatic injury, and 7 (24.1%) had no intra-abdominal injury.
After surgery, during immediate postoperative periods in both emergency and elective trauma patients, 157 (88.2%) of them were transferred safely to surgical wards, 16 (9%) were admitted to ICU and 5 (2.8%) died on the operation table and/or in the postanesthetic care unit. The magnitude of death in each specific system was head trauma at 8 (25%) and musculoskeletal injuries at 11 (9.9%). Two or more systems involved 6 (16.2%): abdominal injuries at 4 (23.5%) and chest injuries at 2 (14.3%).
Factors associated with trauma outcome
The outcome of trauma patients admitted during the study period was analyzed with logistic regression for each predictor with bivariate analysis. Sex, blood pressure (BP) of the patient at admission, pulse rate (PR), mental status (Glasgow Coma Scale (GCS) score) and hemoglobin level were found to have a p value <0.25 and further analyzed with multivariate logistic regression, and the following variables were found to have significant association with AOR, 95% CI, and p value <0.05.
Accordingly, 31 (14.7%) (95% CI 14.68 to 14.72) died before hospital discharge and factors associated with increased risk of death were male sex at 27 (87.09%, AOR=2.3, 95% CI 1.08 to 4.75, p=0.03), mental status of patients at presentation (GCS score 15/15, AOR=0.04, 95% CI 0.003 to 0.464), and patient hemoglobin level (AOR=0.252, 95% CI 0.074 to 0.859), all with p value <0.05.
On the contrary, BP ≤90/60 mm Hg and PR >100 were significant in bivariate analysis but were found to be non-significant at multivariate analysis (table 3).
Association between predictor variables and outcome of patients admitted due to trauma to JUSH, August to December 2015
Discussion
This study showed that trauma has affected males more than females and has 2.3 times increased hospital mortality rate (AOR 2.3, 95% CI 1.08 to 4.75, p<0.05). From a demographic study of trauma worldwide, it commonly occurs in young productive force with more occurrence in males.13 14 One-third of the deaths occurred in the age range of 11–40 years, which is similar to the research done in other low and middle-income countries.1 9 15 Probably, this could be due to the majority of outdoor activities performed by adults and children in low and middle-income countries like Ethiopia,15 and males are more affected with traumas. Additionally, males are prone to rage and injuries than females of the same age range.3
Considering the intent of trauma, 159 (75.4%) of the admissions were due to unintentional injury which is in agreement with the result of a systemic review done by Azaj et al.4 RTC was the leading cause of trauma admissions and was nearly the same with the result of a study done at Hawassa University Comprehensive Specialized Hospital which was 40.9%.14 According to Kirya et al, RTC was the leading cause of trauma admissions that accounted for 75%.16 This could be attributed to the geographic difference and concentration of vehicles to larger cities in low and middle-income countries.2
As to the injured system concerned, musculoskeletal system was affected in 111 (52.6%), in a similar way to study2 that showed 113 (53.8%). A prior study from the same institution which included all non-admitted cases showed relatively a lower figure, yet it was a leading injured system.7
The pattern of systemic injury differs with the mechanism of injury. When pedestrians are hit by a moving car, they sustain trauma to the extremities, head or torso, unlike in the case of stab injuries which occur around the trunk. So this result showed that the burden of orthopedic admission was higher in these patients with relatively longer hospital stay, 47 (36.9%) stayed for 7–14 days.
When the trauma triage and transfer were concerned, this study’s result was almost similar to research2 but shorter than the time of hospital arrival of studies conducted in South Africa.17 On the contrary, the average time for transfer in Saudi Arabia was 45 minutes.18
This time is the second peak of mortality at which severely injured patients die, so making as short as possible may save the life of these patients before they go into irreversible stage.6 19
The study revealed in-hospital mortality rate during the study period was 14.7% which is by far greater than the result of study done in Saudi Arabia where hospital mortality was 2.6%,18 but the study done in central India showed 9.5% mortality rate.1 Still, it was higher than the study done at JUSH at 7.5%,7 which was conducted on all injuries presented to the hospital. This difference could be explained by the majority of emergency outpatient department visits which were minor injuries and did not need admission.20 Evidence showed that 50.0% of hospital visits from trauma were minor injuries.21
On stratification of systemic injuries, 8 (25%) of patients who sustained head injury died, which showed higher mortality rate in line with lower mental status level of the patient on presentation. Patients with GCS score of 15/15 have 96% lower chance of dying compared with patients having lower GCS score, AOR=0.04, 95% CI 0.00 to 0.46. A study done by Landes et al22 revealed 21 (10.3%) of patients with head injury admissions died, which was lower than our study finding. In a similar way, patients admitted with hemoglobin level >10 g/L have 75% less chance of dying from trauma (AOR=0.25, 95% CI 0.07 to 0.86). This finding is consistent with the studies that indicated preoperative hemoglobin level, GCS and other parameters were the independent predictors of mortality in trauma patients.23 24 On the contrary, BP <90/60 mm Hg becomes a non-predictor of death despite the fact that hypotension in trauma patients is a clear bad prognostic factor. This could be attributed to small number of counts under this category from the study which has underpowered it.
Conclusion and recommendations
Higher proportion of trauma victims and admissions were male patients aged 11–40 years. RTC was the leading cause of mortality and morbidity. Awareness creation about RTC, improving road safety and posing strict regulation on pedestrians and drivers need further measures. Lastly, as trauma is an ever evolving problem, the government has to establish trauma centers to work on this preventable neglected global problem.
Limitation of the study
The study was conducted at a relatively shorter study period in a single institution which might not be generalized to national or international status of trauma. As the study design was cross-sectional, the power of causal association and temporality could be compromised. Therefore, a larger sample and appropriate design will be needed for which this study might help as a stepping stone.
Data availability statement
Data are available upon reasonable request. The data can be readily available from the corresponding author upon request.
Ethics statements
Ethics approval
Ethical clearance was obtained from the Institutional Review Board (IRB) of Jimma University College of Public Health and Medical Sciences and permission to proceed with data collection was granted from the hospital administrative with reference number IRB1380/15. The data were collected from the patient charts, and patient consent was waived as per the institution’s regulation.
Acknowledgments
We thank our patients and the Jimma University Specialized Hospital ICU/surgical ward staff for their support.
References
Footnotes
Contributors BBB developed the proposal, conducted literature search, wrote the methodology and design, supervised the data collection, analyzed the data and wrote the final result, and interpreted and prepared the final article. SA edited the proposal and wrote the methodology, analyzed and interpreted the data, read the report thoroughly and edited the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.