Article Text

Abstract
Background Emergency department (ED) patients present with complaints and not diagnoses. Characterization and risk stratification based on chief complaint can therefore help clinicians improve ED workflow and clinical outcome. In this study we investigated the 30-day mortality and readmission among ED patients based on chief complaint.
Methods In this cohort study we retrieved routinely collected data from electronic medical records and the Danish Civil Registration System of all ED contacts from July 1, 2016 through June 30, 2017. All patients triaged with one chief complaint using the Danish Emergency Process Triage system were included. Patients with minor injuries were excluded. The chief complaint assigned by the triaging nurse was used as exposure, and 30-day mortality and 30-day readmission were the primary outcomes. Logistic regression was used to determine crude and adjusted ORs with reference to the remaining study population.
Results A total of 41 470 patients were eligible. After exclusion of minor injuries and patients not triaged, 19 325 patients were included. The 30-day mortality and 30-day readmission differed significantly among the chief complaints. The highest 30-day mortality was observed among patients presenting with altered level of conscousness (ALOC) (8.4%, OR=2.0, 95% CI 1.3 to 3.1) and dyspnea (8.0%, OR=2.1, 95% CI 1.6 to 2.6). 30-day readmission was highest among patients presenting with fever/infection (11.7%, OR=1.9, 95% CI 1.4 to 2.4) and dyspnea (11.2%, OR=1.7, 95% CI 1.4 to 2.0).
Discussion Chief complaint is associated with 30-day mortality and readmission in a mixed ED population. ALOC and dyspnea had the highest mortality; fever/infection and dyspnea had the highest readmission rate. This knowledge may assist in improving and optimizing symptom-based initial diagnostic workup and treatment, and ultimately improve workflow and clinical outcome.
Level of evidence Level III.
- diagnosis
- emergency department
- triage
Data availability statement
Data are available upon reasonable request. Data are stored on a local server. The owner of the data is Professor Hans Kirkegaard (hans.kirkegaard@clin.au.dk). Anonymized data can be accessed upon request. Raw data, cleaned data and cleaning protocols are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The number of visits to emergency departments (ED) is increasing. Therefore, the ED workflow, that is, initial treatment and diagnostic workup, needs to be constantly optimized and improved to fit the increased patient flow without placing the patient at risk. Thus, it is crucial to risk-stratify patient groups according to outcome, for example, mortality and readmission. These factors are to a certain degree known for different diagnoses.1 However, patients attending the ED present with a variety of chief complaints, not diagnoses.2 Triage systems classify and prioritize patients according to chief complaint, and hence the initial diagnostic workup and treatment are based hereupon.3 4 It is therefore relevant to characterize the population in the ED based on the patient’s chief complaint—a symptom-based approach.
In recent years, there has been increased focus on symptom-based research.5 Studies have shown that the ED patient’s chief complaint can be used as a predictor of mortality, both long term and short term.6–10 Likewise, revisits to the ED are associated with higher mortality.11 12 However, readmissions have not yet been investigated based on chief complaint. Also, previous symptom-based ED research has mainly focused on a limited number of chief complaints at presentation and primarily in medical (non-surgical) patients and rarely in a mixed ED population.
Therefore, the primary aim of this study was to investigate 30-day mortality and 30-day readmission among all acute surgical and non-surgical ED patients using chief complaint as an exposure. Second we present data on in-hospital and 1-year mortality and 7-day readmission, and report discharge diagnoses of the 10 chief complaints with the highest 30-day mortality.
Methods
Study design and setting
This study is a single-center retrospective cohort study from the ED of Aarhus University Hospital and will be reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) criteria.
The Aarhus University Hospital serves a population of around 350 000 inhabitants and the ED has approximately 45 000 contacts a year. The ED operates as the only major trauma center and receive trauma patients from the entire region (1.2 million people). Patients with acute medical or surgical conditions can be referred to the ED round the clock either by calling the emergency medical service or by calling a general practitioner or an out-of-hours physician. Acute pediatric, obstetric and psychiatric patients are primarily referred to other departments. Patients with suspected stroke, end-stage cancer, cardiac arrest (with suspected thrombosis) or ST-Elevation Myocardial Infarction (STEMI) are referred directly to specialized units and therefore bypass the ED. Patients with suspected stroke are prehospitally conferred with a vascular team neurologist, and if stroke is still suspected and there is indication for thrombolysis or thrombectomy the patient is taken to a specialized stroke unit. Patients with suspected acute coronary syndrome receive prehospital ECG, which is then sent to a cardiologist, and if STEMI is suspected from the ECG and history patients are taken directly to the cardiac catheterization laboratory. The remaining are taken to the ED.
Patients arriving at the ED are triaged using the Danish Emergency Process Triage (DEPT) system, which is based on chief complaint-specific parameters and vital parameters (see online supplemental figure 1 for an overview of the DEPT system process).3 DEPT is the most used triage system in Denmark and is similar to other modern triage system, for example, Adaptive Process Triage, Canadian Triage and Acuity Scale, Australian Triage Scale and Manchester Triage System.4 13 The most acute patients, such as major trauma and surgical or medical emergencies, are received by coded rapid response teams and are not receiving formal DEPT triage. The initiation of the coded rapid response team is decided by the doctor (or sometimes paramedic) at the scene in conference with a senior doctor at the ED, who makes the final call. The decision is based on the Airway-Breathing-Circulation-Disability-Exposure (ABCDE) survey and vital parameters at the scene, and if the patient is highly unstable and at risk of dying within minutes to hours the rapid response team is initiated.
Supplemental material
Study population
All patients 18 years or older attending the ED at Aarhus University Hospital during July 1, 2016 through June 30, 2017 were eligible.
The following were the exclusion criteria:
Patients with a planned/elective visit to the ED.
Patients assessed to have a minor injury.
Patients with no triage registered.
Patients registered with more than one specific chief complaint at the same time.
The most acute patients, such as major trauma and surgical and medical emergencies, are received by the coded rapid response teams and are not registered with chief complaint or triage color and are therefore excluded. Included patients were followed up 1 year from the beginning of their first contact to the ED (index contact) using the civil registration number given to all Danish citizens. Repeated ED visits in the follow-up period were regarded as separate contacts.
Exposure
This study uses chief complaint as an exposure. The chief complaint is defined by the specific contact card assigned by the triaging nurse on arrival (figure 1). Included patients who were triaged but not assigned with a specific contact card were allocated to a “no contact reason” group.

Flow chart showing the included contacts. 1Majority of this group were patients with minor injuries who never got triage-registered. A small fraction is constituted by the most acute patients, such as major trauma and medical and surgical emergencies, who are received by the coded rapid response team and thus not triaged. Exact numbers not known. 2Index contact was defined by a patient’s first contact during the inclusion period. ED, emergency department.
Primary outcomes
The primary outcomes are 30-day mortality and 30-day readmission. Thirty-day mortality was defined as death within 30 days after the index contact start. Thirty-day readmission was defined as a patient being acutely/unplanned admitted to the hospital (hospitalized) between 12 hours and 30 days after discharge from the index contact.
Secondary outcomes
The secondary outcomes are in-hospital mortality, 1-year mortality and 7-day readmission. In-hospital mortality was defined as death during the index contact. 1-year mortality and 7-day readmission, was defined consistent with the above-mentioned conditions. Discharge diagnosis was the International Classification of Disease, tenth revision (ICD-10) diagnosis registered at discharge from the hospital. Patients not being admitted were also given a discharge diagnosis.
Other variables
We defined admission as the patient being registered as an inpatient and thus hospitalized. ED revisit was defined as a new ED contact without admission, also within 12 hours and 30 days. Length of stay was defined as total time spent at the hospital during one contact.
Data source
Data were retrieved from the electronic medical record system (MidtEPJ) used in the Central Denmark Region. Vital status was retrieved from the Danish Civil Registration System.
Statistics
Mortality and readmission data are presented as cumulative number of events and cumulative event proportions with 95% CI. Univariate and multivariate logistic regression was used to estimate crude and age-adjusted and gender-adjusted ORs, respectively. For each chief complaint logistic regression analyses were made using the remaining study population as reference.
For data to be independent, only index contacts were included in the mortality and readmission analyses; furthermore, only chief complaints with more than 150 index contacts were presented in these analyses, and the remaining chief complaints were grouped as “the rest” due to small sample size and lack of statistical power. Significance level was set at 0.05. Continuous variables were reported as median and categorical variables as proportion in percentage. Stata V.15 (Stata, College Station, TX, USA) was used for data management and statistical analysis.
Results
Study population and patient characteristics
During the study period 41 470 contacts were registered at the ED. A total of 19 325 (47%) were included in the study (figure 1). Hereof there were 15 369 index contacts, defined by a patient’s first contact during the inclusion period. Thus, 22 145 (53%) contacts were excluded: 2377 (6%) elective contacts, 10 346 (25%) with minor injuries, 7960 (19%) not registered with triage color and 1462 (2.5%) assigned with two different chief complaints. Among the patients who received two chief complaints, the most frequent chief complaints were head and face symptoms (318), extremity injury (261) and dyspnea (211).
Patient characteristics and the distribution of chief complaints are shown in table 1.
Patient characteristics and distribution of chief complaints, ranked by prevalence
Mortality
For mortality analysis 317 foreign index contacts were excluded due to lack of follow-up and a total of 15 052 index contacts were analyzed (table 2).
Mortality analysis showing chief complaints with more than 150 index contacts, ranked by 30-day mortality (primary outcome)
The overall 30-day mortality was 3.0% (95% CI 2.7% to 3.3%). It is apparent from the table that mortality differed significantly among the chief complaints. Seven chief complaints stood out with a 30-day mortality of 6% or more, with altered level of consciousness (ALOC) and dyspnea having the highest at 8.4% (95% CI 5.6 to 11.9) and 8.0% (95% CI 6.5 to 9.7), respectively. In addition, focal neurological symptoms, nausea, vomiting and diarrhea, no contact reason, gastrointestinal (GI) bleeding, and unwell were also among the seven chief complaints with the highest mortality.
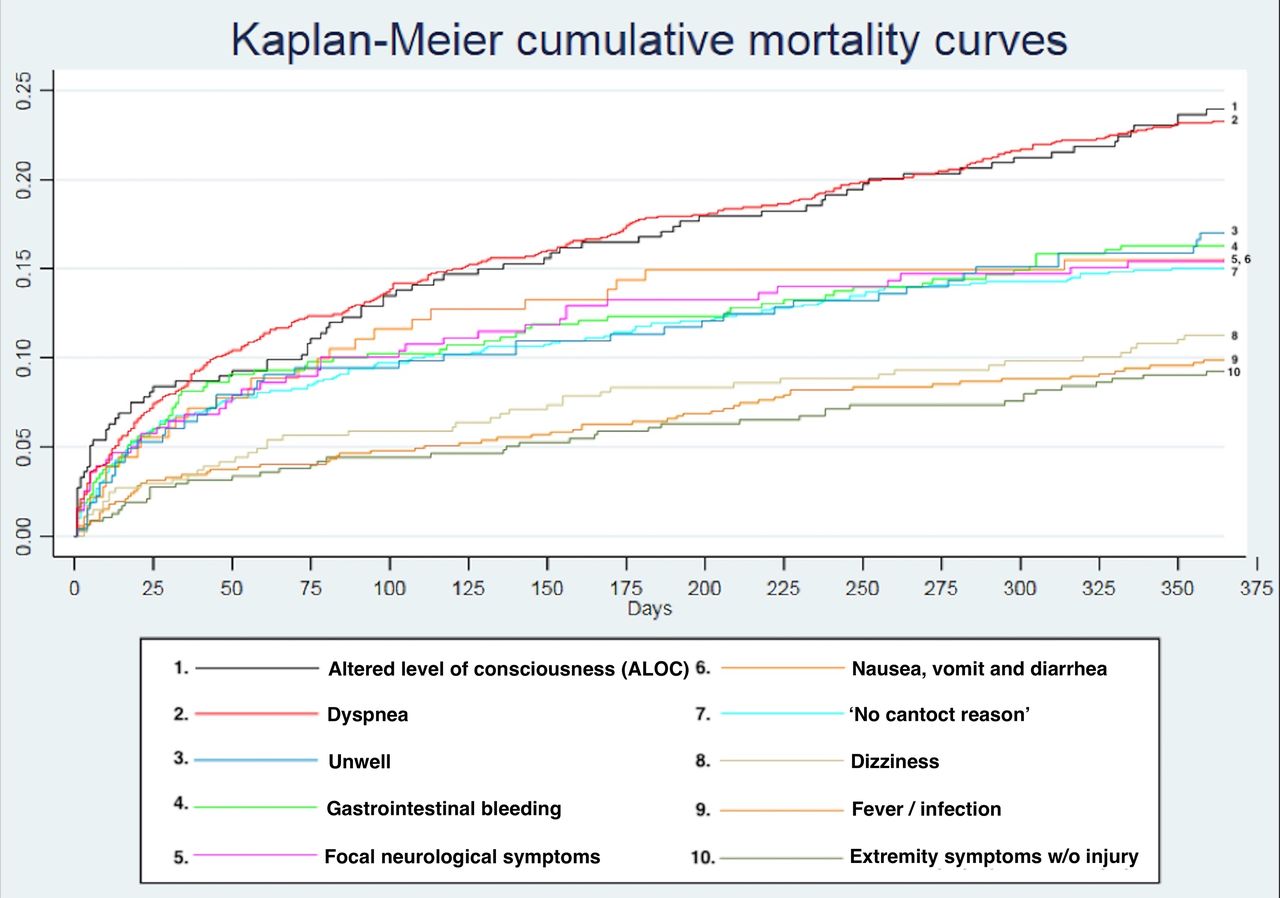
Before adjustments, patients with any of the seven chief complaints had significantly higher odds of dying within 30 days; however, after adjusting for age and gender, only patients with no contact reason (OR 2.2, 95% CI 1.7 to 3.0), dyspnea (OR 2.1, 95% CI 1.6 to 2.6), ALOC (OR 2.0, 95% CI 1.3 to 3.1) and GI bleeding (OR 1.7, 95% CI 1.1 to 2.6) had significantly higher odds of dying, each complaint compared with the rest of the study population. Similar tendencies were seen when looking at in-hospital and 1-year mortality, and differences in mortality became even clearer over time, with ALOC and dyspnea having a prominently higher mortality after 1 year (figure 2).
{kind=link}
{kind=link}
Kaplan-Meier cumulative mortality curves showing the 1-year cumulative mortality for the 10 chief complaints with the highest 30-day mortality.
Chest pain had the lowest 30-day mortality of the shown groups, with only 0.4% (95% CI 0.1 to 1.0) dead within 30 days and an adjusted OR of 0.1 (95% CI 0.1 to 0.4).
Readmission
For readmission analysis another 213 index contacts were excluded due to in-hospital death and a total of 14 839 index contacts were analyzed (table 3).
Readmission and revisit analysis showing chief complaints with more than 150 index contacts, ranked by 30-day readmission (primary outcome)
Overall, 6.5% (CI 6.1 to 6.9) were readmitted and 6.4% had an ED revisit without admission within 30 days. As for mortality, the 30-day readmission differed significantly among the chief complaints. Five chief complaints had a 30-day readmission of more than 10%, with fever/infection having the highest at 11.7% (95% CI 9.4 to 14.4), followed by dyspnea (11.2%, 95% CI 9.4 to 13.2), nausea, vomiting and diarrhea (10.8%, 95% CI 6.6 to 16.3), and abdominal symptoms (10.2%, 95% CI 8.7 to 11.8).
After adjustment, the highest odds of being readmitted within 30 days were seen in abdominal symptoms (2.0, 95% CI 1.7 to 2.4), fever/infection (1.9, 95% CI 1.4 to 2.4), skin and mucosal symptoms (1.8, 95% CI 1.1 to 2.9) and dyspnea (1.7, 95% CI 1.4 to 2.0).
Diagnoses
Table 4 illustrates that the 10 chief complaints with the highest 30-day mortality had various discharge diagnoses. Moreover, it shows that all chief complaints except GI bleeding had discharge diagnoses within each of the 10 most common ICD-10 chapters.
Distribution of discharge diagnoses grouped by the 10 most common International Classification of Disease, tenth revision (ICD-10) chapters, among the 10 chief complaints with the highest 30-day mortality
Furthermore, it stands out in the table that R-diagnoses (symptoms, signs, abnormal results of clinical or other investigative procedures, and ill-defined conditions regarding which no diagnosis classifiable elsewhere is recorded, eg, dyspnea and chest pain) were given to more than 15% of the patients at discharge within all of the shown chief complaints, except fever/infection and extremity symptoms without injury.
Discussion
This study presents data on mortality and readmission among different chief complaints presented to the ED. We found that ALOC, dyspnea and GI bleeding had the highest 30-day mortality, and fever/infection, dyspnea, and nausea, vomiting and diarrhea had the highest 30-day readmission. Dyspnea was very frequent and associated with both high mortality and readmission compared with other chief complaints. Chest pain was found to be relatively frequent and had the lowest mortality. Second, we looked at discharge diagnoses among the 10 chief complaints with the highest 30-day mortality and found that each chief complaint had various discharge diagnoses across the ICD-10 chapters, with the unspecific R-diagnoses frequently represented.
In the present study, the overall 30-day mortality was 3% and differed significantly among the chief complaints, which is in line with Nielsen et al10 in a similar study including medical ED patients. Moreover, we found an overall 30-day readmission of 6.5%, which also differed significantly among the chief complaints. Previous studies have mainly focused on readmission based on discharge diagnosis14 15; however, few studies have described short-term readmission/revisit in the ED,16 but the definitions of “readmission” and “revisit” differ and are often used interchangeably, making comparison difficult. Furthermore, organization of the health system also plays a major role in terms of readmission.
ALOC had the highest 30-day mortality (8.4%, OR=2.0). This chief complaint is not included in previous studies comparing ED chief complaints; however, this finding is supported by Völk et al, who found an in-hospital mortality of 10% among patients presenting to the ED with ALOC. The higher mortality found by Völk et al17 may be explained by only including unknown reasons for ALOC. In the present study, ALOC was not one of the most common chief complaints and only represented 2.6% of the study population. In addition, it was not associated with a significantly higher readmission. ALOC is acknowledged as an unspecific but critical condition associated with various causes, for example, intoxication, trauma and vascular emergencies.18 Correspondingly we found a diverse distribution of discharge diagnoses among patients with ALOC; however, the unspecific R-diagnoses were most used (21.5%).
Unwell is also an unspecific complaint, and interestingly we found a relatively high mortality (6.0%) in this group as well, but not significantly higher after adjusting for age and gender. Like ALOC, unwell had a diverse distribution of discharge diagnoses, with 30.2% being unspecific R-diagnoses. These findings indicate that unspecific complaints are difficult to diagnose and have a high mortality, corresponding to the findings by Nemec et al19 in an ED study investigating unspecific complaints. Thus, further research and development of risk stratification tools is needed to identify patients at high risk of presenting with these unspecific complaints.
Dyspnea had the second highest 30-day mortality (8.0%, OR=2.1) in the present study. Furthermore, it was very prevalent (8.4%) and had significantly higher 30-day readmission (11.2%, OR=1.7). Patients presenting to the ED with dyspnea have previously been found to have high mortality compared with other chief complaints in the ED, both long term and short term6–10; however, the high 30-day readmission is a new finding. This suggests that patients with dyspnea in the ED are very frequent and at higher risk of adverse outcomes, calling for increased awareness. Moreover, they represent a heterogenous group with various diagnoses and needs and thus remain a challenge to the ED physician.20 21 Further studies are needed to evaluate the diagnostic workup and initial treatment and to identify prognostic factors. Moreover, standardized algorithm and risk stratification tool are advisable to quickly identify patients with dyspnea at high risk.22
GI bleeding was the “surgical complaint” found to have the highest 30-day mortality (6.7%, OR=1.7). Likewise, previous studies have reported high mortality among this patient group, with an in-hospital mortality of 7% to 8%.23 Furthermore, GI bleeding had the strongest association with a specific ICD-10 main chapter (61.2%, K - diseases of the digestive tract). Acute management of GI bleeding is very important and the challenge in the ED is to determine if intervention is needed, for example, endoscopy, transfusion and surgery.24
In the present study, we found chest pain to be less prevalent (5.7%) and with a surprisingly low mortality compared with other European ED studies.6–10 However, the low mortality corresponds to what was found in a study by Nielsen et al10 from another Danish ED. These findings can be explained by a common practice in Denmark, where all patients with STEMI and cardiac arrest are referred directly to the cardiac catheterization laboratory from the prehospital area, thereby bypassing the ED. This finding also indicates that prehospital visitation of patients with chest pain is effective.
Fever/infection, nausea, vomiting and diarrhea, and abdominal symptoms, together with dyspnea, had the highest 30-day readmission, all at more than 10%. Whether some of these readmissions were preventable is unknown; however, it is known that preventable factors such as too early discharge can lead to acute readmissions.25 Identifying patients at high risk of readmission is important to determine which patients can be sent home safely and which cannot. This could potentially increase patient flow, without further risk to the patient.
Among the 10 chief complaints with the highest 30-day mortality, we found that they all had a wide distribution of discharge diagnoses. This suggests that chief complaint offers information independent of diagnosis and is also available in a timely manner to the ED physician compared with a final diagnosis, which is one of the reasons why symptom-based research is essential to emergency medicine.
The fact that chief complaint is associated with multiple final diagnoses also emphasizes the importance of not thinking too narrow in terms of differential diagnoses, which underlines the challenging essence of emergency medicine: to initiate acute treatment and diagnostic workup to “convert” a patient’s symptoms to a correct diagnosis, to assure the best treatment.
Furthermore, we found that unspecific diagnoses (majorly R-diagnoses and less frequent Z-diagnoses) were often used, which means that many ED patients leave the hospital without a specific diagnosis. This may be explained by the patients being stable and discharged to further diagnostic workup electively or at the general practitioner. Another contributing factor could be the patients getting well spontaneously and therefore discharged without specific diagnosis. However, the large proportion of patients without organ-specific or cause-specific diagnosis is inappropriate and underlines the need to improve the diagnostic process. More research is needed to understand the link between discharge diagnoses and chief complaints.
The 1-year follow-up revealed that ALOC and dyspnea stood out with a mortality of 24% and 23.4% (both with adjusted OR of 2.1). These are alarming numbers, but are not new. A Danish study of emergency medical services patients also found impaired consciousness and dyspnea to have the highest mortality, with a 1-year mortality of 54.7% in “unconscious and cardiac arrest” patients and a 1-year mortality of 27.7% in patients with dyspnea.26 This suggests that these two chief complaints should be considered extremely high risk, both short and long term, and there is a potential for outcome improvement in these patients.
A major strength of this study is the large study population with complete follow-up due to the Danish Civil Registration System. All adult patients visiting the ED during the inclusion period were eligible, thus minimizing selection bias. Moreover, we included patients during a whole year and thereby avoided bias from seasonal variance.
The study has some limitations. First, we excluded 7960 contacts not registered with a triage color. However, a review of the discharge diagnoses of these contacts revealed that the vast majority belonged to the minor injury group and thus correctly excluded. A minority of the contacts encompassed patients dying at the hospital (n=237), with the most frequent diagnoses being intracranial injury and cardiac arrest. These contacts represent the most acute patients attending the ED and are prehospitally reported as “major trauma,” “surgical or medical emergency” and received by coded rapid response teams and thus not triaged at arrival. The exclusion of the most acute patients causes selection bias and will most likely underestimate the mortality rates, especially in the chest pain group, the ALOC group and the focal neurological symptoms group.
Second, the classification of chief complaint might be imprecise and thereby add random error. Many patients present with several complaints9 27 and it may be difficult to determine the most appropriate chief complaint in an acute situation. Furthermore, in case of several symptoms, there are, to date, no guidelines on how to prioritize symptoms, thus placing the decision on the triaging nurse, which implies a risk to the patient of being assigned a misleading chief complaint—a potential source of misclassification. Also, chief complaint combinations/interactions may be an important factor in identifying high-risk ED patients. This is not touched on in this study due to the exclusion of patients assigned with two specific chief complaints.28 This is an area of interest in future research.
Third, we included a group with no chief complaint registered. The discharge diagnoses of this group indicated that it was a heterogenous group of medical and surgical patients and with different triage colors. The reason why these patients were not given a chief complaint is unknown. One possible explanation could be that the patients’ presenting symptoms were unspecific and none of the chief complaints predefined by DEPT fitted. However, lack of registration of chief complaint is another possible explanation and it is therefore another potential source of misclassification.
This is a single-center study and the result cannot therefore by definition be directly generalized to other EDs. However, the study population was comparable with other ED studies in terms of age, gender, admission rate and mortality,6–10 indicating that the results can be generalizable. This said, it is important to notice that the generalizability is limited due to the Danish set-up where patients suspected of cardiac arrest due to thrombosis, STEMI or stroke are not seen in the ED, but directly sent to a specialized department.
This study may be used as an impetus to more ED symptom-based research in general. As discussed, identification of risk factors among the chief complaints as well as the link between discharge diagnoses and chief complaint, and even combinations/interactions of chief complaints, is an essential area to focus future research on. This knowledge may contribute to the development or improvement of standardized ED algorithms and risk stratification tools, potentially improving patient outcomes.
Conclusion
This study shows that chief complaint is associated with 30-day mortality and readmission in a mixed ED population. Patients with dyspnea stood out as very frequent with high mortality and readmission. The unspecific complaints ALOC and unwell also had high mortality. GI bleeding was the surgical complaint with the highest mortality. Patients with fever/infection, nausea, vomiting and diarrhea, and abdominal symptoms were more often readmitted within 30 days. Second, we found that ALOC and dyspnea stood out in terms of a high 1-year mortality at 24% and 23%, respectively. Overall, chief complaint at presentation carries important information that may assist in improving initial diagnostic workup and treatment and patient flow in the ED.
Data availability statement
Data are available upon reasonable request. Data are stored on a local server. The owner of the data is Professor Hans Kirkegaard (hans.kirkegaard@clin.au.dk). Anonymized data can be accessed upon request. Raw data, cleaned data and cleaning protocols are available.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Danish Patient Safety Authority (case no: 3-3013-2615) and the Danish Data Protection Agency (case no: 1-16-02-371-18). According to Danish law, approval from the regional ethics committee was not required.
Acknowledgments
The authors gratefully acknowledge the contributions of Anne Aavad Mortensen for data management and the data office at Aarhus University Hospital, with special thanks to Erik Soeters, data consultant.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Design of the work: all authors. Data collection: SFS and SHO. Data analysis and interpretation: SFS. Drafting the article: SFS. Critical revision of the article: all authors. Final approval of the version to be published: all authors. Guarantor SFS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.