Article Text

Abstract
Background Rib fractures are common among trauma patients and may result in significant morbidity and mortality. There are numerous treatment options, but ideal management is unclear. Delivery of local anesthetic via an analgesia catheter for continuous intercostal nerve blockade offers an attractive potential option for management of patients with rib fractures.
Methods We performed a single-center, retrospective case–control analysis of trauma patients with multiple rib fractures from 2016 to 2018, comparing patients managed with continuous intercostal nerve blockade with standard care. Matching was performed in a 2:1 ratio by Injury Severity Score, age, and gender. Respiratory morbidity potentially secondary to rib fractures, including unplanned intubation, failure of extubation, need for tracheostomy, pneumonia, or mortality, were all identified and included. Potential complications due to catheter insertion were identified to be recorded. The primary outcome of interest was 30-day hospital-free days.
Results Nine hundred and thirty-three patients were eligible for analysis, with 48 managed using intercostal blockade compared with 96 matching controls. No complications of intercostal blockade were identified during the study period. Controls demonstrated fewer rib fractures (6.60±4.11 vs. 9.3±3.73, p=0.001) and fewer flail segments (0.8±1.76 vs. 2.0±2.94, p=0.02). Those managed with intercostal blockade demonstrated significantly more 30-day hospital-free days (15.9±6.43 vs. 13.2±9.94, p=0.048), less incidence of pneumonia (4.2% vs. 16.7%, p=0.03), and lower hospital mortality (2.1% vs. 13.5%, p=0.03). When adjusting for number of rib fractures and number of flail segments, use of continuous intercostal nerve blockade was significantly associated with lower hospital mortality (OR 0.10; 95% CI 0.01 to 0.91), pneumonia (OR 0.15; 95% CI 0.03 to 0.76), or need for tracheostomy (OR 0.23; 95% CI 0.06 to 0.83).
Discussion The addition of continuous intercostal nerve blockade may help to improve outcomes in patients with multiple rib fractures compared with standard care alone.
Level of evidence Therapeutic/care management; level IV.
- rib fractures
- nerve block
- analgesics
- opioid
Data availability statement
No data are available. Permission for data sharing not requested when obtaining IRB approval for this project.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Rib fractures are among the most commonly encountered injuries in the trauma population. Poorly controlled pain, altered respiratory mechanics, and underlying pulmonary injury combine to present the clinician with complex management decisions. Failure to control pain can result in low tidal volume ventilation, inadequate clearance of bronchial secretions, obstructive atelectasis, and progressive respiratory dysfunction. As a result, multiple rib fractures are associated with significant increase in length of stay and ventilator requirements.1 Furthermore, each additional rib fracture has been correlated with subsequent increase in mortality, with approximately 10% of all patients suffering death prior to hospital discharge.2 With appropriate analgesia at the forefront of management, a multitude of techniques and approaches have been investigated. Most treatment algorithms employ a combination of narcotic and non-narcotic analgesia, but opioids typically serve as the bedrock and carry many negative side effects and potential dependency issues.
Management of multiple rib fractures should seek to maintain normal respiratory mechanics and pulmonary toilet through adequate analgesia.3 Epidural analgesia is often a recommended adjunct in the management of multiple rib fractures.4 5 However, its use may be limited in this population due to a variety of reasons, including need for interruption of thromboembolic chemoprophylaxis or lack of trained personnel available for catheter placement.6 An alternative to epidural analgesia is subparaspinous continuous intercostal nerve blockade (CINB) via an extrathoracic catheter inserted below the vertebral paraspinous muscles just above and along the ribs. In the elective setting, CINB has been shown to provide equivalent pain relief compared with thoracic epidural after thoracotomy.6 Specific to trauma patients, prospective studies have demonstrated equivocal or even superior pain control between thoracic epidural and thoracic paravertebral infusions of local anesthetic following multiple rib fractures.7 8
There is limited information available regarding the impact that management with CINB has on outcomes among trauma patients. Although CINB may improve pain scores and lung volumes among trauma patients, further information is still needed to determine if this limits associated morbidity and mortality in patients with multiple rib fractures. We hypothesized that use of these catheters in the treatment of trauma patients with multiple rib fractures will result in improved outcomes and increased 30-day hospital-free days compared with patients undergoing standard management.
Methods
The trauma registry at the University of Alabama at Birmingham Medical Center (UABMC) was queried for patients with multiple rib fractures from January 1, 2016 to February 1, 2018. UABMC is a 908-bed tertiary care facility for the region and serves as an American College of Surgeons-verified level I trauma center.
We performed a retrospective case–control study for patients with multiple rib fractures managed with CINB via analgesia catheter with standard care (CATH) compared with patients with standard care alone (STD). The study design featured 2:1 case–control matching using nearest neighbor matching according to Injury Severity Score (±1), then age, then gender. A larger control cohort was identified given the lack of random patient selection for the case cohort. Patients with multiple rib fractures were identified using International Classification of Diseases-10 codes S22.41XA, S22.42XA, S22.43XA, and S22.49XA. Exclusion criteria included age <18 years old, death within 48 hours, or less than two rib fractures.
Continuous intercostal analgesia was delivered via an ON-Q SilverSoaker catheter (Halyard, Alpharetta, GA), either 7.5 inches or 10 inches in length depending on the number of rib fractures. Catheter insertion was performed via a 1 mm incision made ~5 mm lateral to the spine, one rib below the most inferior rib desired to undergo nerve blockade. A tunneling device with peel-away sheath was then used to gain access below the paraspinous muscle above the ribs without entering the pleural cavity. The tunneler was then directed cephalad, palpating each rib as the tunneler was inserted further. After insertion, the tunneler was removed and the ON-Q catheter inserted through the sheath, which was then peeled away. The ON-Q catheter was then secured with adhesive strips and bandages put into place. A variable rate (1–14 cc/hour), ON-Q pump prefilled with 0.2% ropivacaine was then attached and local anesthetic instilled. Catheters remained in place for up to 5 days after placement. There were no other standards for analgesic management for either cohort, with patients managed with a mix of narcotic, non-narcotic, and topical analgesics according to provider preference.
Data regarding patient demographics, injury characteristics, and outcomes were extracted from the medical record. Fractures were further defined in terms of three anatomic sectors as recommended by the Chest Wall Injury Society.9 As previously described by Chapman et al,10 fractures were described as anterior from the insertion of the serratus anterior to the distal rib, lateral from the serratus anterior to the costal angle, and posterior from the proximal rib to the costal angle. Respiratory morbidity potentially secondary to rib fractures, including unplanned intubation, failure of extubation, need for tracheostomy, pneumonia, or mortality, were all identified and included. Potential complications due to catheter insertion were identified to be recorded, including pneumothorax, hemothorax, abscess, or cellulitis. Pneumonia was defined by culture-proven bacterial isolate from bronchoalveolar lavage with 1×105 colony forming units. Unplanned intubation was identified in patients as any intubation after admission, excluding patients who required intubation for the operating room. Failure of extubation was identified and defined as any patient who required reintubation following previous liberation from mechanical ventilation.
Variables were collected and expressed as either percentage or mean±SD. Univariate analysis was performed with χ2 and independent t-test for categorical and continuous variables, respectively. A p value less than or equal to 0.05 was identified as statistically significant. Homogeneity of group data was tested using Levene’s test for equality of variances.
Multivariate logistic regression was subsequently performed to determine the effect of continuous analgesia catheter use on the development of potential respiratory complications of multiple rib fractures. Potential covariates were selected based on the results of the univariate analyses with p<0.2. Hosmer-Lemeshow was performed to assess the goodness of fit of each model.
The primary outcome of interest was the effect of ON-Q analgesia catheter use for continuous intercostal blockade on 30-day hospital-free days. Based on our population, we estimated a required sample size of 162 patients to identify a difference of 3 hospital-free days for α=0.80. The secondary outcomes of interest included 90-day hospital-free days, intensive care unit (ICU)-free days, ventilator-free days, pneumonia incidence, need for tracheostomy, failure to extubate, need for reintubation, and hospital mortality.
Results
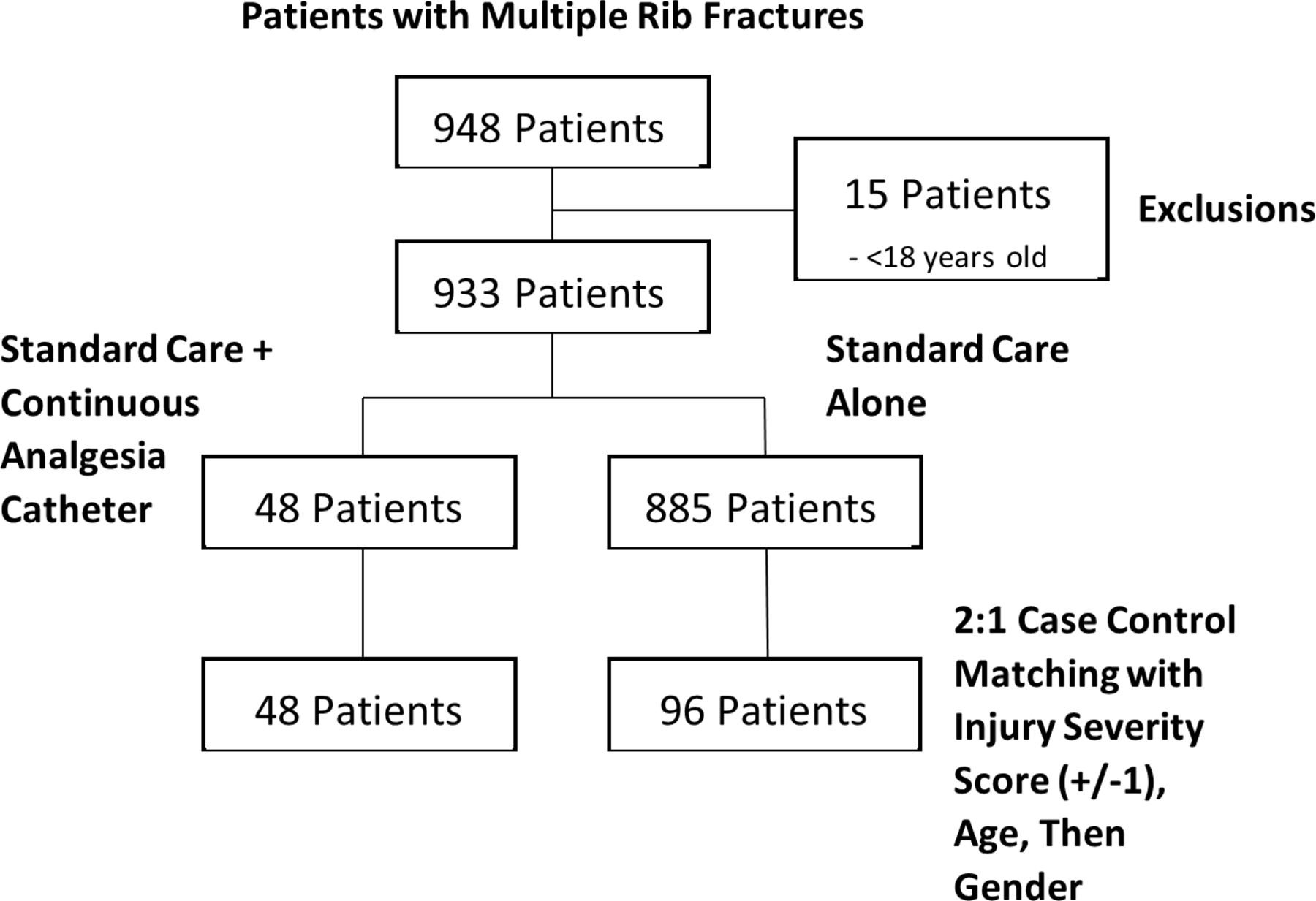
Nine hundred and forty-eight patients with multiple rib fractures were identified from the trauma registry during the study period. Fifteen were excluded by age. Of the remaining 933 patients, 48 (5.1%) were managed with continuous intercostal analgesia and included in the CATH cohort. These patients were subsequently reviewed and 96 matching controls identified and placed in the STD cohort (figure 1).

{kind=link}
CONSORT diagram for patient selection. CONSORT, Consolidated Standards of Reporting Trials.
Patients managed with continuous intercostal blockade underwent catheter placement on average after ICU day 2, with a large mean number of ribs anesthetized (table 1). No patients suffered pneumothorax, hemothorax, local cellulitis, or abscess as a result of catheter insertion. Comparing the two cohorts, both were demographically similar, consisting predominantly of middle-aged male patients with blunt traumatic injury (table 2). There was no difference in Injury Severity Score between the two groups. Similarly, there was no difference in the Abbreviated Injury Scale score for thorax (p=0.62) or abdomen (p=0.82). Patients in the CATH group suffered significantly more rib fractures (p=0.001) and more flail segments (p=0.02). Additionally, patients in the CATH cohort were more likely to undergo rib fixation (p<0.001) and tube thoracostomy (p<0.001).
Characteristics of ON-Q analgesia catheter use
Comparison of demographic and injury characteristics in patients with multiple rib fractures based on use of ON-Q catheter for continuous intercostal nerve blockade
Management with CINB resulted in significant improvement in 30-day hospital-free days compared with patients managed with standard care alone (p=0.048) (table 3). There were no differences in ICU-free or ventilator-free days between the two cohorts. Patients in the CATH cohort demonstrated significantly lower rates of pneumonia (p=0.03) and hospital mortality (p=0.03). When patients were further subdivided to compare those managed with rib fixation independent from those with medical management or CINB, those with medical management had significantly greater number of rib fractures than the CINB or rib fixation cohorts (p<0.001) (table 4). Those receiving medical therapy alone had significantly fewer 30-day hospital-free days than those with CINB (13.4±9.89 vs. 16.7±6.51, p=0.03). There were no significant differences in the outcomes of patients managed with either rib fixation or CINB. Subanalysis of patients with rib fractures with removal of all patients managed with rib fixation demonstrated similar outcomes as our previous analyses (table 5).
Comparison of outcomes in patients with multiple rib fractures based on use of ON-Q catheter for continuous intercostal nerve blockade
Comparison of patients with multiple rib fractures based on management with standard medical management, rib fixation, or ON-Q catheter for continuous intercostal nerve blockade
Comparison of outcomes in patients with multiple rib fractures based on use of ON-Q catheter for continuous intercostal nerve blockade, excluding patients with rib fixation
Comparing opioid analgesic requirements between patients in the CATH and STD cohorts, there were no significant differences in the oral morphine equivalents (OME) required for the total hospitalization (2741±1960 vs. 3429±4251, p=0.19) (table 6). Patients with six or more rib fractures required significantly less OME when managed with CATH compared with STD (2641±1990 vs. 4900±5443, p=0.01).
Comparison of opioid analgesic requirements in patients with multiple rib fractures based on use of ON-Q catheter for continuous intercostal nerve blockade
Multivariate regression modeling was performed adjusting for the total number of rib fractures and the number of flail segments. Use of continuous intercostal analgesia was significantly associated with decreased risk of hospital mortality, pneumonia, need for tracheostomy, or overall complication due to rib fractures (table 7).
OR and associated 95% CI for the association of use of continuous intercostal blockade and outcomes
Discussion
In our case–control study, we compared patients with multiple rib fractures treated with the addition of CINB with those managed with standard therapy alone. Patients treated with CINB had significantly more rib fractures and flail segments than those managed with standard therapy. Regardless, patients in the CATH cohort demonstrated increased 30-day and 90-day hospital-free days, as well as lower rates of pneumonia, hospital mortality, and overall rib fracture complications. When adjusting for possible confounding covariates, use of continuous intercostal blockade was still significantly associated with decreased odds of pneumonia, need for tracheostomy, hospital mortality, or overall rib fracture complications. Lastly, we identified that patients managed with CATH trended toward lower opioid narcotic use than those with STD management, a finding which was significant when comparing patients with six or more rib fractures.
Our study is consistent with previous works that highlight the advantages of CINB via a paraspinous catheter over other potential therapies in the management of multiple rib fractures.7 11 These findings may be explained by the advantages inherent in use of the subcutaneous, extrathoracic catheter. As in our study, no other previous work has reported any catheter-related or drug-related complication associated with ON-Q or any other subcutaneous catheter delivery system for CINB.7 8 12 13 Due to its anatomic location, catheter placement is relatively simple and straightforward and may be performed by the trauma team almost immediately following presentation. We choose to employ the ON-Q system as an immediately available alternative to epidural analgesia that could be inserted by the trauma service. Extrathoracic catheters avoid the need for intraoperative insertion, whereas avoiding the epidural space obviates concerns for concomitant injury, sympathetic-related hypotension, or coagulopathy that may accompany and delay epidural catheter placement.14 15 Overall, this may allow for earlier intervention in patients at high risk of development of complications due to their thoracic injuries and may explain the improved outcomes seen in patients in the CATH cohort.
Although our study did not examine differences in pain scores among patients in the CATH and STD cohorts, patients managed with CATH demonstrated significantly lower opioid requirements in patients with more severe injury patterns. Fewer OMEs were seen in all cohort comparisons between CATH and STD. The failure to detect a significant difference is likely due to the limited number of patients in our study. Standard analgesic management in all patients with multiple rib fractures at our institution consists of multimodal therapy with a combination of non-narcotic analgesics, muscle relaxants, and opioid analgesia. CATH is typically added to our standard maximal medical management in patients with the most severe injuries, evidenced by either poor respiratory effort by bedside spirometry or complex fracture pattern on CT. Anecdotally, the improvement in pain management is significant, with numerous patients reporting it as the most significant factor in their pain relief and outcome.
Previous studies comparing the use of CINB with other modalities have shown similar findings with regard to pain control.7 8 11 However, studies of individual, non-CINB show only transient improvement in pain scores without any difference in outcomes.16 17 The difference is likely secondary to the method of intercostal nerve blockade. Non-catheter-based intercostal nerve blockade requires drug delivery via needle directly into the intercostal muscle adjacent to the neurovascular bundle, resulting in anesthetization of that corresponding nerve.18 This differs from the extrathoracic, subcutaneous, catheter-based approach for CINB. Rather than local nerve blockade, extrathoracic catheter CINB may actually act over a wider tissue plane. Recent cadaveric examination demonstrated that the paraspinous, subrhomboidal space into which the ON-Q catheter is inserted actually is a large, continuous space below the erector spinae, rhomboid, serratus, latissimus dorsi, and upper external obliques, encompassing the dorsal rami of the thoracic intercostal nerves and the lateral cutaneous branches of the thoracic intercostal nerves.12 Local anesthesia may therefore spread via the catheter to have a more diffuse effect and result in improved analgesia throughout the affected hemithorax, possibly explaining why patients managed with CINB demonstrate improved outcomes rather than those treated with only intercostal nerve blockage.
Our study is limited by the retrospective nature of its design. It is limited by patient number to detect significant differences in several of our outcome measurements. Further it suffers from possible selection bias given the lack of specific indication for ON-Q placement. We attempted to compensate for this through our multivariate analysis in which we adjusted for the number of rib fractures and flail segments. However, further study is needed to prospectively evaluate the use of CINB with the ON-Q catheter in comparison with multimodal analgesia and thoracic epidural catheter use. Further studies should include larger patient populations to allow the analysis to control for additional variables, such as individual body area injury scores. Additionally, prospective use of pain intensity and opioid consumption scores may assist in better quantifying the effect of ON-Q.
Given that multiple rib fractures are among the most common injury patterns encountered while also carrying major implications in terms of morbidity and mortality, our study carries major implications given the improvement in outcomes. In particular, we identified that management with CINB was associated with significantly lower mortality and respiratory complications, even when controlling for the number of rib fractures and flail segments. If prospectively demonstrated, use of CINB may significantly improve the care of this large patient population.
Conclusion
CINB, via a paraspinous, subcutaneous catheter, decreases complications in patients with multiple rib fractures while also increasing hospital-free days. Multivariate analysis adjusted for number of rib fractures and number of flail segments demonstrated a significant reduction in pulmonary complications among patients managed with CINB.
Data availability statement
No data are available. Permission for data sharing not requested when obtaining IRB approval for this project.
Ethics statements
Ethics approval
Approval from the Institutional Review Board of the University of Alabama at Birmingham (IRB-170414001) was gained prior to initiation of this study.
References
Footnotes
Contributors RU, PH, and PB were responsible for study design, article development, and critical revision. RU and PH were responsible for data collection and analysis. JDK was responsible for article development and critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.