Article Text

Statistics from Altmetric.com
History
A 24-year-old man presented to the trauma center with obvious distress and a gunshot wound above the left nipple.
Examination
The patient was speaking but was confused and diaphoretic with a systolic blood pressure of 80 mm Hg, heart rate of 110 beats per minute and a respiratory rate of 20 breaths per minute. He had a single gunshot wound 5 cm superior to the left nipple and decreased breath sounds over the left hemithorax.
Management
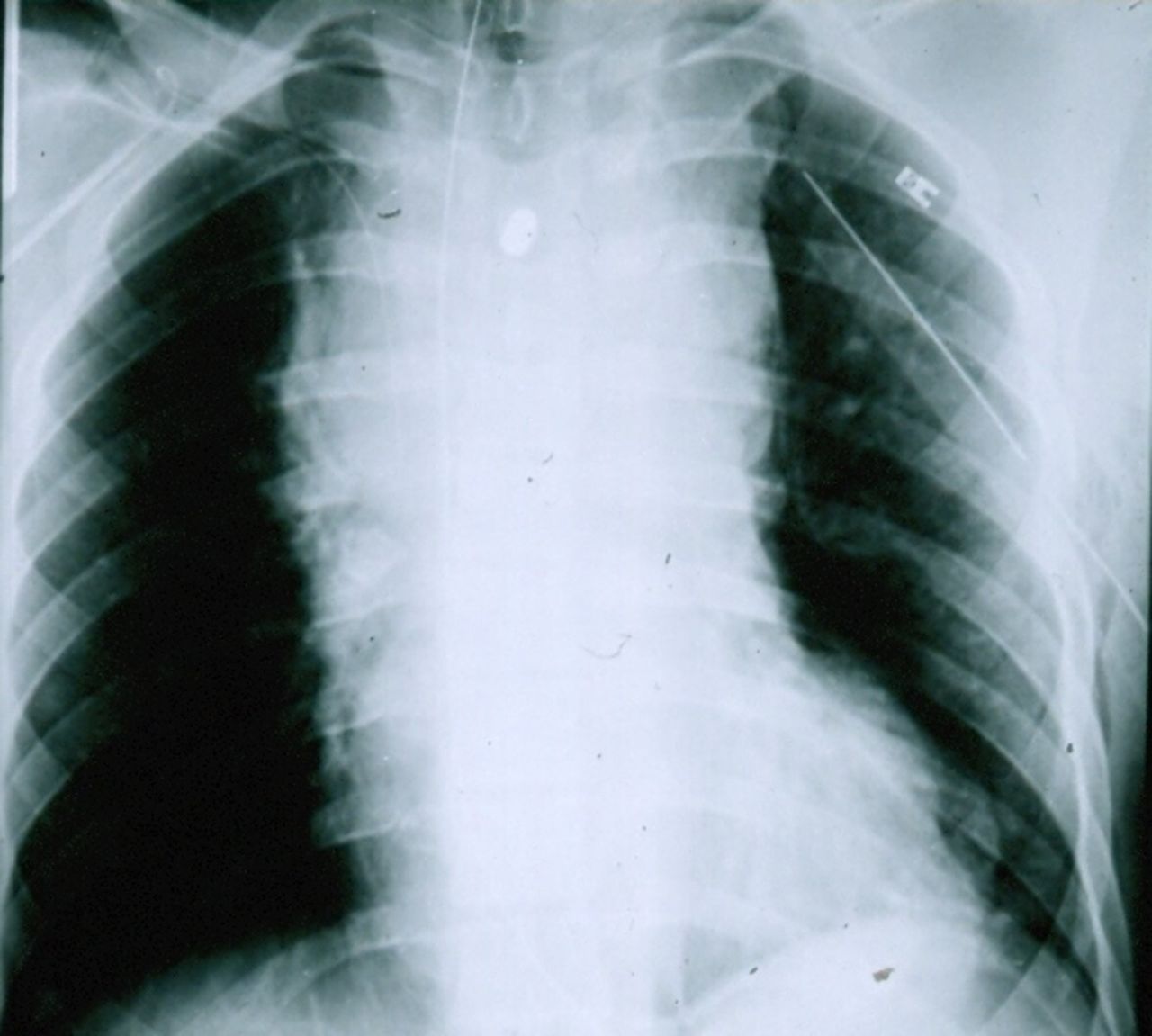
After blood was drawn for type and cross-match, two #14 gauge intravenous catheters were inserted into the antecubital veins and lactated Ringer’s infusions were started. A surgeon-performed extended ultrasound focused assessment for the sonographic evaluation of the trauma patient (FAST) examination documented the absence of pleural sliding and of a comet tail artifact in the left hemithorax. Also, there was no pericardial fluid noted. A 36-Fr thoracostomy tube was inserted through the left fifth intercostal space, and a rush of air from the left hemithorax was noted. A stat chest X-ray was performed (figure 1).

{kind=link}
Gunshot wound to superior mediastinum injured posterior left common carotid artery at its origin on the transverse arch, left innominate vein and distal innominate artery. Patient had a contained hematoma and was transported to the operating room. From Feliciano.14
Question
The patient’s systolic blood pressure remained at 80 mm Hg. In addition to intubation and transfusion of blood, your choice for the next step in management would be:
emergent left anterolateral thoracotomy.
contact the endovascular specialist.
CT aortogram with contrast.
median sternotomy in the operating room.
Management
The surgical team felt that the contained hematoma in the superior mediastinum reflected an injury to a great vessel. A median sternotomy was performed, and three separate vascular injuries were noted as follows:
4 mm perforation of the posterior left common carotid artery at its origin off the transverse arch.
6 mm perforation of superior edge of crossover left innominate vein.
large hematoma surrounding the innominate artery near its bifurcation.
At this point, the surgical team was reminded that the cardiothoracic surgeon on call lived 25 miles away.
Question
Vascular clamps were placed around the large hematoma in the innominate artery; however, the distal clamp partially occluded the origin of the right common carotid artery. Your next step in management would be:
ligation of left common carotid and innominate arteries and left innominate vein.
reimplant left common carotid artery into aortic arch, ligate innominate artery and left innominate vein.
repair left common carotid artery and left innominate vein and initiate innominate artery bypass repair.
repair left innominate vein and left common carotid artery and ligate innominate artery.
Management
The cardiothoracic surgeon on call was asked to come to the operating room. The assistant surgeon placed a finger over the hole in the posterior left common carotid artery at the aortic arch, while the surgeon performed a venorrhaphy of the left innominate vein with 5-0 polypropylene suture. The surgeon then used a double-armed 5-0 polypropylene suture to place a ‘U stitch’ around the posterior defect in the left common carotid artery, and bleeding was controlled.
Because of the large hematoma in the distal innominate artery, a major injury was presumed and a bypass around the injury was initiated. This was the same open technique developed for blunt injuries of the innominate artery at its origin prior to the development of endovascular stents and stent grafts. First, a large Satinsky (Victor P Satinsky, 1912–1997) side-biting vascular clamp was placed on the lateral ascending aorta proximal to the origin of the innominate artery. An aortotomy over the clamp was made, and an end-to-side anastomosis between a preclotted knitted 8 mm Dacron graft and the ascending aorta was completed with 4-0 polypropylene suture. At this point, the cardiothoracic surgeon arrived in the operating room. The large vascular clamp on the distal innominate artery at its bifurcation was removed. Slightly angled vascular clamps were then placed on the origins of the right common carotid and subclavian arteries.
The distal innominate artery beyond the previously placed vascular clamp was divided, and the injured area was resected. The distal end of the 8 mm Dacron graft was then sewn with no tension to a cuff of the distal innominate artery using a continuous 5-0 polypropylene suture. Prior to completion of the suture line, temporary back-bleeding from the right common carotid and subclavian arteries was allowed by removal of the angled vascular clamps. A vascular clamp was reapplied to the origin of the right common carotid artery as the polypropylene suture was pulled tight, and flow was restored to the right subclavian artery. After 10 s, the clamp on the right common carotid artery was removed as well. The final step in the operation was to undersew the origin of the innominate artery on the arch with a 4-0 polypropylene suture and excise the entire innominate artery.
The patient’s postoperative course was surprisingly uneventful until the fourth postoperative day when he had a grand mal seizure. A CT of the brain and a vascular imaging study encompassing the thoracic aorta and great vessels were both normal. Antiseizure medication and a daily 81 mg aspirin tablet were initiated for 3 months. The patient had no further complications and was well when examined on short-term follow-up in the outpatient clinic.
Discussion
Only 10%–15% of patients with penetrating wounds of the chest needed a thoracotomy or median sternotomy in the pre-endovascular era. The major indications have always been tamponade or hemorrhage from a cardiac wound, hemorrhage from or occlusion of a wound to a great vessel or hemorrhage from the lung.1
Cardiothoracic surgeons rarely take in-house call in level I or level II trauma centers in the USA. Therefore, patients with penetrating thoracic wounds most commonly undergo emergent or urgent operations by in-house trauma, acute care or general surgery teams. This is logistically necessary and clinically sound as operative techniques to repair 97%–99% of cardiac injuries and all wounds of the great vessels and lungs are well-known to well-trained surgeons in all these groups.2 Also, new partners about to start trauma call are encouraged to first read an atlas of thoracic surgery as well as the trauma textbook chapters on thoracic, cardiac, thoracic vascular and pulmonary injuries and operations.3
There are three different presentations for patients arriving with penetrating wounds to the thoracic outlet. First, there are patients who are exsanguinating into a pleural cavity, have fluid (blood) on an extended-FAST examination and do not respond to the transfusion of blood. Second, as in the patient described, there are hypotensive patients who present with a contained hematoma in the superior mediastinum, superior extrapleural area or the supraclavicular area on an admission chest X-ray. Third, there are hemodynamically stable patients who present with a hematoma in the same areas or with a ‘normal’ chest X-ray despite the presence of a missile or track of a missile through the superior mediastinum, supraclavicular space, or lower neck.
The operative approach with suspected or documented wounds to the great vessels will depend on presentation. Profoundly hypotensive patients in the first group should have a unilateral or bilateral thoracotomy in the emergency center.4 A unilateral thoracotomy is appropriate for a wound to the left hemithorax as it often allows the experienced surgeon to control the source of hemorrhage, perform internal cardiac massage and cross-clamp the descending thoracic aorta. With a wound to the right hemithorax, the addition of a left anterolateral thoracotomy allows for better exposure for the inexperienced surgeon and, once again, for cross-clamping of the descending thoracic aorta.
The role of resuscitative endovascular balloon occlusion of the aorta (REBOA) in such patients remains controversial.5 This is because inflation of the balloon in the thoracic aorta distal to a wound in a proximal great vessel is presumed to increase hemorrhage. Recent data from Ordoñez et al in Cali, Colombia, however, have demonstrated success with insertion of a REBOA device in patients with penetrating and blunt thoracic trauma.6 7 The caveat is that the patient is immediately transported to the operating room for insertion of the REBOA device and simultaneous thoracotomy or sternotomy for control of proximal hemorrhage.
The approach to patients in the second group will vary depending on the patient’s response to resuscitation. The patient who does not have hemodynamic improvement with transfusion should have a unilateral/bilateral thoracotomy or median sternotomy in the operating room. The choice will depend on the presumed track of the missile, the location of the hematoma on the chest X-ray, the patient’s hemodynamic status and the experience of the surgeon. Either approach (thoracotomy or median sternotomy) to an injured great vessel is time-consuming, but time of dissection to isolate the area of injury and long-term postoperative discomfort are both greater with the thoracotomy. If the patient’s hemodynamic status improves and is maintained with transfusion, transfer to radiology for a CT angiogram will allow for possible localization and consideration of an endovascular approach to vascular repair. For hemodynamically stable patients in the third group, cervicothoracic CT and CT angiogram are used to document and localize any wound or injury to a great artery.
Ligation of an injury to the crossover left innominate vein has been performed many times over the past 45 years on both trauma and cardiothoracic services. Short-term and long-term follow-up has demonstrated no sequelae other than occasional transient edema of the left upper extremity.8–10 In the patient described with multiple thoracic vascular injuries, ligation rather than repair would have been acceptable. Repair, however, was performed as bleeding from the other vascular injuries had been temporarily controlled.
The U-stitch repair performed on the posterior wound of the origin of the left common carotid artery at the transverse aortic arch was described, among others, by the late Thomas E Starzl (1926–2017) in 1974.11 The original description was for repair of posterior leaks from abdominal aorta to prosthetic graft suture lines to avoid having to detach a newly performed anastomosis. The fundamental principle is that repair is accomplished by passing the U-stitch around the palpable or visible leak or hole without ideal visualization.
Options for repair of the presumed major injury (hematoma around artery) in the distal innominate artery were either segmental resection with insertion of an interposition graft versus bypass graft as was performed. The surgical team was familiar with the step-by-step approach to repair blunt rupture of the origin of the innominate artery (case preceded endovascular stenting) as previously mentioned and chose this approach.12 13 The technique used has the same disadvantages as segmental arterial resection and insertion of an interposition graft, namely, a prolonged period of time without inflow into the right common carotid and subclavian arteries. There is little enthusiasm, however, for inserting a temporary intraluminal shunt from proximal graft to the proximal right common carotid artery as long as there is vigorous backflow from this vessel when the vascular clamp is removed.
The patient’s uneventful recovery was interrupted by a grand mal seizure on the fourth postoperative day. Diagnoses considered included the following: (1) cerebrovascular accident secondary to partial finger occlusion of the injured proximal left common carotid artery prior to U-stitch repair; (2) cerebrovascular accident secondary to prolonged occlusion of the innominate artery during bypass grafting; (3) cerebral edema secondary to ischemia from temporary occlusion of the innominate and right common carotid arteries; and (4) cerebral embolization of atheromatous material from either the left common carotid or innominate artery.
As the CT of the brain and arteriogram of the aortic arch and great vessels were both normal, the etiology is unknown.
Conclusion
Trauma, acute care or general surgeons taking in-house call in trauma centers dealing with penetrating trauma must know thoracic, cardiac, thoracic great vessel and pulmonary anatomy and techniques of operative repair.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.