Article Text

Abstract
Background Trauma is a cause of significant morbidity and mortality globally, and patients with major trauma require specialized settings for multidisciplinary care. We sought to enumerate the variability of costs of caring for patients at a Canadian level 1 trauma center.
Methods A retrospective analysis of all adult patients admitted to The Ottawa Hospital trauma service between June 2013 and June 2018 was conducted. Hospital costs and clinical data were collected. Descriptive statistics and multivariable regression analysis using generalized linear model were performed to assess cost variation with patient characteristics. Quintile-based analyses were used to characterize patients in different cost categories. Hospital costs were reported in 2018 Canadian dollars.
Results A total of 2381 admissions were identified in the 5-year cohort. The mean age of patients was 50.2 years, the mean Injury Severity Score (ISS) was 18.7, the mean Charlson Comorbidity Index (CCI) score was 0.35, and the median total cost was $10 048.54. ISS and CCI score were associated with higher costs (ISS >15; p<0.0001). The most expensive mechanisms of injury (MOIs) were those involving heavy machinery (median total cost $24 074.38), pedestrians involved in road traffic collisions ($20 965.45), patients in motor vehicle collisions ($17 621.01) and motorcycle collisions ($16 220.89), and acts of self-injury ($13 903.69). Patients who experienced in-hospital adverse events were associated with higher costs (p<0.0001). Our multivariable regression analysis showed variation in costs related to male gender, penetrating/violent MOI, ISS, adverse hospital events, CCI score, urgent admission status, hospital 1-year mortality risk score, and alternate level of care designation (p<0.05). Quintile-based analyses demonstrated clinically significant differences between the highest and lowest cost groups.
Discussion Major trauma was associated with high hospital costs. Modifiable and non-modifiable patient factors were shown to correlate with differing total hospital costs. These findings can aid in the development of funding strategies and resource allocation for this complex patient population.
Level of evidence Level III evidence for economic and value-based evaluations.
- health care costs
- health care economics and organizations
- multiple trauma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Injuries are a leading cause of morbidity and mortality worldwide and are the leading killer of Canadians 1 to 44 years of age. Despite this burden, trauma care remains largely underfunded and an underestimated cost to the healthcare system.1 2 Care of the injured patient involves a multidisciplinary team of physicians, nurses, and allied healthcare professionals involved in acute resuscitation and long-term recovery and rehabilitation. Trauma can affect people of all ages, but disproportionately affects young, working-age patients, which compounds a significant socioeconomic burden and significant cost of lifetime productivity losses.3
Canada has a publicly funded health system. Healthcare is mostly financed and delivered by the country’s provinces and territories. In 2019, the country spent 27% of its total national healthcare expenditure on inpatient care.4 With regard to in-hospital expenditure for all-cause hospitalizations, studies have shown that the majority of healthcare costs can be accounted for by a small proportion of patients, and that within these “high cost” patients 54% of costs were accumulated from a single hospitalization.5 In the pediatric population, an injury prevention study by Jessula and colleagues6 described that the median cost per hospitalization for individuals aged 0 to 19 years sustaining injury was $C3262. In pediatric trauma patients requiring urgent injury-related surgical intervention, in-hospital expenditure was substantially higher, with the median cost of hospitalization shown to be $27 571, as reported by Anantha et al.7 The complexity of trauma and the urgent need for both specialized and multidisciplinary care at trauma centers generate a patient population that leads to high in-hospital expenditures. Data regarding the hospital costs of the admitted trauma patient population are currently lacking in Canada, highlighting the need for further study.
As such, we sought to undertake a retrospective cohort study to estimate the hospital costs of admitted trauma patients. We hypothesized that specific modifiable factors, such as adverse hospital events, as well as non-modifiable factors, such as Injury Severity Score (ISS), would be associated with differences in costs incurred by trauma patients. Through an understanding of the variables which influence in-hospital expenditure within patients admitted after trauma, we intend to improve resource allocation within our trauma system.
Methods
All patients aged 18 years and over admitted to trauma services for any period of time between June 2013 and June 2018 were identified retrospectively from the prospectively collected Ottawa Hospital Data Warehouse database (table 1). A total of 46 variables, including demographic, clinical, direct, indirect, and total hospital cost data, were collected. These data were integrated with the Ottawa Trauma Registry, a local database of trauma patients maintained by The Ottawa Hospital trauma services department. We manually annotated the mechanism of injury (MOI) within each of our 2381 patients with available data regarding mechanism.
Clinical and demographic details of 2381 patients included in the cohort study
Cost data were estimated from the hospital’s perspective; only costs that were borne to The Ottawa Hospital were considered. These costs were calculated at our institution using standard methods according to the Management Information Systems guidelines outlined by the Ontario Ministry of Health.8 Direct hospital costs were calculated as costs accrued based on health service utilization for direct patient care, for example nursing costs, laboratory tests, and radiologic studies. Indirect hospital costs were costs indirectly related but essential to patient care, for example costs related to administration, housekeeping, and building maintenance. Costs are shown in 2018 Canadian dollars.
Descriptive statistics, univariate analysis, bivariate analysis and graphical illustration were performed using GraphPad Prism Version 8.0.2 software (San Diego, California, USA). Median and IQR values were calculated with Microsoft Excel software (Microsoft, USA) (table 2). A generalized linear model with a log-link function and a gamma distribution was performed using Stata Version 16 (StataCorp LLC, Texas, USA) in accordance with best practices for analysis of cost data.9–11 We used a consensus group of experts (PG, JL, MM) to select clinically meaningful variables for inclusion in multivariable regression analyses. We reduced redundancy of the included variables to increase the reliability of the regression analysis, and in doing so we reclassified specific MOIs into broad categories (table 3). We extracted cost ratio data within this analysis to define the positive or negative influence variables may exert on the data using the eform function within Stata to calculate exponential coefficient values.12 As previously described at our institution for cost analysis of patients with chronic obstructive pulmonary disease (COPD),13 quintile-based analysis was employed to elucidate important patient characteristics in the highest and lowest costing groups. Quintile-based analyses were performed using the Stata software for quintile designation and cost ratio calculations (table 4). GraphPad Prism was used to calculate p values and 95% CI to analyze patient characteristics between quintiles. Temporal correlation was assessed via Spearman correlation coefficient with two-tailed p value calculations (GraphPad Prism). Error±values are indicated as SEM.
Total costs incurred by trauma patients vary with mechanism of injury
Multivariate analysis of total cost within the data set across expert consensus-chosen variables
Total cost quintile-based analysis of the trauma cohort
We define modifiable factors as those with the potential to be avoidable and can be addressed by identifying risk before a hospital admission. These factors involve patient safety indicators (PSIs), which are elements such as ventilator-associated pneumonia, Clostridium difficile infection, and others in a manner designated by The Ottawa Hospital and which are publicly reportable to the Ministry of Health and Long Term Care of Ontario and potentially avoidable events (https://www.ottawahospital.on.ca/en/quality-safety/reporting/indicator-reporting/, accessed October 13, 2020).
Results
In-hospital cost varies with modifiable and non-modifiable patient factors in the data set
Our study included 2381 patients (table 1). The majority of the study sample were male (69%) and the mean age of patients within our cohort was 50.2±0.4 years. The mean ISS was 18.7±0.2, consistent with a level 1 trauma center which handles major trauma. The mean Charlson Comorbidity Index (CCI) score of our patient cohort was 0.35±0.02. The median total cost per encounter was $10 048.54. The results of univariate analysis suggested that high ISS and CCI score were associated with higher direct, indirect, and total costs (ISS >15; p<0.0001). Additionally, any patients who experienced any adverse in-hospital outcome, reportable as a PSI, were correlated with higher direct, indirect, and total hospital costs than those who did not experience an event (p<0.0001, one-way analysis of variance (ANOVA); figure 1). This was consistently seen in subgroups of patients who sustained a venous thromboembolic event (p<0.0001, one-way ANOVA; data not shown) or a hospital-acquired infection (p<0.0001, one-way ANOVA; data not shown).
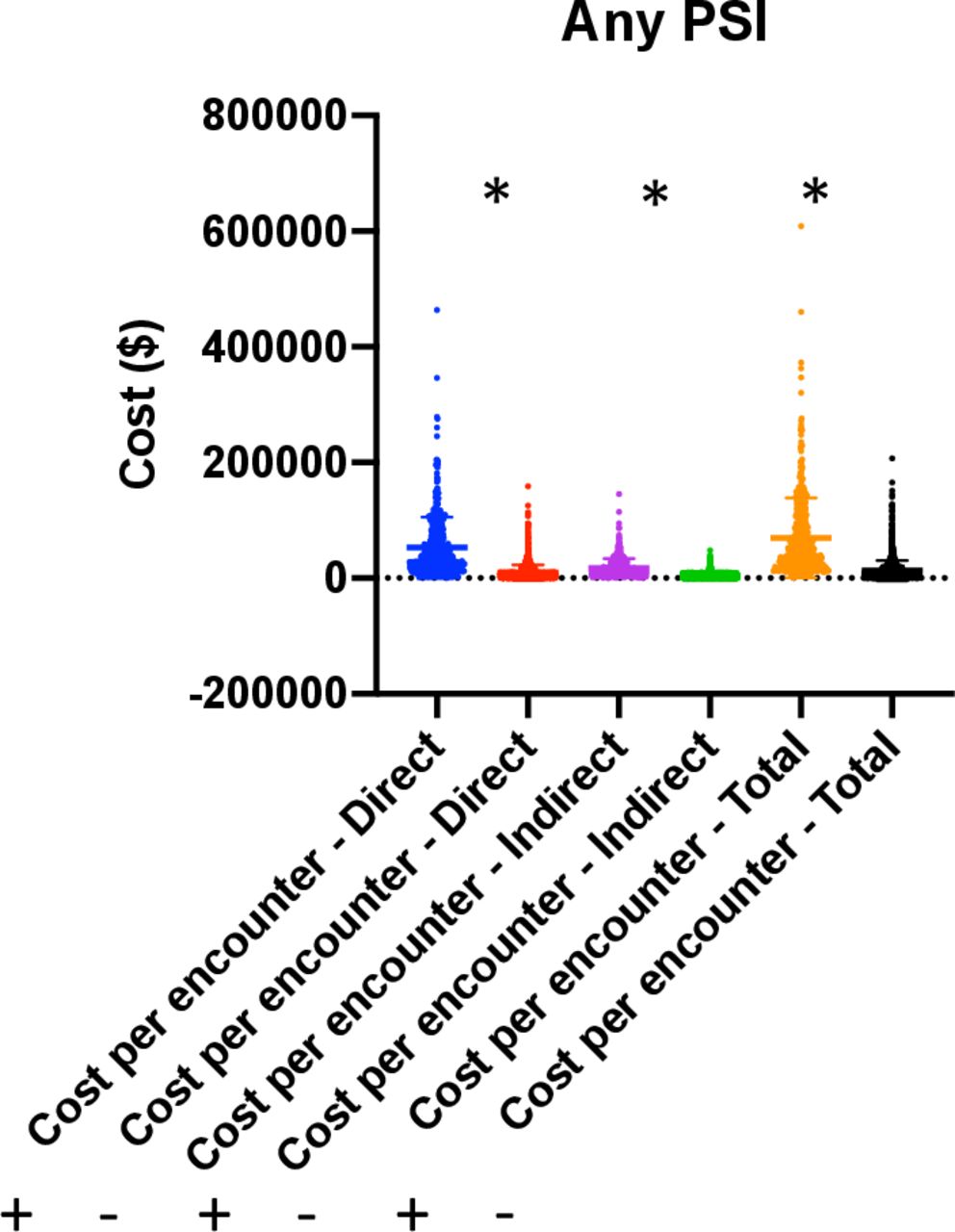
Potentially preventable adverse events correlated with higher hospital costs. Any patient safety indicator (PSI) experienced in hospital correlated with higher in-hospital direct, indirect, and total costs.
MOI was associated with differing total hospital costs in trauma patients
In assessing cost variability by MOI, patients involved in injuries related to heavy machinery (median total cost $24 074.38) and pedestrians involved in road traffic collisions (median total cost $20 965.45) (table 2) represented the most costly subgroups. Other forms of road traffic injuries formed the next most costly subgroups, with patients involved in motor vehicle collisions (all driver, passenger and rear-seated patients, n=425) representing the third most costly subgroup (median total cost $17 621.01) and motorcycle injuries the fourth ($16 220.89). Injuries related to suicide attempts or acts of self-harm constituted the fifth most costly MOI, with a median cost of $13 903.69. Stab wounds, which represented a total of 160 patients within our data set, represented the least costly MOI in terms of total cost, with a median total cost of $5614.02. All trauma mechanisms related to impairment (involving drug or alcohol intake) demonstrated a median total cost of $10 030.15.
Temporal trends in trauma patients admitted to The Ottawa Hospital between June 2013 and June 2018
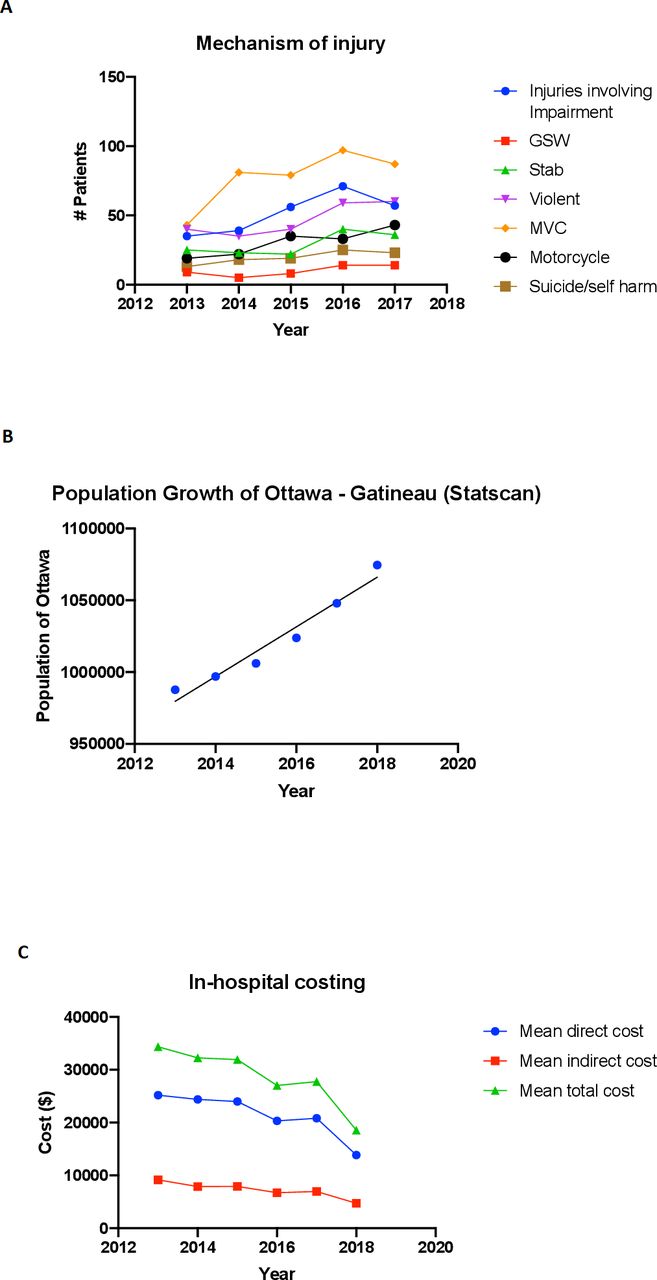
We sought to assess whether the type of trauma admissions had evolved throughout the 5-year study time span as well as trends in average hospital cost; these data are displayed in figure 2. Figure 2A demonstrates temporal trends of specific MOIs seen within our data set in absolute values. Note should be made of exclusion of 2018 data due to the study endpoint of June 2018. A general increase in all plotted mechanisms can be appreciated during this time span, indicating an enlarging absolute burden of patient admissions for all studied MOIs, which when assessing relative frequencies between 2013 and 2017 amounted to a range of increases between 50% and 125%. Injuries involving impairment, motorcycle injuries, and suicide/self-injury mechanisms demonstrated a statistically significant increase during this time span (Spearman correlation, p<0.05). This increase appeared to be in excess of the 6% population growth (figure 2B) of the Ottawa-Gatineau catchment region during this time. Figure 2C displays data assessing the mean total, direct, and indirect in-hospital costs during the 5-year study, demonstrating a decrease in all average cost categories during the course of June 2013 to June 2018. In summary, temporal analysis demonstrates that, although all cost categories on average have decreased for trauma admissions during the period of June 2013 to June 2018, the absolute burden of traumas related to all mechanisms has increased in excess of the catchment area of The Ottawa Hospital.

{kind=link}
{kind=link}
Temporal trends among injured patients admitted to The Ottawa Hospital between June 2013 and June 2018. (A) Admission to trauma services during the study period showed general increase during this time span, with significant increase seen for injuries involving impairment, motorcycle injuries, and suicide/self-injury mechanisms, demonstrating a statistically significant increase during this time span (Spearman correlation, p<0.05). (B) Population data of the Ottawa-Gatineau catchment area indicating a 6% population growth during the study period. (C) Decreased mean direct, indirect, and total costs seen during the study time period of 2013 to 2018. GSW, gunshot wound; MVC, motor vehicle collision.
Drivers of in-hospital cost identified through multivariable regression analysis of the trauma patient cohort
A multivariable regression analysis, displayed in table 3, demonstrated that ISS, CCI score, hospital 1-year mortality risk (HOMR) score, urgent admission priority, alternate level of care (ALC) status, and any PSI while in hospital were significantly associated with increased total hospital cost within our data set (cost ratios >1; p<0.05). Interestingly, however, variables such as male gender and penetrating/violent MOIs were negatively associated with total hospital cost within the data set (cost ratios <1; p<0.05).
Quintile-based analysis of the trauma cohort reveals stratified patient characteristics according to total costs
We sorted trauma patients within the cohort into quintiles in increasing order of total cost, and tabulated discrete and continuous variables of interest within these quintiles; these data are displayed in table 4. Male gender constituted the majority of each quintile as expected, with a greater composition in the lower cost quintiles. Patients having any PSI or designated with ALC status during the course of their admission were seen as constituting a greater proportion of higher cost quintiles than the lower quintiles, consistent with our univariate and multivariate analyses data in figure 1 and table 3. In accordance with their costly nature, road traffic-related injuries were more prominent within the highest cost quintiles, compared with penetrating/violent injuries within the lowest cost quintile. Continuous variables such as age, ISS, and mean total cost were analyzed with mean quintile values and associated 95% CI, displayed in table 4.
Discussion
Our retrospective cohort study of 2381 admitted trauma patients aged 18 years or older during the period from June 2013 to June 2018 identifies important independent drivers of in-hospital costs and characterized patients within the highest and lowest cost categories. Our study demonstrates that all cost categories were elevated in patients suffering from major trauma (ISS >15) and those with CCI scores of 1 to 2 or ≥2. Zuraik and colleagues1 demonstrated this previously in their assessment of cost within a Haitian cohort of patients. CCI score in addition appeared to correlate with higher costs, indicating that comorbid patients in general appeared to incur greater in-hospital expenditure. The multivariable regression analyses showed that ISS was an independent driver of cost (table 3). Level 1 trauma centers caring for patients suffering from major injuries must account for the multisystem nature of trauma, notably those sustained in road traffic collisions, and would benefit from further investment in trauma systems to facilitate the necessary diagnostic assessment, expertise involvement, and ongoing care of patients with polytrauma. Patients are often cared for in specialty trauma units or intensive care units with levels of expertise required for the multitude of injuries that can be sustained by patients involved in major trauma as reflected by ISS. Mechanisms to invest in expansion of these areas may aid in streamlining care and recovery of injured patients. Identical CCI scores can describe very different individual patients. Within our data set, we were limited in our assessment of specific comorbidities in that we did not have sufficient data to explore cardiovascular disease, preinjury anticoagulation, or other pre-existing conditions as drivers of cost. In summary, further studies assessing specific preinjury comorbidities are necessary to determine the significance that previous medical diagnosis has on the cost of the injured patient.
Knowledge of high-cost characteristics at admission would be valuable for resource allocation in the trauma setting. Previous studies by Ronksley and colleagues5 explored patients with one or more hospitalizations at The Ottawa Hospital between April 1, 2010 and March 31, 2011 and described that high-cost patients were more likely to be male, have higher comorbidity scores, and spend more days in hospital as ALC than non-high-cost patients. In a separate analysis of preadmission and postadmission factors within high-cost admissions, Rashidi and colleagues14 reviewed 5% of high-cost admissions at The Ottawa Hospital between January 1 and December 31, 2010 and reported that complications, disposition delays, clinical service delays, and inefficient clinical decision-making were contributory factors associated with higher cost. Mulpuru and colleagues13 described factors contributing to high in-hospital expenditure within a cohort of patients diagnosed with COPD as being from two general groups: patients who were severely ill and required intensive care unit care or patients with ALC designation and requiring disposition to a long-term care facility due to changes in care needs. They argue that early identification of patients with functional limitations in chronic disease is critical to reducing cost in this particular population.13 Calculated parameters at admission may represent useful tools in identifying patients in such a manner, supported by multivariable regression analysis identifying non-modifiable factors such as urgent admission priority status, ISS, CCI score, and HOMR score as associated with higher total hospital cost (table 3).
Similar to data described above by Mulpuru and colleagues13 in the cost analysis of patients with COPD, ALC designation was seen as a statistically significant, independent driver of total cost in the data set following multivariable regression analysis (table 3) and shown to constitute a large proportion of the most expensive patients within our data set (table 4). ALC designation is necessary in our institution when patients are deemed no longer acutely ill but cannot be discharged to their previous living situation given the lack of support, functional impairment, or the logistical issues associated with new level of care needs. This is consistent with the use of this designation in the rest of Ontario.15 Furthermore, our study is likely underestimating these costs as several patients may also continue their hospital course at their local hospitals as part of a repatriation process from tertiary to community settings once their course of specialty care has been completed. Endeavors to reduce this aspect of cost must be multidisciplinary in nature. Early involvement of allied health services such as physiotherapy, occupational therapy, and social worker services should be encouraged notably in older patients who sustain care-altering injuries requiring long-term interventions such as wound care, rehabilitation, or specialty consultation with geriatricians.
Studies have shown the economic and clinical impact of early mobility programs in trauma intensive care units and their impact in the reduction of patient care costs.16 Given the success of enhanced recovery after surgery (ERAS) programs at reducing cost for a plethora of surgical procedures,17–19 a similar approach can be explored for enhanced recovery of trauma patients. Clearly, the diversity of trauma patients does not permit a single unified ERAS protocol. Rather, system-based protocols that would encourage rapid recovery for each injured system may facilitate a more rapid recovery and may translate into economic benefit. Further studies are needed to assess whether automatic specialty service referral systems may be of cost benefit. Of interest within our institution, an automatic geriatric patient referral pilot program for trauma patients aged 75 years and older (GeriTrauma implemented in November 2017) was enacted within the 5-year study plan and this may have contributed to the demonstrated decreased average cost for care of trauma patients (figure 2). During the study timeline, other specific projects directed toward management of urinary catheters (Catheter-associated urinary tract infection (CAUTI) program piloted in March 2016 and rolled out in June 2017) and increasing the development of the regional trauma network allowing for advanced disposition programs, and improved repatriation policies were instituted which may have also contributed to the decreased average cost of patients seen. Data regarding the increase of admissions during the study timeline across several injury mechanisms, with statistical significance seen for injuries involving impairment related to drugs and alcohol, suicide or self-injury, and motorcycles, speak volumes to the evolving pattern of admissions we face at our institution (figure 2). Given these findings, efforts directed at societal prevention should focus on strengthening involvement in occupational and workplace safety, mental health efforts, as well as drug and alcohol-based rehabilitation programs.
Adverse events in the hospital are never desirable and are potentially avoidable. In our data set, PSIs correlated with higher in-hospital cost in univariate and multivariate analyses. Patients who experienced adverse events in-hospital constituted a larger proportion of the higher cost groups (figure 2, tables 3 and 4). Factors that can translate into cost reduction include diligent management of prophylactic anticoagulation to avoid venous thromboembolic events in the high-risk trauma population once bleeding risk is diminished. Judicious use of preprinted protocols and discontinuation of unnecessary lines and tubes such as urinary catheters along with adequate pain control to avoid respiratory complications in patients suffering from thoracic injuries may translate into cost reduction.
Significant variation in costs was seen when assessing our data set by MOI, with higher costs seen for blunt trauma mechanisms (table 2). Patients with injuries sustained via heavy machinery or road traffic collisions, notably pedestrians, were seen as sustaining on average the highest in-hospital expenditures (table 2). In multivariable regression analyses, penetrating and violent injuries, including stab wounds and gunshot wounds, were negatively associated with cost within the data set (table 3). Factors for this may be driven by systematic considerations of our hospital, namely an automatic mechanism-driven trauma code for penetrating trauma, and that most patients involved in these mostly single-system injuries are younger and less comorbid. It is clear that high-velocity blunt injuries, such as those sustained by patients involved in road traffic collisions, can involve multiple systems and thus may explain the higher associated costs, whereas those incurred by single-system stab wounds may be less. Interestingly, male gender was shown to negatively influence cost in a multivariate analysis (cost ratio <1; table 3). Male gender constituted most patients within our cohort and within all quintiles assessed (69% of all patients). Given that male patients within our data set were more commonly associated with penetrating/violent injuries, this may explain the negative influence on cost within multivariate studies. Taken together, these findings indicate the influence of MOI on driving in-hospital costs. Further studies are required to elucidate specific system injuries (ie, thoracic, abdominal, orthopedic) and their economic impact.
The strengths of our study include a large sample size encompassing the breadth of trauma patients and mechanisms encountered at a Canadian level 1 trauma center. Additionally, a substantial degree of demographic and clinical variables were available for the study and cost analysis. Limitations of our study include its retrospective nature and inherent selection biases. As well, our study was limited to patients admitted to trauma services at our hospital and does not include patients admitted to other departments which may have sustained single-system injuries, patients who died in the trauma bay due to their injuries, and patients discharged directly from the emergency department. We were limited in our analyses of specific comorbidities and in our assessment of surgical intervention of these patients. In addition, we limited our study to in-hospital cost analysis and consequently cannot comment on cost associated with time in rehabilitation, disability-adjusted life-years, or quality-adjusted life-years, important metrics when discussing the economic impact of disease/injury. One important limitation in the temporal analysis of cost is the implementation of programs such as the GeriTrauma program during the course of this study, which are confounders in this analysis.
Conclusion
With temporal trends showing a general increase in trauma admissions related to all studied MOIs during the 5-year study time span (figure 2), our trauma center will undoubtedly encounter hospital management-related logistical stresses. We have shown that both modifiable and non-modifiable factors are significantly associated with hospital costs. We describe that lengthy admissions that may be related to ALC status and placement issues for patients with increased care needs correlate with significant cost and constitute the largest users of hospital expenditure in our quintile analysis of trauma patients. We outline the importance of specific protocols in reducing costly adverse events and we emphasize the importance of a multidisciplinary approach to the care of the trauma patient. We posit that systems-based enhanced recovery protocols may similarly correlate with economic and clinical benefits in the trauma population. Unique care protocols for distinct populations such as the elderly may be required, notably given that injuries are highly likely to be life-altering and carry a significant social and economic burden within geriatric populations. With further studies, we hope that the benefits of these studies can aid in resource allocation and encourage funding in the highly variable field of caring for injured patients.
Acknowledgments
We wish to thank The Ottawa Hospital Data Warehouse (TOHDW) for their skills and expertise in assembling data for retrospective chart review, notably Ms Deanna Rothwell and Mr Jiro Inoue. We wish to acknowledge the Ottawa Trauma Registry and specifically Ms Heather Knight for her assistance in recruiting trauma-related data for retrospective review. We wish to acknowledge the Ottawa Methods Centre for help with the methodological design of the multivariate analyses. We wish to thank Dr Alan Forster, The Ottawa Hospital, for facilitating data acquisition for this project. We acknowledge and thank Mr Timothy Prendergast from Statistics Canada for aid in the assessment of Ottawa-Gatineau population data.
Footnotes
Contributors Project design and Research Ethics Board (REB) approval was obtained by AMF, SF, JL, and MM. Univariate analyses and descriptive statistics were performed by AMF and MM. Variables for multivariate analysis were selected by a consensus group of experts in trauma care, PG, JL, and MM. Multivariate analyses were designed and performed by AMF and KT. All authors contributed to writing and approval of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Institutional Research Ethics Board (REB) approval was obtained (protocol number 20180774-01h) in October 2018 following application and review according to institutional procedures at The Ottawa Hospital, a level 1 trauma center in Eastern Ontario.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.