Article Text

Abstract
Background Recently, interest has increased in surgical fixation for severe thoracic wall injury with good short-term outcomes. However, few reports have evaluated long-term outcomes or complications. This study aimed to assess long-term quality of life and implant-related complications after rib fixation for flail chest and multiple rib fractures.
Methods We interviewed patients who had undergone rib fixation from January 2014 to December 2019 about their current ability to work and their usual life.
Results Twenty-two patients underwent rib fixation during the study period. Two patients with flail chest had already died after the surgery due to senescence; thus, follow-up information was obtained from 20 patients (91%), with a follow-up duration of 47.5 (IQR 22–58) months. The most undesirable event occurring during the study period was irritation caused by a palpable plate (n=2, 10%), probably due to the thin skin of patients over 70 years old. Eighteen patients were able to return to their usual life or same work as in the premorbid state with no complaints. Two patients are still undergoing rehabilitation due to concomitant extremities fractures. The median EQ-5D-5L index score was 0.89 (IQR 0.84–0.93). There were no implant-related complications requiring plate explantation.
Discussion We concluded that rib fixation offers good long-term benefits, with the ability of the patient with flail chest or multiple rib fractures to return to activity in the premorbid state. Elderly patients especially with thin, soft tissue may complain of irritation caused by the plate and should be informed of this prior to surgery.
Level of evidence Level IV therapeutic care/management.
- thoracic injuries
- rib fractures
- thoracic surgical procedures
- bone plates
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Flail chest and multiple rib fractures are one of the most commonly occurring injuries especially in blunt trauma, and their influences on mortality and morbidity are not negligible. As previously reported, up to 60% of patients experienced some kind of morbidity, such as nosocomial pneumonia, prolonged respiratory instability, prolonged number of ventilation days, and a resulting long-term hospital stay.1 2 Recently, open reduction and internal fixation of critical rib fractures have been performed globally with good short-term outcomes.3–5 Previous reports including one meta-analysis comparing the outcomes of surgical rib fixation with conservative therapy for critical thoracic wall injury reported the advantages of rib fixation not only in decreasing mortality and the incidence of pneumonia or tracheostomy but also in shortening the hospital and intensive care unit (ICU) length of stay.3–7
However, the long-term outcomes focusing on delayed complications and patient quality of life after rib fixation are still not well elucidated. Some previous studies described the sufficient effectiveness of surgical rib fixation, but their follow-up rate was only about 50% and follow-up duration was approximately within 1 year.8 9 Therefore, the purpose of this study was to assess the exact long-term patient quality of life and implant-related complications after recent surgical rib fixation for both flail chest and multiple rib fractures.
Patients and methods
Treatment strategies for patients with flail chest and multiple rib fractures
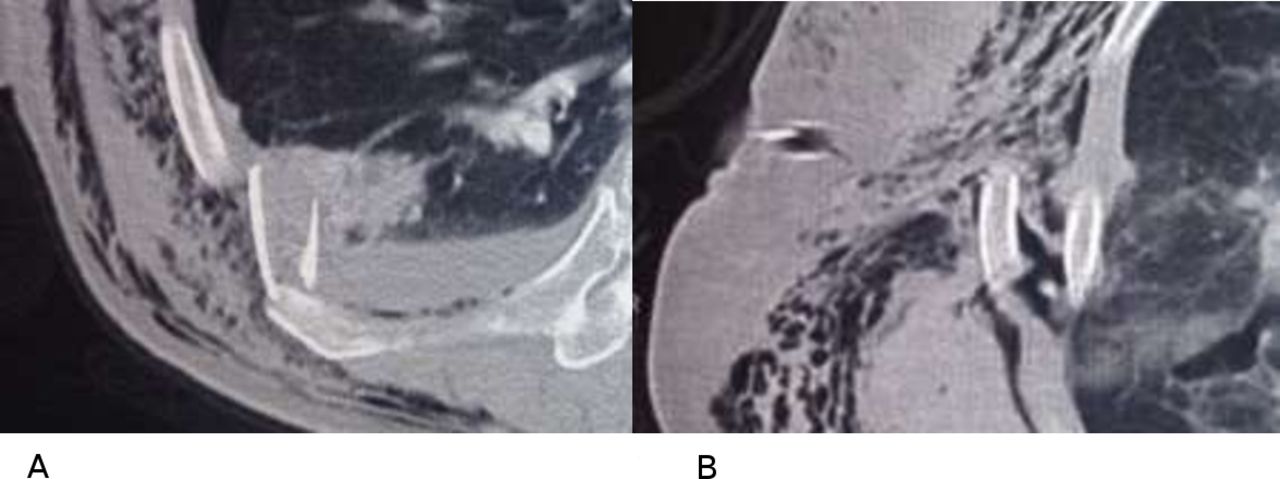
This study was performed at the Department of Trauma and Critical Care Center of Osaka City University Hospital. Because there is no universal definition for multiple rib fractures, we defined the term to be fractures of at least more than two ribs either unilaterally or bilaterally. Following the strategies for multiple rib fractures in our institution, if the patients had a flail segment at their injury site, they were intubated, and operative fixation was the priority for repair of the segment. For patients who did not have flail segments, we preferred to perform surgical rib fixation for massive fractured rib dislocations, such as ribs lacerating the lung (figure 1A) or when overlapping of the fractured ribs was >15 mm (figure 1B) on the basis of CT scan, the patients could not be tapered from continuous intravenous or epidural narcotics, or the patients could not start rehabilitation due to the severe pain caused by the fractured ribs. Patients who died from severe brain, abdominal, spinal, or pelvic injury as indicated by an Abbreviated Injury Scale (AIS) score of >5 were excluded. We also excluded patients with severe brain injury who had not recovered during hospital admission, as indicated by not attaining a Glasgow Coma Scale score of >8, and those with spinal or pelvic injury for which a lateral decubitus position for surgery was difficult or contraindicated.
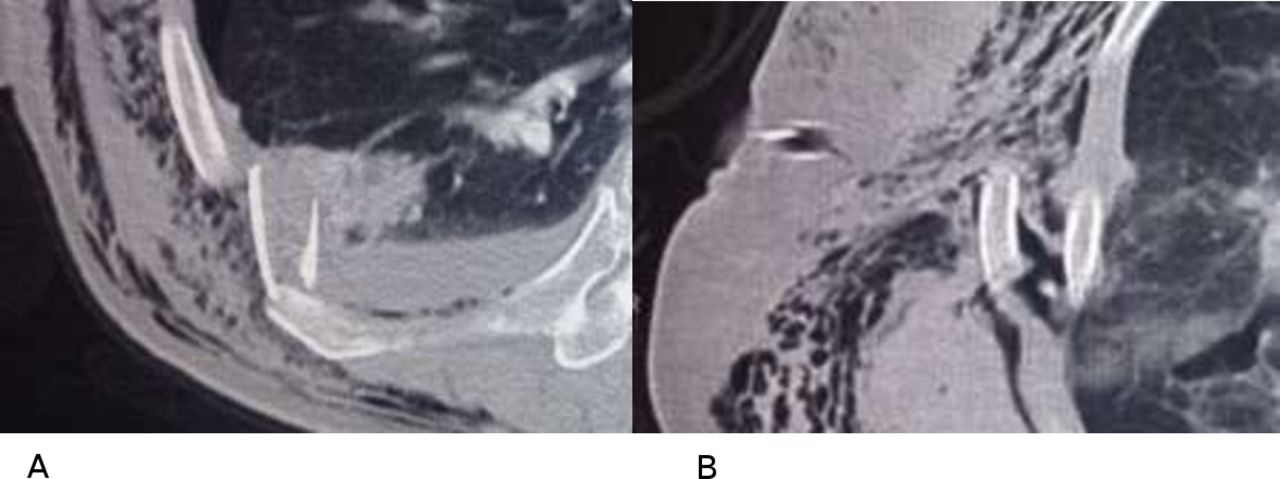
Indications for surgical rib fixation. (A) Massive fractured rib dislocations, such as ribs lacerating the lung. (B) Overlapping of fractured ribs of >15 mm.
Surgical strategy for patients with flail chest and multiple rib fractures
The operations were performed under general anesthesia and differential lung ventilation. Surgical access to the fractured ribs was via posterolateral muscle-sparing or minimal thoracotomy, and depending on the number of fractures to be repaired, several types of skin incisions were performed. In all cases, the three or four most dislocated or flailed segment ribs were fixed by locking screws and plates (Synthes, Oberdorf, Switzerland). After fixation, a 28 Fr intercostal drainage tube and 10 Fr subcutaneous drainage tube were inserted. We consider that if the patients have criteria for surgical rib fixation, the surgery should be performed within 7 days after admission because delayed surgical fixation becomes more difficult and results in longer operating time compared with surgery performed in the early phase following injury.
Survey and evaluation of quality of life of patients
To assess long-term outcomes including patients’ current ability in daily life, current working status and quality of life, we performed a telephone survey with the patients or their families after a minimum of 6 months of follow-up. We also asked about additional interventions needed for implant-related occurrences, such as removal of an implant or administration of antibiotics for infection.
Quality of life was assessed using the Euro quality of life-5 dimensions-5 level (EQ-5D-5L) questionnaire, which was initially introduced in 2009 and updated in 2011.10 This indicator has currently been modified globally, and the Japanese version was published in 2016.11 The descriptive system is composed of five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has five levels: no problems, slight problems, moderate problems, severe problems, and extreme problems.10 The EQ-5D-5L index score ranges from −0.33 to 1.00, where higher scores indicate better quality of life.
Statistical analysis
Because this was a single cohort study with a small sample size and the data were not normally distributed, data for continuous variables are presented as median (25%–75% IQR), while categorical variables are presented as number (%). Data were analyzed using IBM SPSS Statistics V.22.
Ethics consent
Written informed consent was obtained from the patients for publication of this report and any accompanying data.
Results
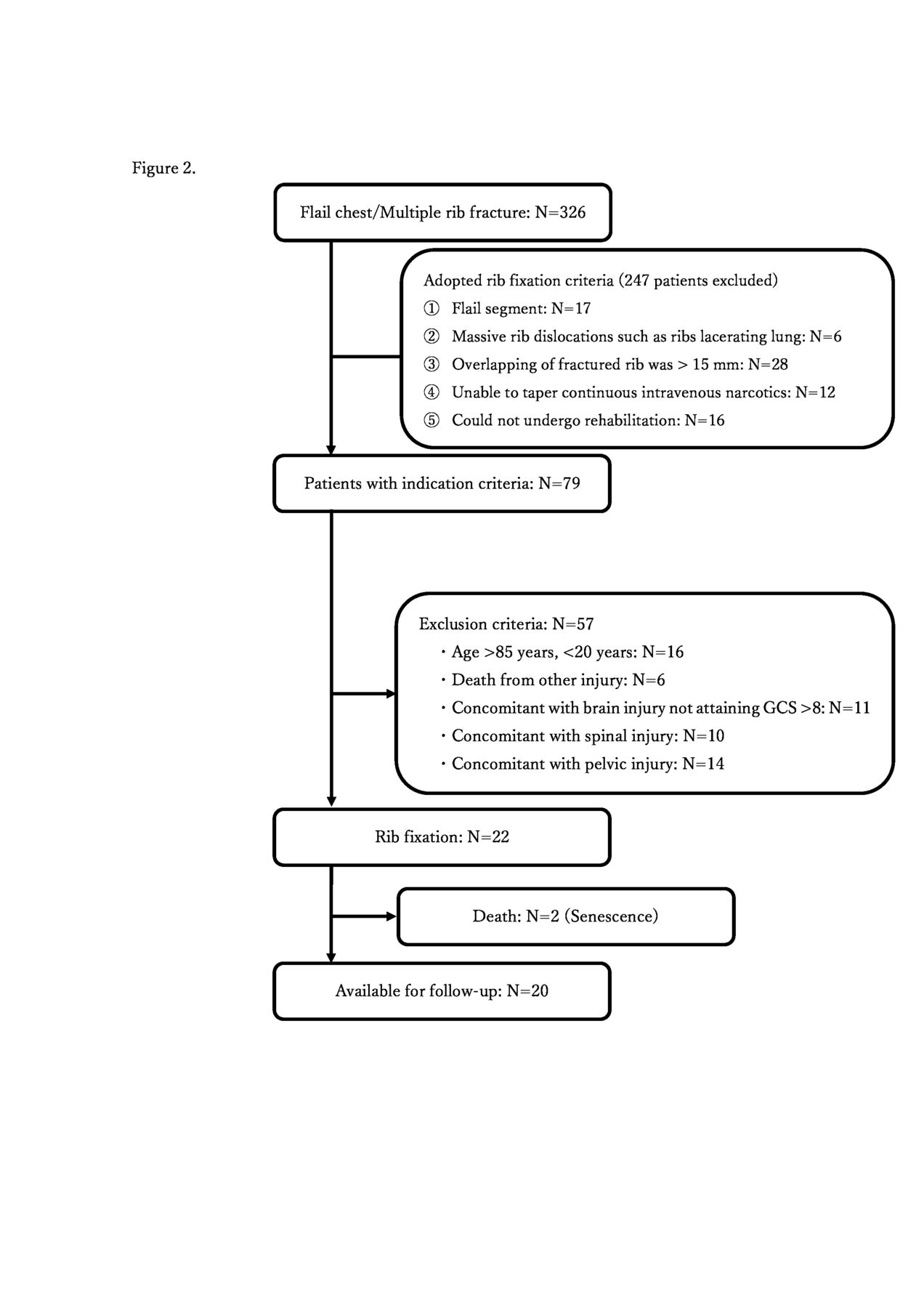
During the study period, 326 patients were diagnosed as having multiple rib fractures by CT scan at admission or after their vital signs became stable enough to allow them to undergo pan-CT scanning. Of these patients, 22 were treated with surgical rib fixation, and we successfully contacted 20 of these patients (91%) for follow-up and to obtain information on their current condition (figure 2). Two patients with flail chest had already died after the surgery due to senescence.
{kind=link}
{kind=link}
Flow chart of patient inclusion in the study. Of the 326 patients diagnosed as having multiple rib fractures, 79 potentially had an indication for rib fixation. However, 57 patients were excluded, and the remaining 22 patients underwent surgical rib fixation. Two patients had already died due to senescence. Finally, we could contact and obtain follow-up information from 20 patients. GCS, Glasgow Coma Scale.
Surgical rib fixation was applied to 9 patients with flail chest and 11 patients with multiple rib fractures. Table 1 shows the baseline characteristics of the patients. The median age was 64 (IQR 56–73) years old, and the median thoracic AIS score was 4 (IQR 4–5). The median Injury Severity Score (ISS) of the patients was 29 (IQR 22–41).
Demographic data of patients
Table 2 provides data on the fractured ribs. The median number of fractured ribs was 8 (IQR 6–10), the number of fixed fractured ribs was 4 (IQR 3–5), and the median days from admission to surgery was 4 (IQR 2–7) days.
Description of the fractured ribs
As short-term outcomes, the median number of days of mechanical ventilation and those of the ICU stay were 4 (1–8) and 6 (3–10) days, respectively. Three (15%) patients with concomitant pneumonia required antibiotics during hospitalization, and one (5%) patient with a medical history of severe chronic obstructive pulmonary disease required a tracheostomy. We also observed acute-phase partial plate detachment within 1 week in one patient (5%), who initially had extensive flail chest concomitant with open pneumothorax on the anterior components. This patient was also complicated with osteomyelitis but was treated successfully with antibiotics and negative pressure wound therapy (5%) (table 3).
Short-term overall outcomes
The long-term outcomes and observed events are described in table 4. The median follow-up duration was 47.5 (IQR 22–58) months. The most undesirable event occurring during the study period was irritation caused by a palpable plate (n=2, 10%), probably due to the thin skin of patients over 70 years old. Eighteen (90%) patients were able to return to their usual life or same work as in the premorbid state with no complaints. Two (10%) patients are still undergoing rehabilitation due to concomitant extremities fractures. The median EQ-5D-5L index score was 0.89 (IQR 0.84–0.93). There were no implant-related complications requiring plate explantation.
Long-term overall outcomes
Discussion
In the previous decade, the treatment options for flail chest depended only on internal fixation by using positive pressure ventilation and pain control.1 2 Surgical rib fixation is currently performed worldwide in major trauma centers, and the reported short-term outcomes are good.5–7 Although rib fixation was initially indicated only for flail chest,4 5 some types of severe multiple rib fracture were also reported to be good indications for surgical rib fixation.6 7 We also introduced our established indications for surgical rib fixation for multiple rib fractures with good short-term outcomes compared with conservative therapy on the basis of propensity-matched analysis.6 There are three main advantages of surgical rib fixation compared with conservative therapy in the short term. First, mortality and the incidence of complications such as pneumonia or tracheostomy are decreased.6 12 Second, it is easy to terminate the administration of continuous intravenous or epidural analgesic drugs such as fentanyl,12 13 which also contributes to helping the patient start rehabilitation smoothly. Third, by performing rib fixation, we can shorten the number of days of mechanical ventilation, which contributes to shortening of length of hospital and ICU stays.14 15
With regard to perioperative unexpected events, we observed one patient with acute-phase partial plate detachment within 1 week. This patient had extensive flail chest including thin anterior costal cartilage and sternum components. Hence, we had to use short unlocking-screw for fixing the plate. However, from this experience, we routinely use longer-sized locking-screw even for fixing anterior thin segment.
Currently, there are few studies evaluating the long-term outcomes or complications of patients undergoing rib fixation, although some studies have described the long-term assessment of factors such as irritation or quality of life of these patients.8 9 16–18 Importantly, these past studies have small sample sizes, their follow-up rates are limited to only about 50% of the patients, and the follow-up duration is within several months up to 1 year.
Beks et al8 reported as long-term results that 48% of their patients had implant-related irritation and 9% required implant removal. In the present study, irritation was also reported by some patients, but the incidence rate was approximately 10% among the patients followed up. We can offer no explanation for the large difference in the incidence rates of this complication between these studies. However, in our study, the two patients complaining of irritation were both aged over 70 years old, and thus we consider irritation to be one of the risks in elderly patients. Currently, none of our patients requires implant removal.
The EQ-5D-5L index is used globally to evaluate the quality of life of patients8 9 19 20 and includes the best components to evaluate patients’ general health condition. The patients who underwent surgical rib fixation in our study had scores almost equal to the average score of the standard EQ-5D-5L index in Japanese aged 60 to 69 years (male: 0.911, female: 0.899).11
Caragounis et al20 reported that 45 patients with rib fixation for flail chest and multiple rib fractures had an EQ-5D index score of 0.93 after 1 year of follow-up. In another study, Campbell et al17 described slightly lower quality of life after 1 year of follow-up following surgical rib fixation. We think this is possibly because their included patients had more severe trauma as indicated by their higher ISS.
As described, the EQ-5D-5L index is a score for evaluating general health conditions and not specifically thorax-related problems. We used this index because we were unable to evaluate the complaints of the patients objectively and directly. However, almost all of the patients indicated that they were adequately satisfied with rib fixation in the long-term follow-up period. There were no implant-related deaths in our patients or complications requiring additional procedures during the observational period.
Although the number of patients in this study is small, it has one of the highest follow-up rates and also one of the longest follow-up durations of the published studies. Previously, we reported that surgical rib fixation is a safe and effective strategy for obtaining good short-term outcomes both for patients with flail chest and those with multiple rib fractures. In this study, the long-term outcome, which was assessed by comparing the EQ-5D-5L index score with that of a Japanese reference population, showed no decrease in the score and patient satisfaction was adequate. Prior to surgery, it is important to inform patients, especially the elderly patients, that about 10% of them may experience irritation from the rib plating.
Limitations
Although the present study is a small preliminary report with good follow-up, it is a single-center study, and the number of patients is too small to establish significance and conclusive proof of long-term benefits of surgical rib fixation. Further multi-institutional, prospective, randomized trials will be needed to assess the long-term outcomes of surgical rib fixation and its complications.
Conclusions
We conclude that in patients with flail chest or multiple rib fractures, rib fixation offers good long-term benefits for return to their premorbid state. Older patients, especially those with thin, soft tissue, may complain of irritation caused by the rib plate and should be informed of this prior to surgery.
References
Footnotes
Contributors KU and YM designed this study and also conducted the literature search. ToN contributed to the literature search, data analysis, study design, critical revision, and writing of the article. KU and MM contributed to data collection and data interpretation. TeN contributed to the literature search, data interpretation and critical revision. SK and HY contributed to study design and critical revision. All authors read and approved the final article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval As this was a retrospective study with no additional interventions, the Institutional Review Board of Osaka City University waived the need for ethical approval for this study
Provenance and peer review Not commissioned; externally peer reviewed.