Article Text

Abstract
Background Cricothyrotomy is associated with significant aerosolization that increases the potential risk of infection among healthcare providers. It is important to identify simple yet effective methods to suppress aerosolization and improve the safety of healthcare providers.
Methods 5 ear, nose and throat and general surgeons used a locally developed hybrid cricothyrotomy simulator with a porcine trachea to test three draping methods to suppress aerosolization during the procedure: an X-ray cassette drape, dry operating room (OR) towels and wet OR towels. The three methods were judged based on three categories: effectiveness of suppression, availability in all healthcare systems and ease of handling.
Results All five surgeons performed the procedure independently using each of the three suppression methods. The wet OR towel drape was found to be an effective method to suppress aerosolization, and it did not hinder the surgeons from performing the procedure accurately. This finding was confirmed by using an atomized fluorescein dye injection into the porcine trachea, representing aerosolized material while performing the procedure.
Conclusions We present a novel intervention using wet towels to suppress aerosolization during cricothyrotomy. Wet towels are cheap and readily available within any healthcare setting regardless of the financial resources available.
- airway management
- critical care
- emergency treatment
- intubation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Emergency surgical airway, cricothyrotomy, is an aerosol-producing procedure that increases the risk of infection for healthcare providers particularly during epidemics or pandemics.1 2 National and international healthcare organizations have provided safety guidelines for airway management and for non-emergent tracheostomy procedures, but there is little information on how to suppress aerosolization when performing emergent surgical airways, that is, cricothyrotomy. There are no known practical recommendations on how to suppress aerosolization and splatter apart from those published in May 2020 by the American Association for the Surgery of Trauma, which recommends that ventilation should be stopped as a measure to decrease the generation of aerosolized matter but did not address suppression of active aerosolization.3 During early March 2020, we were faced with escalating numbers of emergency intubations for patients with COVID-19 or suspected cases that had the potential to require cricothyrotomy at Northwestern Memorial Hospital in Chicago, Illinois, USA. To address concerns about aerosolization during this emergency (often bedside) procedure, a taskforce of ear, nose and throat surgeons and trauma/critical surgeon developed and evaluated three methods to suppress aerosolization during cricothyrotomy. The following study describes the approach this group of surgeons undertook to reach institutional practice recommendations for performing cricothyrotomy on suspected or proven cases of COVID-19.
Methods
Five board-certified surgeons (4 ear, throat and nose surgeons and one trauma/critical care surgeon) used a locally developed hybrid simulator with a porcine trachea to test three methods to suppress aerosolization during cricothyrotomy at the Northwestern Simulation Laboratory, Northwestern University Feinberg School of Medicine. The surgeons agreed on standard procedural steps for cricothyrotomy. The group adopted a previously described technique ‘Scalpel–Bougie–Tube’ approach, which is based on Seldinger technique using a bougie as a guide.4–6 Box 1 lists the cricothyrotomy procedural steps that were implemented by the surgeons.
Procedural steps for cricothyrotomy using the Scalpel–Bougie–Tube technique
Cricothyrotomy procedure steps
Palpate the thyroid notch and cricoid cartilage. Use the thumb and middle finger of your non-dominant hand to fix the tracheo-laryngeal complex in position.
Use size 10 scalpel to create a 3–5 cm vertical skin incision starting inferior to the thyroid notch.
Use a hemostat to reach the cricothyroid membrane.
Use the scalpel to incise the membrane horizontally.
Remove scalpel and insert your non-dominant index finger until you reach the posterior wall of the airway.
Deliver the bougie with the ETT mounted on it into the trachea along your index finger directing it inferiorly toward the carina.
Slide the size 6 ETT over the bougie into the airway. Do not advance the tube beyond 5 cm into the trachea.
Inflate the ETT balloon and withdraw the bougie.
ETT, endotracheal tube.
Then in a two-step process, the group of surgeons evaluated the effectiveness of using a see-through X-ray cassette drape, dry operating room (OR) towels and wet OR towels as neck coverings to suppress aerosolization during cricothyrotomy. figure 1 shows the three types of drapes that were used in the experiments. These particular materials were chosen because they are readily available in the emergency department (ED) where most potential cases take place. We did not include the larger C-arm fluoroscopy drape because it is not readily available in the ED.

The three types of drapes that were used in the experiments: (A) X-ray cassette drape; (B) dry towels; and (C) wet towels.
In the first step of the experiment, the five surgeons performed the surgical cricothyrotomy procedure independently. Each surgeon was provided with a cricothyrotomy simulator containing a swine trachea and the three types of drapes; trachea replacements were provided if needed. The criteria used to evaluate each of the three coverings were the following: is it easy to use; does it cover the hands of the surgeon through the whole procedure; and does it hinder the procedural steps. The surgeons were also instructed to identify the best orientation of the drape that allows the maximum versatility and least hindrance to performing the procedure.
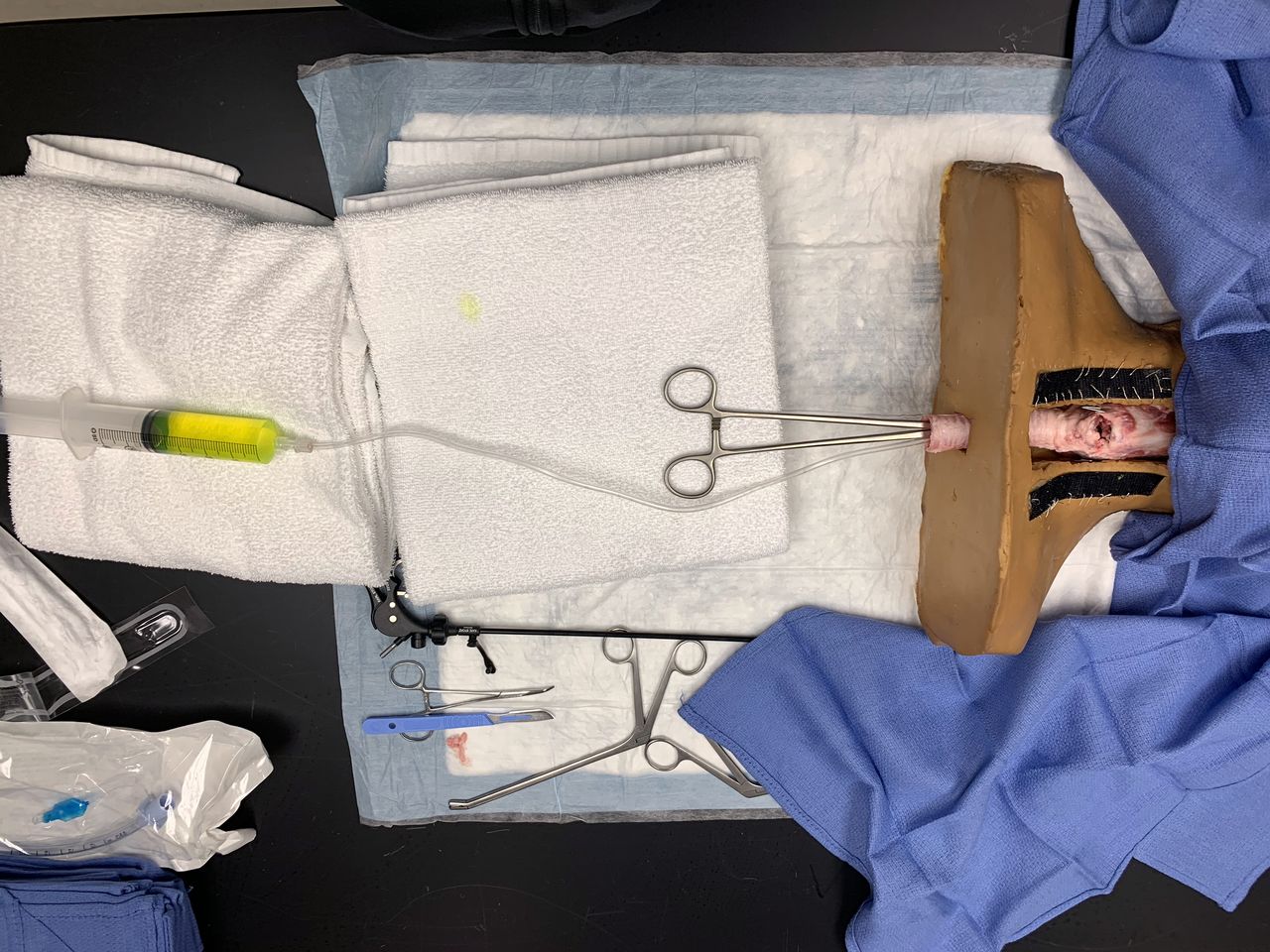
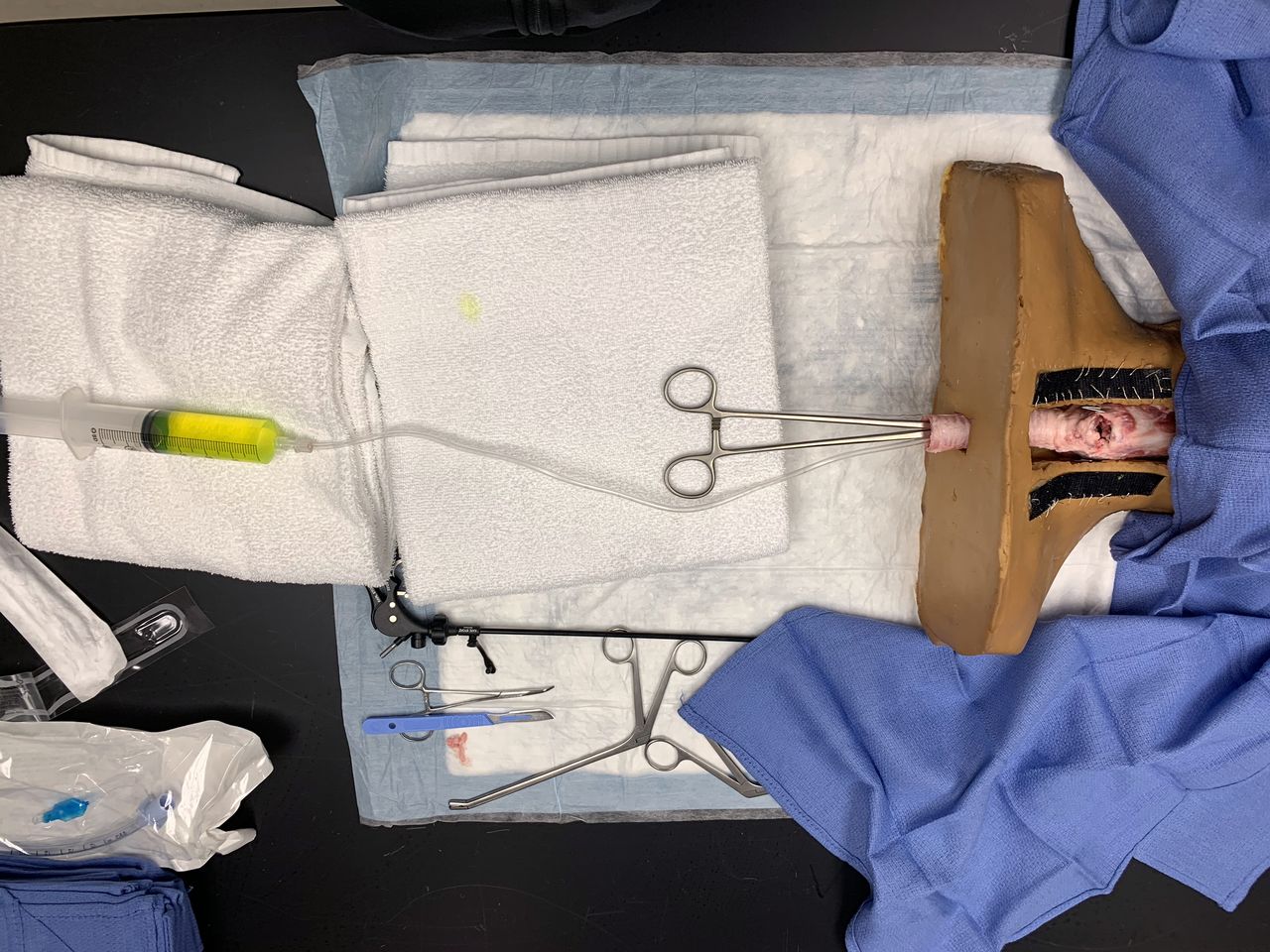
In the second step, the surgeons injected fluorescein dye through an atomizer, representing aerosolized material, placed into the lower end of the porcine trachea when the surgeon was cutting into the cricothyroid membrane to evaluate the effectiveness of each of the three drapes (figure 2). We then shined a black light on the surgical field to assess the contamination of aerosolized fluorescein on the surgeon and healthcare providers’ gowns and face shields (see online supplementary video 1). The testing of each drape with atomized fluorescein dye and the black light was repeated twice with two different surgeons while witnessed by the rest of the team. The surgeons then met as a group to discuss their individual experience with each type of drape and their assessment of the fluorescein dye test to reach consensus on which drape to recommend for use during emergent cricothyrotomy on known or suspected patients with COVID-19.
Supplementary video
{kind=link}
{kind=link}
The setup used to inject fluorescein dye through an atomizer, representing aerosolized material, into the lower end of the porcine trachea. The simulated skin covering layer was removed to show the porcine trachea within the simulator.
Results
The five surgeons agreed that all three drapes offered aerosol suppression. They also agreed that using the sterile see-through X-ray cassette drape to cover the neck while performing cricothyrotomy allowed for the best visualization and that it was easy to manipulate. However, this drape did not allow a firm seal around the surgeon’s hands, which allowed aerosolized materials to escape and cause contamination of the surgeon and the healthcare team. The dry OR towels were easy to manipulate but hindered visualization and easily slipped off the surgeon’s hands, again exposing the surgeon to the aerosolization of materials from the airway. When using the wet OR towels to cover the operative site, all five surgeons agreed that the wet towels remained over the hands of the surgeon during the procedure. When discussing their observations from the black light test, they all agreed that all three drapes provided suppression of the aerosolization but that was dependent of how well the drape stayed covering the procedure field (see online supplementary video 1). Moreover, the surgeon-investigators reached a consensus advocating the use of wet towels during cricothyrotomy but acknowledged that while the reduction of the aerosolization using the wet towels came at the expense of some of the visibility, it did not hinder the ability to perform the procedure safely because cricothyrotomy is dependent on the tactile identification of the anatomical landmarks more than depending on visual cues. Table 1 summarizes the conclusion reached by the group of investigators.
Summary of the five surgeons’ consensus on the ease to manipulate, ability to cover the surgeons hands throughout the procedure, hindrance of procedural steps and ability to suppress aerosolization for each of the three surgical drapes used during emergency cricothyrotomy
Discussion
We illustrate the effectiveness of using wet towels to suppress aerosolization during the performance of a cricothyrotomy procedure on a locally developed hybrid simulator. This technique, using wet towels, takes advantage of the cheap and readily available cloth towels that do not require extra investment in time, money or efforts and is suitable to all healthcare settings, poor and wealthy. Additionally, experienced surgeons can easily rely on their tactile senses to perform cricothyrotomy using anatomic landmarks. The surgeons acknowledged that the increased safety that wet towels provide comes at the expense of compromising the visual cues, but they all agreed that this did not compromise the efficiency and accuracy of performing the procedure given that cricothyrotomy is dependent on tactile identification of the anatomical landmarks and not on visual cues. We recommend the deployment of wet towels as a safety measure when performing cricothyrotomy regardless of the instrument used (eg, tracheostomy tube or cricothyrotomy tube) or whether the surgeons choose a different procedural technique not employing a bougie.
Other innovative techniques for airway surgery have been developed during the COVID-19 pandemic to enhance the safety of healthcare providers by suppressing aerosolization. These innovations include the use of see-through C-arm covers with suction to create a negative pressure space when performing tracheostomy,7 the use of a metal frame set and a see-through C-arm cover to perform tracheostomy8 and using double drapes when performing mastoidectomy.9 All these innovative techniques are well suited for the OR where resources are readily available. We believe our technique is well suited for performing emergent cricothyrotomy either inside or outside of the OR (eg, in the ED or at the patient’s bedside). Additionally, using wet towels is inexpensive and can be easily used in healthcare systems where personal protective equipment (PPE) or ORs may not be readily available. However, we do stress the importance of using full PPE including face shields and N95 masks or a Powered Air-Purifying Respirators (PARP) whenever available. It is also important to emphasize that airway management of patients with suspected or proven COVID-19 should comply with national and international guidelines including cessation of ventilations and using negative pressure rooms for all airway procedures.10
Limitations
There are several limitations to our study. First, this study reflects the consensus agreement of a small group of surgeons within a single institution on how to perform cricothyrotomy safely during an escalating COVID-19 crisis based on our own personal experiences and comfort. Other groups may elect to choose a different procedural approach, a different airway instrument or even make use of different barrier materials based on their own expertise and locally available resources. For example, we used an endotracheal tube (ETT), while other surgeons may use tracheostomy or cricothyrotomy tubes. Our use of the ETT was based on our current practice within the institution and the fact that cricothyrotomy tubes are not kept in storage. However, we believe that using wet towels as a barrier against aerosolization remains a viable option to contain aerosolization regardless of the technique or instruments used. Second, we did not calculate the procedural time by the different surgeons or provide comparisons of the new wet towel technique with the surgeons baseline performance using their personal procedural steps (without a wet towel). Finally, we were unable to show the effects of our new technique on actual clinical outcomes due to the rare nature of emergency cricothyrotomy.
Conclusions
Wet OR towels suppress aerosolization during cricothyrotomy on a locally developed hybrid simulator. Based on our findings, we recommended its use as a barrier against aerosolization in all cricothyrotomy procedures at our institution. We share our investigative methodology and experimental findings with the larger community of healthcare providers for the greater benefit during the COVID-19 pandemic or other potentially infective disease processes. At the conclusion of our work, we decided to create a simulation-based educational program to train all those involved in performing cricothyrotomy at our institution (residents, fellows and attendings).
Acknowledgments
We would like to thank the Instructional Design and Development Team at Northwestern Simulation: Kim Le Mezo, Deon Griffin and James Brucker for their help creating and editing the video.
Footnotes
NI and JHB are joint first authors.
NI and JHB contributed equally.
Collaborators Instructional Design and Development at Northwestern: Kim H Le Mezo; Deon Griffin; James B Brucker for creating and editing the video.
Contributors All seven authors contributed to the concept, design, drafting and revision of the manuscript. NI, WEL, SS and DBC provided the conception and design. NI and JHB prepared the initial draft for the manuscript. All authors contributed to interpretation of data and critical revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.