Article Text

Abstract
Background Time to definitive hemorrhage control is a primary driver of survival after penetrating injury. For these injuries, mortality outcomes after prehospital transport by police and emergency medical service (EMS) providers are comparable. In this study we identify patient and geographic predictors of police transport relative to EMS transport and describe perceptions of police transport elicited from key stakeholders.
Methods This mixed methods study was conducted in Philadelphia, Pennsylvania, which has the highest rate of police transport nationally. Patient data were drawn from Pennsylvania’s trauma registry and geographic data from the US Census and American Community Survey. For all 7500 adults who presented to Philadelphia trauma centers with penetrating injuries, 2006–2015, we compared how individual and geospatial characteristics predicted the odds of police versus EMS transport. Concurrently, we conducted qualitative interviews with patients, police officers and trauma clinicians to describe their perceptions of police transport in practice.
Results Patients who were Black (OR 1.50; 1.20–1.88) and Hispanic (OR 1.38; 1.05–1.82), injured by a firearm (OR 1.58; 1.19–2.10) and at night (OR 1.48; 1.30–1.69) and who presented with decreased levels of consciousness (OR 1.18; 1.02–1.37) had higher odds of police transport. Neighborhood characteristics predicting police transport included: percent of Black population (OR 1.18; 1.05–1.32), vacant housing (OR 1.40; 1.20–1.64) and fire stations (OR 1.32; 1.20–1.44). All stakeholders perceived speed as police transport’s primary advantage. For patients, disadvantages included pain and insecurity while in transport. Police identified occupational health risks. Clinicians identified occupational safety risks and the potential for police transport to complicate the workflow.
Conclusions Police transport may improve prompt access to trauma care but should be implemented with consideration of the equity of access and broad stakeholder perspectives in efforts to improve outcomes, safety, and efficiency.
Level of evidence Epidemiological study, level III.
- wounds
- penetrating
- healthcare disparities
- policy
- emergency medical services
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Hemorrhage control is a primary determinant of survival after penetrating trauma.1–3 Accordingly, a key goal of trauma system improvement is to minimize prehospital time.4–6 In urban areas near trauma centers, at-scene prehospital interventions may delay transport with little benefit. This is supported by evidence demonstrating that patients transported in private vehicles have better survival outcomes when compared with those transported by emergency medical services (EMS).7 This is likely because, unlike EMS, bystanders are not delayed by the need for notification, dispatch, and travel. Police on patrol are often first to arrive at the scene of an injury. Direct hospital transport by police has demonstrated its potential to improve survival outcomes after penetrating injuries.8–10 However, little is known about the broader impact of police transport on patients, police officers, and trauma centers.11
Philadelphia, Pennsylvania, was the first US municipality to codify a ‘scoop and run’ policy in 1987.12 13 This policy authorizes non-medical police personnel to transport patients to the nearest trauma center without waiting for EMS in cases of ‘a serious penetrating wound, eg, gunshot, stab wound, and similar injuries of the head, neck, chest, abdomen’.14 By 2015, over 50% of patients with penetrating injuries arrived to one of the city’s eight trauma centers in a police vehicle.8 15 Philadelphia has the highest police transport rate for any US city,16 17 followed by Sacramento and Detroit,18 and more than 60% of all US police hospital transports occur in Philadelphia. Other cities are beginning to adopt police transport policies to meet the emergency medical needs of their residents.16
Police transport upends many of the usual expectations for prehospital patient care and understanding its full effects can inform trauma systems seeking new strategies to reduce the impact of penetrating injuries. In Philadelphia, for example, patients with penetrating injuries are predominately young Black men who may be at higher risk for mortality after trauma and postacute morbidities like depression and post-traumatic stress disorder.19–22 Qualitative evidence has illustrated how some injured Black men associate police transport and their interactions with law enforcement prior to reaching a trauma center with additional pain and feelings of dehumanization.23 24 Police transport may also pose underappreciated hazards to officers who provide injury first response with minimal medical training and equipment. Lastly, no studies have assessed variations in police transport and access to trauma care across a municipality or the effect on trauma care processes at a receiving center. To our knowledge, no study has evaluated police transport beyond hospital survival and length of stay.
In this study, we examine the practice, context, and social perception of police transport in Philadelphia, as a case study of the municipality with the longest and most prevalent use of police transport as a prehospital strategy. To do so, we combined a quantitative analysis of retrospective trauma registry data with a prospective exploratory qualitative analysis to achieve two distinct but complementary aims. The quantitative arm of this study aimed to identify the influence of geography, neighborhood sociodemography and crime incidence on prehospital transportation for victims of penetrating injuries over 10 years in Philadelphia. We hypothesized that the distribution of police versus EMS transport would differ by neighborhoods of the city and would be associated with the sociodemographic features and crime incidence of those neighborhoods.4 In the qualitative arm of this study we used qualitative interviews to develop an in-depth description the perceived advantages and disadvantages of ‘scoop and run’ as it is interpreted by injured people, police, and trauma clinicians working in the city’s trauma center emergency departments (EDs).25 26 This approach allows us to identify the perceived trade-offs of police transport in practice that we might not have expected a priori and serves to generate hypotheses for future testing.
Study design
We used a concurrent (QUANT-QUAL) mixed methods approach.27 Multivariate regression and geospatial modeling of trauma registry data permitted us to examine individual and geographic characteristics that predict police transport relative to EMS. Qualitative interviews and content analysis of interview data offered a complementary perspective on police transport from the point of view of primary stakeholders.
Quantitative methodology
We drew clinical and demographic data on all Philadelphia residents treated for penetrating injury at a Philadelphia trauma center, 2006–2015, from the Pennsylvania Trauma Outcomes Survey (PTOS) registry. This registry includes all injured patients: admitted for 48 hours or at least 36 hours with Injury Severity Score (ISS) ≥9; all intensive care unit (ICU) and step-down admissions regardless of duration; all deaths; and all transfers from other hospitals. Patients are excluded from the registry if they have an isolated hip fracture, or injuries due to asphyxiation, drownings, poisonings, or in-hospital injury.28 The reliability of PTOS data is supported by site visits and audits to ensure that registry data are accurate and consistently collected as a requirement for accreditation of trauma centers in the Commonwealth of Pennsylvania.29
From registry data we selected any patient presenting for penetrating injury via police transport or ground EMS. Patients arriving via private transport were excluded. Patients were also excluded if their zip code of residence was missing (less than 1% of sample), which is the smallest geographic identifier available for each patient in the trauma registry. Neighborhood sociodemographic information was collected at the zip code level from US Census30 and the American Community Survey 5-year estimates for 2007 and 2011, and neighborhood crime statistics from records published by the Philadelphia Police Department (PPD).31 Given that zip code areas are both small and arbitrarily defined, we aggregated populations into 12 neighborhoods that aligned with the city of Philadelphia’s Planning Analysis Sections32 to reproduce administratively, socially and culturally relevant groupings.
Variables
The main dependent variable was police transport. Demographic variables included age, sex, race, ethnicity and insurance type. Injury diagnoses were derived from International Classification of Diseases, 9th Revision codes. Mechanism, location of injury, and injury intentionality were derived from external cause-of-injury codes.
We evaluated neighborhood crime characteristics including rates of aggravated assault, robbery with a gun, homicide, and narcotic arrests. We evaluated neighborhood sociodemographic characteristics including racial and ethnic make-up, percent of adult population with less than a high school education, percent of vacant housing units, percent of living in poverty, percent of unemployed, and percent of receiving public assistance. We also included number of police and fire stations in each neighborhood. EMS in Philadelphia is part of the city’s Fire Department and ground EMS deploys from fire stations. After evaluating variables for collinearity, final models included number of fire stations, aggravated assault rate, narcotic arrest rate, percent of the population that was Black, percent of housing units that were vacant, and percent of living in poverty.
Analysis
We used bivariable and multivariable analyses to compare police-transported to EMS-transported patients. Categorical variables were compared using χ2 tests and continuous variables were compared using the Kruskal-Wallis test. We used multivariable logistic regression to identify significant predictors of police transport. Candidate predictors were included in the final model if p<0.2 in bivariable testing. We constructed three models to explore the relationship between individual and neighborhood risk factors. First, we constructed a multivariable logistic regression model using only individual patient characteristics to predict odds of police transport. Next, we added neighborhood of residence as a fixed effect to determine if neighborhood-level differences existed in odds of police transport. We found that there were significant differences, and constructed our final model, presented here, as a multilevel logistic regression analysis to identify both individual and neighborhood characteristics that were significantly associated with police transport. Neighborhood characteristics were included as linear predictors, and were standardized to their means prior to inclusion in the model. For each factor, the OR we report represents the change in odds of police transport associated with a change by 1 SD in the predictor in question.
We mapped the proportion of patients undergoing police transport in each zip code and neighborhood, as identified by the Political and Community Service Boundaries of the Philadelphia City Planning Commission,32 over each year. We calculated Moran’s Index of spatial autocorrelation, and conducted a Getis-Ord-Gi hot spot analysis to identify areas of significantly high and low rates of trauma center triage.33 34 Location of injury was estimated by home zip code, which is a validated technique in trauma research.35
Quantitative results
Predictors of police transport, 2006–2015
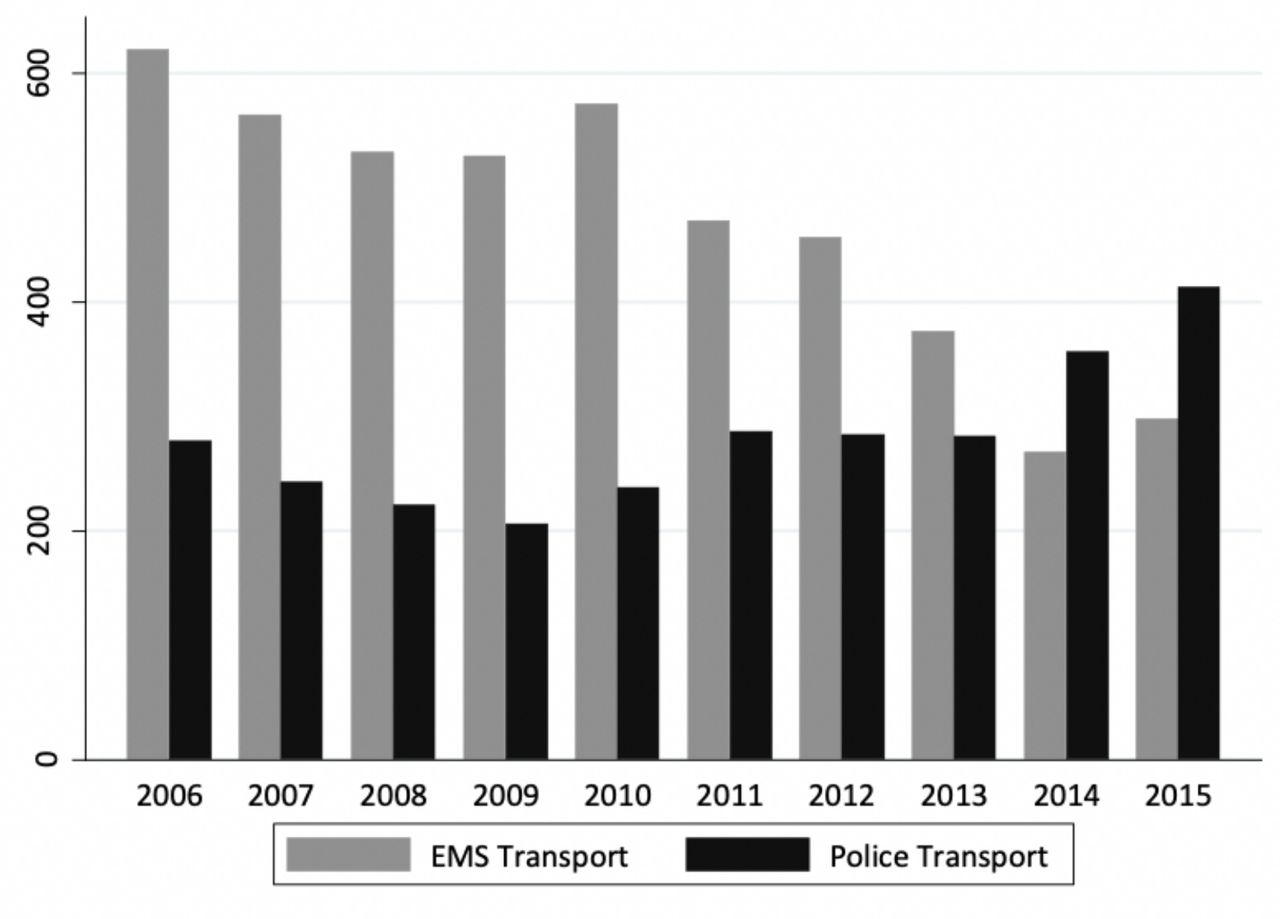
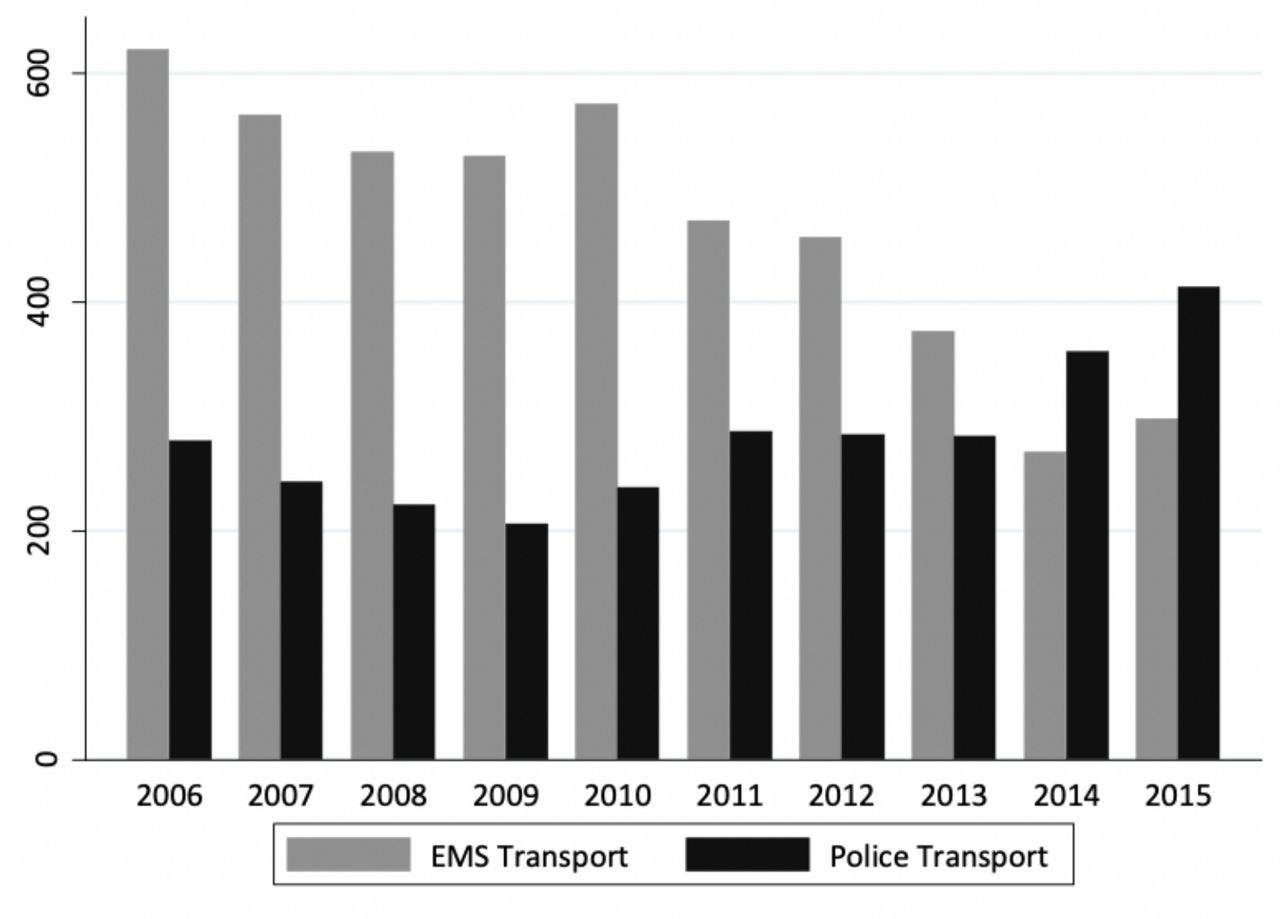
Of 9438 patients with penetrating injury, 4687 (49.7%) were transported by EMS, 2813 (29.8%) by police, and 1938 (20.5%) by private or unknown vehicle. Rates of police transport increased over time, from 27% in 2006 to 57% in 2015 (figure 1), and varied by region of the city. Patients residing in 45 zip codes in Philadelphia were included. The median number of penetrating injuries per zip code was 97 (IQR 34–255). The median number of police transports was 28 (IQR 9–99), as shown in online supplemental figure 2. The individual patient characteristics and outcomes of penetrating injuries relative to mode of transport are shown in table 1.
Supplemental material
Penetrating injury patients transported by police and EMS, 2006–2015
{kind=link}
Penetrating injuries in Philadelphia, 2006–2015, by emergency medical services (EMS) and police transport type.
Using only patient characteristics, the factors significantly associated with police transport included: injury in a public location (OR 2.2; 95% CI 1.9 to 2.6) and during the night (defined as 22:00–04:00, OR 5.6–7.4), assault injury (OR 1.6; 95% CI 1.5 to 1.7), and a more recent year of injury (OR 1.16 for each additional year; 95% CI 1.1 to 1.2). Female sex was associated with decreased odds of police transport (OR 0.6; 95% CI 0.6 to 0.7) as was older age (OR 0.99 for each additional year of age; 95% CI 0.98 to 0.99). Glasgow Coma Scale (GCS) and ISS were not significantly associated with police transport, but hypotension at admission was (OR 1.4; 95% CI 1.2 to 1.5). When neighborhood of residence was included as a fixed effect, these patient-level associations remained very similar. Neighborhood of residence was strongly associated with odds of police transport, with ORs ranging from 1.2 to 3.0.
When we combined patient and neighborhood-level characteristics (table 2), patient characteristics remained significant predictors, though some effects were attenuated. For example, gunshot wound injury was associated with only a 58% increased odds of police transport compared with a 650% increase in odds when looking at patient factors alone. Neighborhood characteristics associated with increased odds of police transport included number of neighborhood fire stations, percent of vacant housing units, and percent of Black population. Neither violent crime rates nor narcotic arrest rates were significantly associated with police transport.
Individual and neighborhood characteristics associated with police transport in patients with penetrating injury, Philadelphia, 2006–2015
Qualitative methodology
We recruited a purposive sample of key stakeholders to participate in qualitative interviews, including: (1) patients with penetrating injuries who arrived at a trauma center via police transport; (2) police with experience transporting individuals with penetrating injuries; and (3) trauma surgeons and nurses who receive patients with penetrating injuries in trauma center EDs. Interviews were approximately 30 minutes in duration and performed by a study team member using a semistructured interview guide. All interviews were audio recorded and transcribed by a Health Insurance Portability and Accountability Act (HIPAA)-compliant transcription service. In accordance with standards for qualitative research rigor and case-oriented analysis, the number of interviews was not predetermined, but rather determined in concurrent data collection and analysis, when descriptive data saturation was achieved.36
Patients with penetrating injuries were consecutively recruited for interviews during hospitalization in the ICU or trauma step-down unit of a level 1 trauma center in Philadelphia. Of the eight victims of penetrating injuries who were approached on the 3 days in which interviews were elicited, six agreed to participate and were interviewed privately on day 2 of their hospitalization. All interviewees were male, between 22 and 43 years, Black or African American, and victim of a single or multiple gunshot wounds, and were broadly representative of the census of police-transported patients with penetrating injuries in Philadelphia. In accordance with previous research on trauma patient perceptions of injury management including prehospital experiences, interviews took place during hospitalization to optimize recall.37 38
Police participants were recruited from three different police districts in Philadelphia. Of the 10 police officers approached, all agreed to participate. These participants were interviewed in a private setting in their police district headquarters. We interviewed 10 officers (nine male, one female). Participants had between 1 and 20 years of experience working with the PPD.
Clinician participants were recruited from a level 1 trauma center in Philadelphia which serves as a catchment for a large region of city which contains the three police districts from which police participants were recruited. Clinicians were interviewed in a private location at the trauma center where they were employed at a time when they were not responsible for patient care. To capture the range of clinician perspectives, we recruited trauma surgeons and registered nurses currently working in an ED of a trauma center in Philadelphia. Of the six clinicians approached to be interviewed, all agreed to participate. Surgeon participants (two male, one female) had between 2 and 12 years of experience providing surgical care (postresidency) in Philadelphia trauma centers. Nurse participants (two male, one female) had between 6 and 12 years of experience in Philadelphia trauma centers.
Analysis
Qualitative interview data were managed for analysis using NVivo V.11 software and analyzed iteratively using content analysis.39–41 One research team member open coded all interview data, organizing these codes into categories and themes that represented stakeholder perspectives. Early findings guided the focus of future interviews which continued until descriptive saturation was achieved.42 A second team member validated this coding schema and the few differences in the interpretation of interview data between coders were resolved through discussion until consensus was achieved.
Qualitative findings
Trade-offs of police transport identified by stakeholders
Tables 3–5 outline the major themes and exemplar quotes identified in analysis of qualitative interview data. Patients, clinicians, and police participants all perceived rapidity and life-saving potential as the primary benefit of police transport. Patients described how it ‘kept (them) alive and bought some time’, and made them feel that the police cared about their well-being and survival. Police participants viewed it as an opportunity to ‘save a lot of lives’ and make a positive difference in the communities they served. Police also described that it often also appeased bystanders’ demand for medical intervention. The scenes of violent injuries, they explained, can draw crowds and conflict and ‘waiting for EMS makes (the police at the scene) look bad’.
Patient perceptions of police hospital transport
Police perceptions of police hospital transport
Trauma clinician perceptions of police transport
Each stakeholder group identified different perceived disadvantages. For patient participants, the ride to hospital in a police vehicle felt painful and unsecured. One participant likened it to a ‘roller coaster’, and another as ‘scary’, because there was no safety belt or restraint. Patients also assumed that if they were transported by EMS, they would have been ‘worked on’ and receive medical care en route.
Police identified exposure to health risks as a primary disadvantage. Moving an injured person from the street to the back of police vehicle was described as physically difficult, especially when an injured individual was unable to bear weight. Officers have disposable gloves but described that these offered limited protection when moving a bleeding individual into a vehicle, and when cleaning blood from vehicles after a transport. They also reported that it was easy to forget to use in their hurry to get a patient to the hospital. Although the majority of police felt that they had the common sense required to identify a penetrating (vs. blunt) injury and perform hospital transport, some were concerned that the extent of their training (basic cardiopulmonary resuscitation and tourniquet use) did not prepare them for making decisions about transport urgency in multiple causality scenarios.
Trauma clinicians had differing perceptions of the disadvantages of police transport. Trauma surgeons associated police transport with increased chaos in the ED due to minimal notification of arrival. This, they reported, threatened the protocolized, team-based approach required for an efficient trauma resuscitation. Surgeons also noted cases in which police-transported patients may have benefited from EMS transport including severe burns, blunt injuries, and spinal injuries. Nurses described concerns about safety risks that included injuries to patients resulting from the structure of police vehicles and speed of driving, risks to the public from road traffic collisions, police officers’ exposure to blood and bodily fluid, and the increased likelihood that firearms in patients’ possession would be brought into the ED.
Each stakeholder group identified different strategies to optimize current police transport practice. Patients advocated for more ambulances on ‘standby’ throughout the city, padding on the seats of police vehicles, and less questioning by police at the scene of an injury prior to transport. Police believed that transport would be enhanced with more equipment to prevent exposure to blood and bodily fluids and training for triage in mass casualty situations. Surgeons felt that police would benefit from training in triage criteria, tourniquet use, and blood exposure safety well as well as enhancement of the notification system to alert the trauma team of an impending police transport arrival. Nurses advocated for protective equipment for police, changes to police vehicles for ease and stability of transport, protocols to search for weapons on arrival to the ED, and enhanced training for police on tourniquet use to limit bleeding during transport.
Discussion
Police transport can reduce delays in definitive care for critically injured patients, and is increasingly appealing to cities and trauma systems around the USA.13 43 In this mixed methods study, we identified trade-offs associated with police transport from the point of view of patients, police and clinical stakeholders. These findings should inform municipalities and trauma systems seeking to implement police transport as part of a broader prehospital strategy. For both patients and police, police transport represented a generally positive opportunity for police–citizen interactions. All stakeholders perceived police transport as expedient and life-saving but identified a range of concerns about its impact on the health and safety of patients, police, and the trauma clinicians who receive injured people in the ED. Consistent with previous research on police transport outcomes, mortality in police-transported patients is higher than EMS-transported patients. This can challenge the ‘life-saving’ perception endorsed by patients, providers and police. However, consistent with previous research, this difference likely reflects the specification that police transport is reserved for patients with penetrating injuries, and in practice the vast majority of police-transported patients are injured in firearm assaults that result in serious, life-threatening injuries.11 18 44
Quantitative analyses revealed an uneven distribution of police and EMS transport across Philadelphia’s population indicating that refinement of police transport could further strengthen equitable access to care of injured patients across the city. Odds of police transport were not impacted by a neighborhood’s rate of aggravated assault (indicating violent activity), or narcotic arrests (indicating non-violent crime and policing activity). Rather, markers of concentrated disadvantage45 including the percentage of Black population and density of vacant housing units predicted police transport, as did although small, differences in drive times to definitive care (3.7-minute vs. 4-minute drive times) between places where police-transported patients were injured and places where EMS-transported patients were injured. We expected that neighborhoods with more fire stations would have lower rates of police transport, as EMS units deploy from fire stations. Our findings did not support this hypothesis. It is possible that these neighborhoods have increased rates of EMS calls, and thus lower actual availability of EMS units. Mismatches between community needs and resources may therefore lead to increased rates of police transport despite an overall higher number of fire stations in these neighborhoods.
When controlling for neighborhood characteristics, we found individual patient characteristics to be associated with police transport. Some of these, such as gunshot wound injury, decreased GCS, and hypotension, likely indicate appropriate triage of severely injured patients by officers on the ground. However, patients of Black race or Hispanic ethnicity were more likely to be transported by police, even when controlling for these characteristics. This may reflect underlying structural discrimination46 which limits EMS services and augments police transport as a result of the racial and ethnic composition of a neighborhood of residence and associated exposures to policing and police contact. In Philadelphia, where there are multiple level I trauma centers, the average transport times based on distance between a patient’s neighborhood of residence and the closest trauma center, comparing police and EMS-transported patients, are statistically different but relatively close. Recognizing the potential for structural disparities in transport based on neighborhood of residence, proximity to trauma centers, and distribution of police and EMS resources should be an implementation consideration, particularly in municipalities where there are few or poorly distributed hospitals equipped to provide definitive trauma care.4
Our qualitative analysis highlighted important issues across stakeholder groups. All groups agreed that speed of transport was an advantage but identified different trade-offs and implementation challenges. Consistent with our prior research, patients reported pain and a sense of risk during police transport,23 and were concerned that their injuries might have been worsened by transport in a vehicle not designed for injury care and stability. These concerns could be addressed by a combination of improved padding and safety restraints in police cars, by officers discussing these risks and benefits with patients in the moment, and by public education. Police identified concerns about exposure to bodily fluids and the ergonomics of lifting patients into police vehicles. Improved training for officers and improved availability of gloves and other personal protective and patient transport equipment could help address this challenge. Clinicians were concerned about disruptions to the flow of care at the trauma center, which could be addressed through institutional protocols and enhanced communication between police and the trauma center.
Both police and patients identified transport to a trauma center as a service police can provide at a critical time. For some, this kind of police–citizen interaction stood out as positive in an otherwise tense and polarized relationship between police and citizens in the city. This forefronts the potential for collaborative policy refinement incorporating police, community and provider perspectives. To this end, trauma systems should collect comprehensive data on patient transport and outcomes to guide quality improvement efforts and to enable comparative effectiveness research.17 23 24 47 Municipalities currently using police transport should examine and mitigate occupational health risks faced by police officers who carry out transport with specific attention to their exposure to blood and bodily fluid, and the physical safety and ergonomics of moving injured people to and from police vehicles. Finally, neighborhoods with the highest odds of police transport can be identified for enhanced EMS access and/or as a priority for training to improve transport practices among the police officers working in local districts. With optimized police transport practices, neighborhoods with the lowest odds of police transport could similarly be targeted to increase the availability of police transport and decrease prehospital time.
There findings of this study must be interpreted in the context of its several limitations. First, the PTOS registry only includes the zip code of residence for each patient. Though there is evidence that home addresses can proxy for location of injury in regional trauma system planning,35 there are likely some location data that are mis-specified48 in our analyses of intracity variation in hospital transport. Second, the regions of the city we compared are approximations of broad neighborhood boundaries, and additional variation may exist at a smaller scale. Finally, the findings of qualitative analyses may not represent stakeholders from other districts and trauma centers in the city or police transport in other cities where it is being implemented or considered for implementation. These limitations prompt several opportunities for future research. To understand the full range of perspectives of police transport implementation, future work should be inclusive of emergency medical technicians and paramedics in city EMS systems, patients transported to trauma centers by emergency medical technicians and paramedics, city policymakers, and uninjured city residents. There is also a need to identify and quantify the opportunity cost of police transport to understand what kind of police work and at what cost may be foregone when police are providing patient transport. Together with clinical outcome data, these multiple dimensions of police transport outcomes will enable a broader and more generalizable understanding of the effectiveness and equity of police transport as a core trauma system strategy.
Conclusion
Beyond its life-saving potential, police transport is viewed by patients, police, and clinicians as a generally beneficial police–citizen interaction. However, patients, police, and trauma clinicians also perceived disadvantages to current practice that can be targeted for improved training, supply, infrastructure and changes to policy implementation. This study presents significant demographic and geographic variations in the distribution of police versus EMS transport warranting greater attention to equity in intracity trauma care resource distribution, like EMS availability and trauma center access,6 across municipalities that choose to implement police transport as a central prehospital strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SFJ and EJK co-led this study and participated in all aspects of the study design, data collection, data analysis and article preparation. CCB and DNH participated in the study design and article preparation.
Funding This study was funded, in part, by the Penn Injury Science Center with support from the Centers for Disease Control and Prevention (R49CE002474).
Disclaimer The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention. This study was performed with the permission of Pennsylvania Trauma System Foundation, which specifically disclaims responsibility for any analyses, interpretations or conclusions.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study protocol was approved by the University of Pennsylvania Institutional Review Board (824456).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data collected from the US Census and the American Community Survey are publicly available. Data collected from the Philadelphia Police Department and Pennsylvania Trauma Outcomes Study through the Pennsylvania Trauma Systems Foundation are not publicly available but may be available based on application to these individual agencies. Research protocols and analytic plans may be available based on individual requests.