Article Text

Abstract
Background Discharge delays for non-medical reasons put patients at unnecessary risk for hospital-acquired infections, lead to loss of revenue for hospitals and reduce hospital capacity to treat other patients. The objective of this study was to determine prevalence of, and patient characteristics associated with, delays in discharge at an urban county trauma service.
Methods We performed a retrospective cohort study with data from Zuckerberg San Francisco General Hospital (ZSFGH), a level-1 trauma center and safety net hospital in San Francisco, California. The study included 1720 patients from the trauma surgery service at ZSFGH. A ‘delay in discharge’ was defined as days in the hospital, including an initial overnight stay, after all medical needs had been met. We used logistic and zero-inflated negative binomial regression models to test whether the following factors were associated with prolonged, non-medical length of stay: age, gender, race/ethnicity, housing, disposition location, type of insurance, having a primary care provider, primary language and zip code.
Results Of the 1720 patients, 15% experienced a delay in discharge, for a total of 1147 days (median 1.5 days/patient). The following were statistically significant (p<0.05) predictors of delays in discharge in a multivariable logistic regression model: older age, unhoused status or disposition to home health or postacute care (compared with home discharge) were associated with increased likelihood of delays. Having private insurance or Medicare (compared with public insurance) and discharge against medical advice or absent without leave (compared with home discharge) were associated with reduced likelihood of delays in discharge after all medical needs were met.
Discussion These results suggest that policymakers interested in reducing non-medical hospital stays should focus on addressing structural determinants of health, such as lack of housing, bottlenecks at postacute care disposition destinations and lack of adequate insurance.
Level of evidence Epidemiological, Level III
- health policy
- delivery of health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The adverse effects of delays in discharge—any days in the hospital spent after a patient has been medically cleared1—on patient health and hospital finance have major implications for the healthcare system. Patients who experience delays in discharge have higher mortality and morbidity2 because they are placed at unnecessary risk of hospital-associated deconditioning, delirium and hospital-acquired infections. Since inpatient surgical services are often not equipped to provide daily physical/occupational/speech therapy, delays in discharge can deny patients access to needed rehabilitate services.3 Delays in discharge strain hospital financial resources, because hospitals receive no reimbursements for custodial care.4 Such losses can routinely average in the thousands per day, leading a surgery department to lose millions of dollars of revenue annually.4 Longer lengths of stay are also associated with reduced profit for trauma centers.5 For example, one trauma center found delays in discharge increased the length of stay of trauma patients by about 5%, leading to a financial loss between $4 and $15 million.1 These kind of financial losses can be particularly challenging for surgery departments in urban safety-net hospitals that are often already under financial strain, due to the high costs that accompany trauma injuries and the number of patients with public health insurance coverage.6
Delays in discharge also pose a challenge for efficient allocation of health systems resources. Delaying discharge for medically stable patients decreases provider time spent with more acute patients, limiting the ability of surgeons to respond to traumas and potentially decreasing the overall quality of care. In the worst case, this may lead to hospitals going on divert, or not accepting new patients, contributing to increased patient morbidity and mortality.
Many types of factors contribute to delays in discharge. Structural factors include inadequate beds at nursing or rehabilitation discharge destinations,7 8 lack of insurance coverage,9 inadequate social worker staff10 and restricted weekend services.11 Interpersonal factors include communication breakdowns, conflicting goals between teams and services and teamwork problems.12 There is conflicting evidence over whether injury severity or comorbidities contribute to delays in discharge.7 8 Despite considerable research, surprisingly little is known about what patient factors, such as age or housing status, affect delays in discharge. This study sought to determine prevalence of, and patient characteristics associated with, delays in discharge at an urban county trauma service.
Methods
We conducted a retrospective cohort study of all patients admitted to the trauma service from 1 January to 31 December 2018, identified using the trauma registry at Zuckerberg San Francisco General Hospital (ZSFGH). The trauma registry includes all patients admitted with traumatic injury and excludes patients who activate a trauma protocol and are discharged from the emergency room. ZSFGH is the only level 1 trauma center for the city and county of San Francisco.
We defined ‘delay in discharge’ as days spent on the ‘lower level of care service’, a census at ZSFGH for patients who are medically cleared from the inpatient trauma service yet awaiting discharge. When on this census, patients receive care equivalent to a ‘lower level’ than a hospital inpatient surgery unit. At ZSFGH, patients are reviewed daily by a team of physicians, nurse practitioners, pharmacists and social workers who determine if a patient should be transferred to the ‘lower level of care’ census. Within the ‘lower level of care’ census are several subcategories, corresponding to different intensities of care and reimbursement. These range from ‘custodial care’, for which the trauma services receives $0/day, to ‘Skilled Nursing Facility’ (SNF) level of care, the highest reimbursement level. While on this census, patients may receive wound care from nursing staff and physical therapists but are not included in daily rounds by the inpatient trauma service. Rehabilitation care is limited by staffing, as ZSFGH is designed primarily as an inpatient service rather than an SNF or formal rehabilitation facility.
We analyzed the following patient factors: age, gender, race/ethnicity, housed versus unhoused status, type of insurance, primary language, discharge location and whether a patient had a primary care provider. For several categories, we grouped variables in order to achieve a sample size sufficient for analysis. Groupings were as follows: ‘Native American’, ‘Hawaiian/Pacific Islander’ and ‘Other’ as ‘Other Race’; all non-English languages as ‘Non-English’; all insurance plans that were not classified as ‘Medical’, ‘Medicare’, ‘Private’ or ‘San Francisco Health Plan’ as ‘Other Insurance’; ‘Skilled Nursing Facility’, ‘Rehabilitation Facility’, ‘Board and Care’ and ‘Long Term Care’ as ‘Post-Acute Care Discharge Facility’.
We tested for univariate associations between each patient characteristic and the binary delay in discharge variable using t-tests for continuous variables and χ2 or Fisher’s exact tests for categorical variables. Factors associated with delays in discharge at the p<0.1 level in univariate tests were entered into univariate and multivariable logistic regression models, and a zero-inflated negative binomial regression model to test for associations with the number of days delayed (taking into account the likelihood of a delay in discharge). We tested for model specification errors, for collinearity using variance inflation factors and for goodness of fit using a Hosmer-Lemeshow test. We chose the zero-inflated negative binomial model over a zero-inflated Poisson or non-zero-inflated models based on visual and likelihood ratio test comparisons. We considered p<0.05 to be statistically significant. All analyses were performed using Stata V.16.0.13
Results
Over the 1-year study period, 1720 patients were discharged from the trauma surgery service at ZSFGH. Characteristics of patients who did and did not experience delay in discharge are presented in table 1. The mean patient age was 49.6 years old (range 18–118), 62% were male, 18% were unhoused and 54% used Medicaid or San Francisco Health Plan (a public health access plan for uninsured residents of San Francisco) as their primary form of coverage.
Age, housing status, insurance and discharge location were associated with increased risk of delay in discharge
A total of 261 patients (15%) experienced a delay in discharge, with a median delay of 2 days (range 1–45). Of the patients who experienced a delay in discharge, 89% experienced a delay of 1 week or less. Factors associated with delays in discharge in univariate analysis were older age, unhoused status, insurance status and discharge location (table 1).
Univariate and multivariable logistic regression analyses (table 2) revealed that older age, unhoused status and discharge to a postacute care destination (SNF, rehabilitation, board and care, and long-term care) or to home health were all significantly and independently associated with increased likelihood of delays. In contrast, having private insurance or Medicare, discharge against medical advice and discharge as absent without leave were independently associated with decreased likelihood of delays in discharge. We tested for interactions between variables, none of which were statistically significant. A link test was used to detect specification error, which was not significant, and there was also no evidence of collinearity according to variance inflation factors (all were <6). A Hosmer-Lemeshow test indicated a good fit to the data.
ORs and 95% CIs for patients the odds of experiencing delays in discharge, from univariate and multivariate logistic regression models
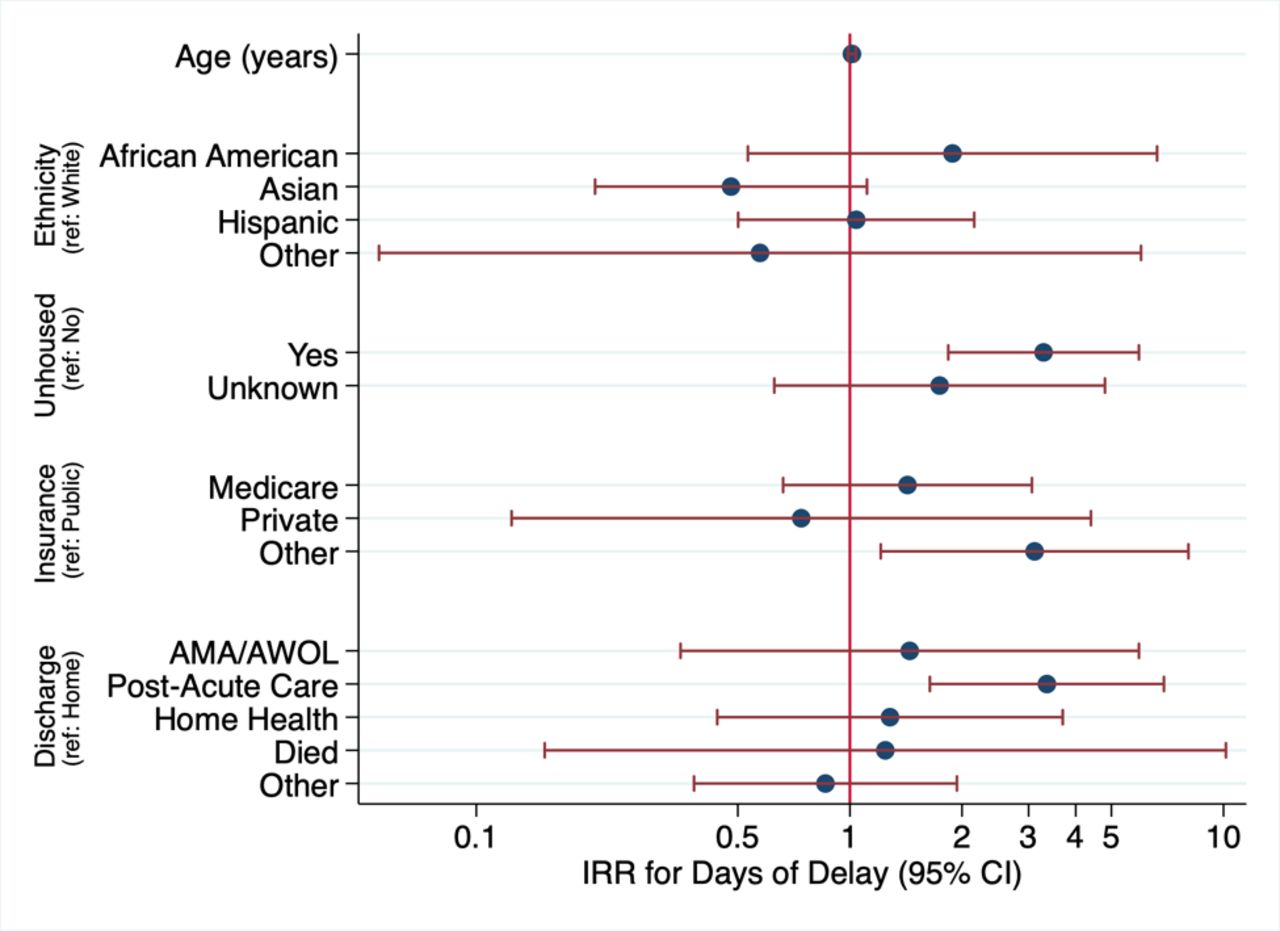
Finally, we conducted a multivariable zero-inflated binomial regression analysis with the same variables that were used in the logistic regression models as predictors of both the odds of any delay in discharge and the of the incidence rates for number of days delayed (figure 1). The incidence rate ratios for number of days of delay in discharge were consistent with the results of the logistic regression in that older age and homelessness were significantly associated with longer delays. In addition, having non-Medicare and non-private insurance was associated with longer delays compared with those on public insurance, and being discharged to postacute care was also independently associated with longer delays in discharge compared with patients discharged to home.
{kind=link}
Incidence rate ratios (IRRs) and 95% CIs are estimated from the count portion of a multivariable zero-inflated negative binomial regression model (all variables were included in the binary portion of the model). AMA, against medical advice; AWOL, absent without leave.
Discussion
In this study, we found that patients experiencing delays in discharge were more likely to be older, unhoused and discharged to a postacute care or home health facility. Patients with private insurance or Medicare were less likely to experience a delay in discharge.
Our findings are consistent with those from other studies that found systems issues—such as affordable housing, insurance coverage or bottlenecks in discharge destinations—are the main driver of excessive length of stay, rather than severity of illness.7 14 15 Although several studies found that severity of trauma is associated with delays in discharge,7 8 16 this relationship is likely correlative rather than causal, because increased illness severity is associated with disposition to SNF or a rehabilitation facility.14
Discharge destinations for unhoused patients are sparse and often unsafe. According to one study in an academic medical center, 27% of unhoused patients were discharged after dark and 11% reported sleeping on the street on the first night of discharge.17 In general, unhoused individuals experience much higher rates of assault and violence and emergency shelters offer little privacy, stability or resources for physical rehabilitation.18 Medical respite programs, designed to provide care to unhoused individuals too sick for shelter but too healthy for the hospital, have been shown to reduce hospital readmissions and improve housing outcomes.19 Yet, San Francisco has only 75 medical respite beds for a homeless population over 8000,20 21 leading to wait times that can exceed several weeks. Rehabilitation facilities also have long wait times. Nationally, private payments for nursing homes have risen more quickly than inflation, suggesting a growing shortage.22
Insurance coverage can contribute to delays in discharge as well.9 23 California has one of the lowest Medicaid reimbursement rates in the USA, which disincentivizes postacute care facilities, such as SNFs, from accepting patients on Medicaid.24 Unlike other patients at our safety net institution, who are predominantly on public insurance, trauma patients have diverse insurance plans since they have little control over where they are admitted. We found patient with private insurance had a lower chance of experiencing delays in discharge, reflecting higher reimbursement rates.
Zip code of residence had no significant effect on likelihood of experiencing a delay, suggesting that coordinating with geographically distant discharge destinations did not increase the chance of experiencing a delay. We were surprised by this finding because discharge criteria can vary by postacute care facility and county, and the San Francisco Health Plan only provides coverage within the boundaries of San Francisco. One possible explanation is social work and case manager staff at our institution may be sufficiently familiar with the requirements of geographically distant discharge destinations.
Our findings point out the need for increased investment in postacute care centers and affordable housing. Such investments are particularly critical in light of the COVID-19 pandemic, which is projected to increase strain on discharge destinations and hospital beds.25 In anticipation of growing COVID-19 cases, many hospitals have attempted to increase their bed capacity by safely discharging patients and canceling non-emergent procedures.26 Reducing delays in discharge allows hospital beds, an increasingly precious resource,27 to be used more efficiently. By decreasing delays in discharge, investments in postacute care centers and affordable housing are also likely to reduce recovery times, risk of hospital acquired infections and overall patient morbidity.2
Our study has several important limitations. Although our findings are consistent with research conducted in other settings,7 15 we only studied delays in discharge at a single institution, which may limit the generalizability of our results. In addition, the number of unhoused patients is likely under-represented because patients with ‘unknown’ housing status were considered housed. Furthermore, we did not collect information on the prevalence of marginally housed patients. Although prior research has suggested that injury severity does not contribute to delays in discharge,8 we did not consider medical diagnosis in our analysis. Transfer from the inpatient trauma service to the ‘lower level of care’ service was a decision made by a multidisciplinary care team, and although there were predetermined criteria for transfer, team members rotate on the service, introducing personal variability on how criteria were applied. This may also underestimate delays in discharge, given staff had to make a decision to transfer a patient from the inpatient census to the lower level of care census. Finally, we did not analyze the financial impact of delays in discharge. However, the average reimbursement rate for a hospital day at ZSFGH is $2700, and days spent on the lower level of care service reimburse at only a fraction of that rate (as low as $0/day for patients remaining in the hospital for only behavioral observation). With 1147 total patient days delayed in 2018, the total opportunity cost of discharge delays is likely on the order of millions of dollars.
In conclusion, our results suggest that older patients, unhoused patients, patients with MediCaid or San Francisco Health Plan and patients discharged to a postacute care facility were more likely to experience a delay in discharge. Policymakers should seek to address the root causes of delays in discharge. Efforts to reduce delays in discharge should be directed to addressing homelessness, lack of adequate insurance and investing in increased availability of postacute care rehabilitation beds.
References
Footnotes
Contributors CC and KL: data analysis, manuscript preparation and editing. TB: study conception, data analysis, manuscript preparation and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study (IRB # 19–27433) consisted of secondary analysis of non-identifiable patient data and was deemed exempt by the University of California San Francisco (UCSF) Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data analyzed from drawn from the San Francisco General Trauma Registry, which includes all trauma admissions during the 2018 calendar year. Patient data are deidentified and are available on reasonable request.