Article Text

Abstract
Background Trauma management requires a multidisciplinary approach, but coordination of staff and procedures is challenging in patients with severe trauma. In October 2014, we implemented a streamlined trauma management system involving emergency physicians trained in severe trauma management, surgical techniques, and interventional radiology. We evaluated the impact of streamlined trauma management on patient management and outcomes (study 1) and evaluated determinants of mortality in patients with severe trauma (study 2).
Methods We conducted a retrospective cohort study of 125 patients admitted between January 2011 and 2019 with severe trauma (Injury Severity Score ≥16) and persistent hypotension (≥2 systolic blood pressure measurements <90 mm Hg). Patients were divided into a Before cohort (January 2011 to September 2014) and an After cohort (October 2014 to January 2019) according to whether they were admitted before or after the new approach was implemented. The primary outcome was in-hospital mortality.
Results Compared with the Before cohort (n=59), the After cohort (n=66) had a significantly lower in-hospital mortality (36.4% vs. 64.4%); required less time from hospital arrival to initiation of surgery/interventional radiology (median, 41.0 vs. 71.5 minutes); and was more likely to undergo resuscitative endovascular balloon occlusion of the aorta (24.2% vs. 6.8%). Plasma administration before initiating hemostasis (adjusted OR 1.49 (95% CI 1.04 to 2.14)), resuscitative endovascular balloon occlusion of the aorta (9.48 (95% CI 1.25 to 71.96)), and shorter time to initiation of surgery/interventional radiology (0.97 (95% CI 0.96 to 0.99)) were associated with significantly lower mortality.
Discussion Implementing a streamlined trauma management protocol improved outcomes among hemodynamically unstable patients with severe multiple trauma.
Level of evidence Level III.
- multiple trauma
- shock
- hemorrhagic
- hemostasis
- endovascular procedures
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Uncontrolled hemorrhagic shock is an important cause of death among trauma patients.1 Recently, trauma management has markedly improved due to rapid advances in medical techniques such as CT and procedures such as interventional radiology (IR),2 3 including resuscitative endovascular balloon occlusion of the aorta (REBOA) and damage control strategies.4 A multidisciplinary approach is required in current trauma management,5 but it is challenging to completely perform coordination of staff and procedures for severe trauma. In October 2014, we implemented a streamlined trauma management system involving trained emergency physicians (TEPs) specialized in emergency medicine and general surgery who were also trained in cardiovascular surgery and IR.6
We evaluated the impact of the streamlined trauma management protocol on patient management and outcomes among hemodynamically unstable patients with severe multiple injuries. Our secondary objective was to evaluate the determinants associated with in-hospital mortality among hemodynamically unstable patients with severe multiple injuries.
Methods
Development of a streamlined trauma management team
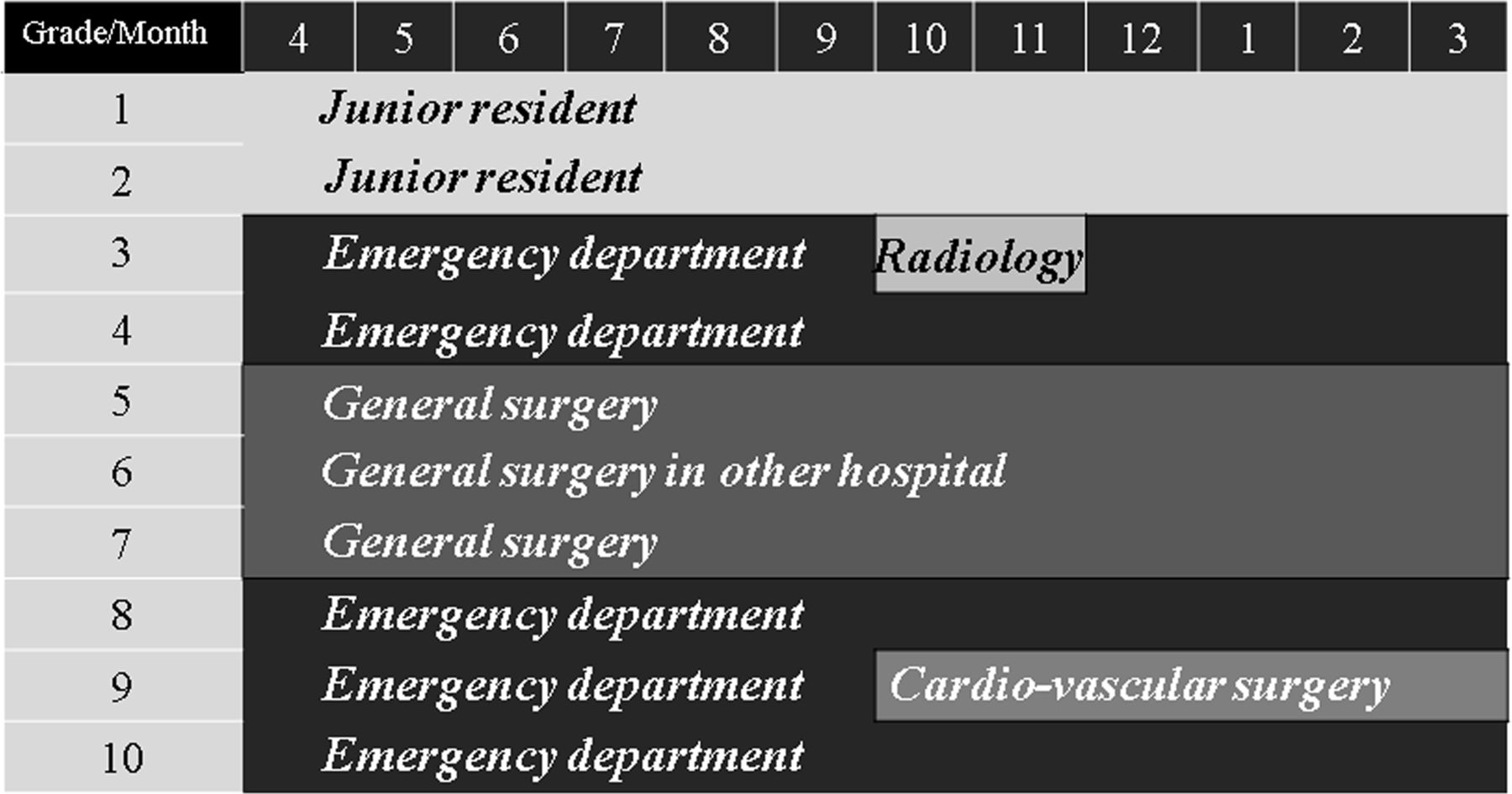
The TEP education curriculum is shown in figure 1. The training program was started in 2006, but has been revised subsequently. The TEPs were taught trauma management, including both surgical and interventional techniques in emergency medicine, radiology, general surgery, and cardiovascular surgery. The TEPs received triple board certifications in Japanese Association for Acute Medicine, Japan Surgical Society, and vascular IR at the Tokai University School of Medicine for which the rules for receiving the certification are as follows: 154 cases or more, with at least 2 years of experience, and one or more publications regarding IR. To complete these requirements a trainee would have at least 350 elective or emergency cases/3 years in general surgery, at least 154 IR cases/2 months in radiology or 2 years in an emergency department (ED), and at least 120 cardiovascular cases/6 months in cardiovascular surgery. Once they had completed all these requirements, they received board certification from the Japanese Society for Acute Care Surgery. Eventually, there were three or four trainees and two or three instructors in our ED.
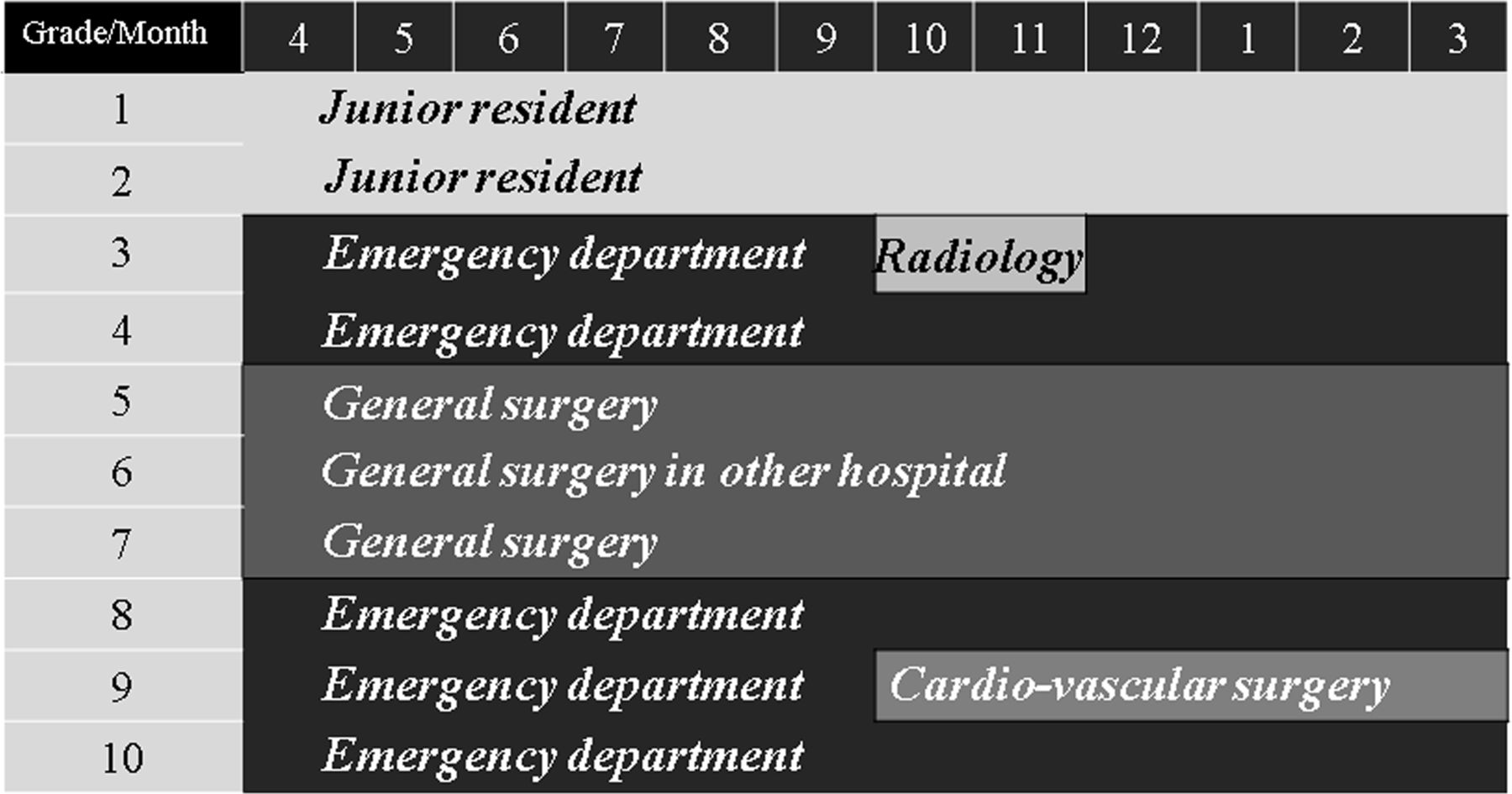
Training curriculum. Emergency physicians were trained in emergency medicine, radiology, general surgery, and cardiovascular surgery. In the emergency department, they were responsible for the initial management, anesthesia, surgery, and endovascular treatment of hemodynamically unstable patients with severe trauma, using the techniques that had been taught during their rotation through the radiology, general surgery, and cardiovascular surgery departments. Moreover, trained emergency physicians (TEPs) have handled hemodynamically stable torso-trauma patients and some hemodynamically unstable non-trauma patients who required surgical or interventional treatment. We evaluated each trainee’s competency based on their management of cases in our emergency department.
There are three or four emergency physicians (EPs) on duty in our ED at any time. Since October 2014, there has been at least one TEP working during each shift. The TEP is in charge of managing all types of severe trauma from start to finish. For example, patients with life-threatening trauma can be admitted directly to the operating room in the ED, enabling them to undergo trauma anesthesia and surgery performed by the TEPs as soon as possible. In patients undergoing CT, it is possible to decide on the treatment strategy immediately, based on the CT findings. It is also possible to change strategies from IR to surgery and vice versa, on a case-by-case basis.6
In the original system, EPs served as the primary doctors of hemodynamically unstable patients with multiple injuries and called on multiple specialists to assist with the management. The EPs or specialists made decisions regarding interventions and investigations. Similarly, multiple specialists performed the procedures. However, after the streamlined system was implemented, the TEPs made decisions regarding interventions and investigations and performed all the procedures seamlessly. The differences in decision-making and practice between the original (Before) and streamlined (After) management systems are shown in figure 2.

Difference in decision-making and practice for initial management between the original trauma management system and the streamlined trauma management system. EPs, emergency physicians; IR, interventional radiology; REBOA, resuscitative endovascular balloon occlusion of the aorta; TEPs, trained emergency physicians.
Importantly, the TEPs have implemented a training simulation and have created a suitable environment for severe trauma management routinely, with EPs, nurses and paramedics.
Study design and patient selection
This retrospective cohort study evaluated severe trauma patients (Injury Severity Score (ISS) ≥16) who were admitted to our hospital between January 2011 and January 2019. The inclusion criteria were systolic blood pressure (SBP) <90 mm Hg on arrival (preadmission and at admission), no cardiopulmonary arrest at admission, and non-traumatic cardiac arrest. Of the 6699 patients identified, including 721 patients who underwent emergency surgery or IR, 427 were included in the analysis. Further, we selected 125 patients who displayed persistent hypotension (≥2 SBP values <90 mm Hg) regardless of primary resuscitation (airway management, massive transfusion of at least two units of blood, and/or reversal of obstructive shock) to evaluate this trauma management system (figure 3).

{kind=link}
{kind=link}
{kind=link}
Patient inclusion flowchart and cohort assignment. ISS, Injury Severity Score; SBP, systolic blood pressure.
Study 1
The patients were divided into two cohorts according to the date of admission: Before (January 2011 to September 2014) and After (October 2014 to January 2019).
The primary outcome was in-hospital mortality. We set several secondary outcomes to evaluate the effectiveness of the new trauma management system including the 24-hour mortality, mortality owing to exsanguination, survivors with probability of survival calculated by the Trauma and Injury Severity Score (TRISS-PS) <25%, prehemostasis CT scan performance ratio, transfusion of red blood cells (RBCs), and fresh frozen plasma (FFP), FFP:RBCs, the proportion of patients who underwent REBOA; the time from arrival to initiation of hemostasis, the number of patients who underwent IR as primary hemostasis (PH), the amount of blood transfused, massive transfusion (≥10 units of RBCs within the first 24 hours), and FFP:RBCs within the first 24 hours.
Study 2
Using a retrospective cohort design, we evaluated the primary determinants of in-hospital mortality using multivariable logistic regression of the whole cohort.
Data collection
The following data were collected from electronic medical records: Glasgow Coma Scale score at admission, respiratory rate, SBP, body temperature, pulse rate, blood pH, base excess, lactate level, D-dimer level, prothrombin time-international normalized ratio, and time taken to initiate hemostasis. The Revised Trauma Score (RTS), Abbreviated Injury Scale, ISS, and the TRISS-PS were used to determine the severity of the patients’ injuries. Data were collected on the total volumes of RBCs and FFP transfused in the first 24 hours, and before initiation of urgent hemostasis, the total volume of platelets transfused in the first 24 hours, and whether patients had been given a massive transfusion. All patients were followed up to the time of discharge or death, whichever occurred first. The outcome measures were 24-hour survival from the time of admission and survival to discharge, mortality owing to exsanguination, and survivors with TRISS-PS <25%.
Statistical analysis
Categorical variables were compared using χ2 tests or Fisher’s exact tests, whereas continuous variables were compared using Student’s t-test or the Mann-Whitney U test, as appropriate. Data were reported as means and SDs or as medians and IQRs, as appropriate. Multivariable logistic regression, adjusted for age, RTS, and ISS, was used to determine the effect of transfusions before initiation of urgent hemostasis, REBOA, and time from arrival to initiation of surgery/IR on in-hospital mortality. The statistical analyses were performed using SPSS V.25.0 for Windows (IBM). Statistical significance was defined as a p<0.05.
Results
Study 1
The Before and After cohorts included 59 and 66 patients, respectively. Table 1 summarizes the patient characteristics. Patients in the After cohort had significantly more severe trauma than those in the Before cohort in terms of ISS and TRISS-PS.
Patient characteristics according to the date of hospital admission
Table 2 shows the outcomes. Compared with the Before cohort, patients in the After cohort had a significantly lower 24-hour mortality rate and in-hospital mortality rate; were significantly less likely to die due to exsanguination; had significantly more survivors with TRISS-PS <25%; had a significantly shorter time from arrival to initiation of surgery/IR; were significantly more likely to undergo REBOA before PH; were significantly more likely to receive RBCs and FFP before PH; and had significantly higher FFP:RBCs administered before initiating hemostasis and in the first 24 hours, but there was no significant difference between the cohorts in the total number of blood transfusions in the first 24 hours.
Patient management and outcomes according to the intervention period
Study 2
Table 3 shows the results of the multivariable logistic regression analysis. Plasma administration before the initiation of hemostasis, REBOA, and time to initiation of surgery/IR were associated with significantly lower mortality.
Primary determinants of in-hospital mortality
Discussion
This study revealed that in hemodynamically unstable patients with multiple severe trauma, the streamlined trauma management system staffed by TEPs enabled earlier massive transfusions (with a target ratio of plasma:platelets:RBCs of 2:1:2), greater use of REBOA, and shorter time to initiation of both surgical and interventional radiological hemostasis than original management. The reduction in mortality is likely to be attributable to early plasma administration, greater use of REBOA, and earlier surgery and IR.
Early plasma administration has been widely used in trauma resuscitation.7 The use of a balanced transfusion may lessen trauma-induced coagulopathy and endothelial injury.8 9 The Prehospital Air Medical Plasma trial demonstrated that compared with standard care resuscitation, prehospital plasma administration lowered the 30-day mortality of severely injured patients at risk of hemorrhagic shock.10 By contrast, plasma-first resuscitation to treat hemorrhagic shock during emergency ground transportation was not associated with reduced mortality among trial participants in urban areas, suggesting that plasma misuse might lead to wastage of medical resources.11 Transfusion strategies of high plasma to RBC and platelet/RBC ratios did not have survival benefits but were associated with an increase in adverse events.12 REBOA is also an important approach in trauma and emergency medicine,3 13 14 but the use of plasma and REBOA for trauma remains controversial. Some large studies have shown a higher mortality rate in severely injured trauma patients who underwent REBOA than in those who did not.15 16 It is unclear which patients are likely to benefit from early plasma administration or REBOA.11 15
The time from hospital arrival to the initiation of hemostasis is critical for improving survival in patients with multiple traumatic injuries.17 Further, a delay in laparotomy in patients with intra-abdominal hemorrhage after trauma is associated with higher mortality.18 One study also reported that earlier time to hemostasis is associated with lower mortality and rate of complications.19 Thus, early hemostasis is crucial. However, it is challenging to perform surgery and/or IR immediately and faultlessly in an appropriate order in hemodynamically unstable patients with severe multiple trauma.
To address this issue, we created a streamlined trauma management system that is run by TEPs. TEPs are experienced in trauma-based specialties,6 which are not limited by the anatomic location,20 21 therapeutic approach,6 20–23 or the in-hospital environment.20 23 Trauma anesthesia during surgery and/or IR in the ED is also performed by TEPs. Although many studies have reported adverse outcomes from early plasma administration or REBOA,11 12 15 16 our TEPs were able to use them effectively. Compared with the original management system, the streamlined management system staffed by TEPs might enable earlier identification of patients with life-threatening trauma. This, in turn, would enable more optimal patient selection for both surgery and IR while deciding on the necessity of early administration of blood transfusions and aortic clamp before cardiac arrest.6 24 Furthermore, the TEPs could perform all necessary modalities, such as the conversion of one form of treatment to another and management of all complications.20–22 They also prevented the need for unnecessary invasive procedures, leading to good functional prognoses.21 22 Taken together, the streamlined management system might enable more effective and rapid utilization of a hybrid environment. The standardization of such competencies could help improve the quality of care for trauma patients.
Resuscitation with percutaneous angiographic treatments and operative resuscitations have been recently reported to be effective.25 Furthermore, the survival benefit of a workflow using a hybrid emergency room (HER) system has been demonstrated.26 We think that such competencies would be effectively performed using a hybrid operating room (HOR) or HER. Although there are some reports regarding acute care with IR performed by trained acute care specialists or acute care surgeons,27 28 few studies have evaluated the effectiveness of similar trauma management protocols.
Only a few patients could benefit from the utility of HOR or HER.29 Moreover, REBOA can result in changes in the management of hemodynamically unstable patients with multiple injuries. Further studies are needed to confirm the optimal management strategy for severe trauma, including the appropriate physician, use of HOR or HER, and cost-effectiveness ratio. Ideally, the relative effectiveness of different interventions should be evaluated in randomized controlled trials (RCTs).
This study had several limitations. First, it was a single-center retrospective study with a small sample size. Although our results were obtained using careful patient selection, the number of patients could have been higher. Second, only 14 patients had penetrating trauma. Therefore, there may be a selection bias. However, we did not exclude patients with penetrating trauma because, in hemodynamically unstable patients with multiple severe injuries, it is sometimes difficult to determine whether the mechanism of the injury was blunt or penetrating. Third, medical equipment and techniques have progressed substantially during the study period. Fourth, although most characteristics were similar between the cohorts, the Before cohort had a significantly lower ISS than the After cohort. As reported previously,30 the ISS in the Before cohort is more likely to have been underestimated because more patients died owing to exsanguination with no diagnosis in the Before cohort. Alternatively, the higher ISS in the After cohort may be partially attributable to improvements in the preadmission management of out-of-hospital impending cardiac arrests that enabled more individuals to survive long enough to be admitted to the hospital. However, the reason for the difference in the ISS between the cohorts is unclear. Fifth, the 64.4% in-hospital mortality in the Before cohort is extremely high. If the ISS was underestimated in the Before cohort, the trauma severity in both cohorts might have been more similar than it appears, and the TRISS-PS in the Before cohort may have been similar to those in the After cohort. Thus, the in-hospital mortality in the Before cohort may not be a poor result. Alternatively, the higher mortality in the Before cohort may have been partially attributable to decision-making failures and poor coordination between the multiple specialists responsible for patient management before the streamlined system was introduced. However, the actual reason for this very high in-hospital mortality in the Before cohort remains unclear. Further studies, such as RCTs, are needed to address these issues. Last, there are some problems within the system. The standard general surgeons, interventional radiologists, cardiovascular surgeons, and anesthesiologists could not be trained for trauma management. The maintenance and improvement of TEPs’ skills could become difficult if the number of cases of severe trauma decreases. In the future, a cooperative agreement with the trauma care department should be developed to address this problem.
In conclusion, compared with the original management system, the streamlined trauma management system improved outcomes in hemodynamically unstable patients with severe multiple injuries, enabling earlier administration of transfusions, more use of REBOA, and shorter time to initiation of surgery and IR. Plasma administration before the initiation of hemostasis, use of REBOA, and early initiation of surgery and IR were significantly associated with lower mortality. These results confirm that the streamlined trauma management system is beneficial for multidisciplinary management in patients with severe trauma.
References
Footnotes
Contributors HO wrote the main article. HO and HA prepared the tables. AU and TS prepared the figures. HO, NS, TS, KS, HA, TY, SIi, and SIn contributed to the creation of the strategy for trauma resuscitation in practice. All authors reviewed and approved the final draft of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The protocol for this research project has been approved by the Tokai University Institutional Review Board for Clinical Research (approval number: 18R-326).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable. The datasets in this study are available from the corresponding author on reasonable request.